Apex
Abnormalities
| Atul Jaidka |
Case
Anatomy
Normal Anatomy
- Apical thinning
- Trabeculations
- False cords/tendons
Imaging
- Seen best in the apical windows (4/2/3) and parasternal short axis
- Imaging greatly improved with contrast
LV Tumour/Endocarditis
will skip, covered recently
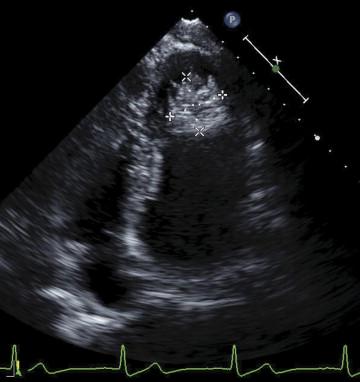
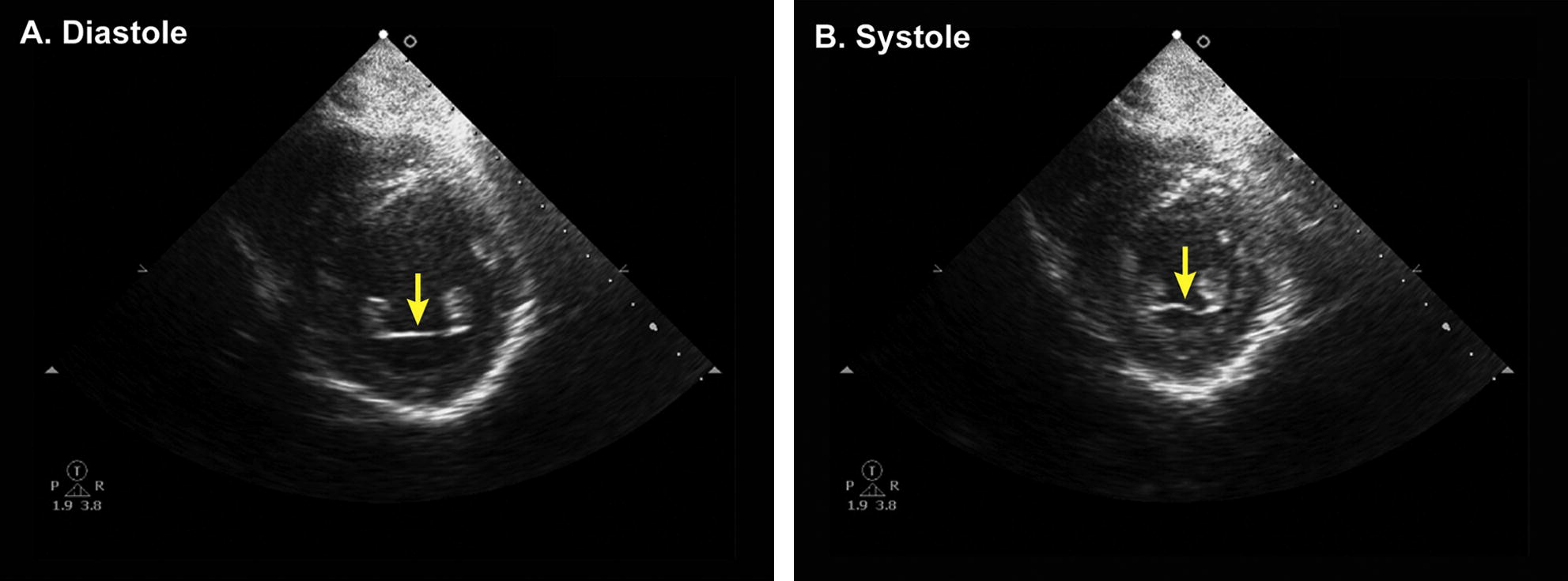
LV Thrombus
Features:
- regional wall motion abnormality
- apical location
- distinct margin with jagged edges
- movement separate from the underlying endocardium
- higher echo density as compared with the myocardium
Mimic
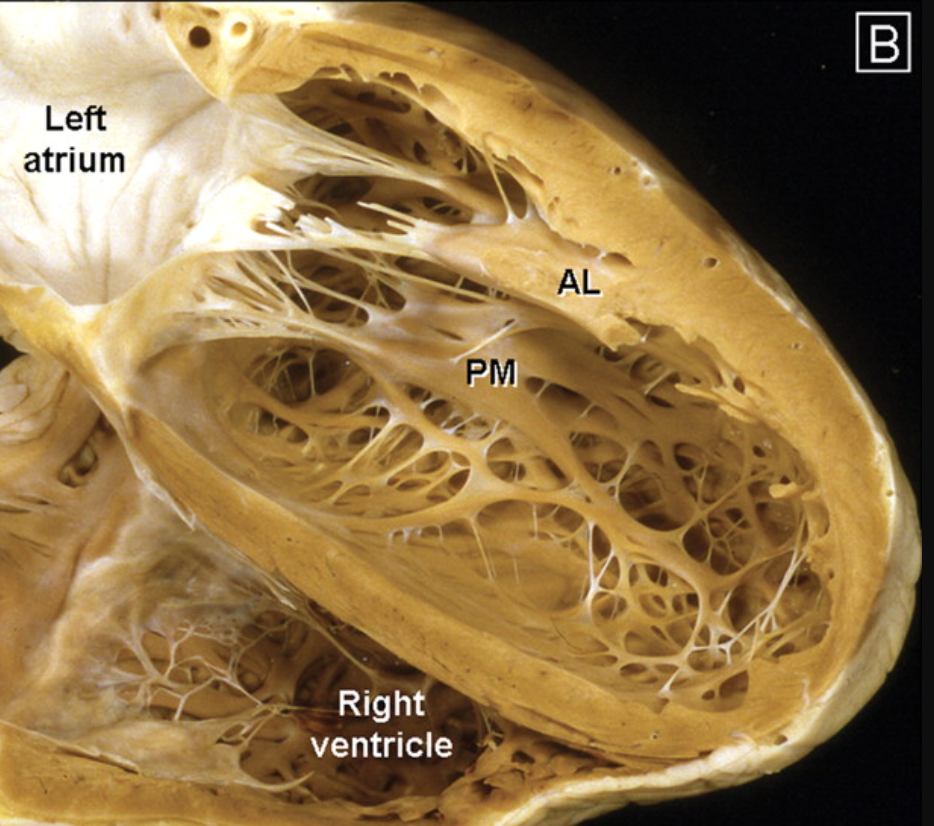
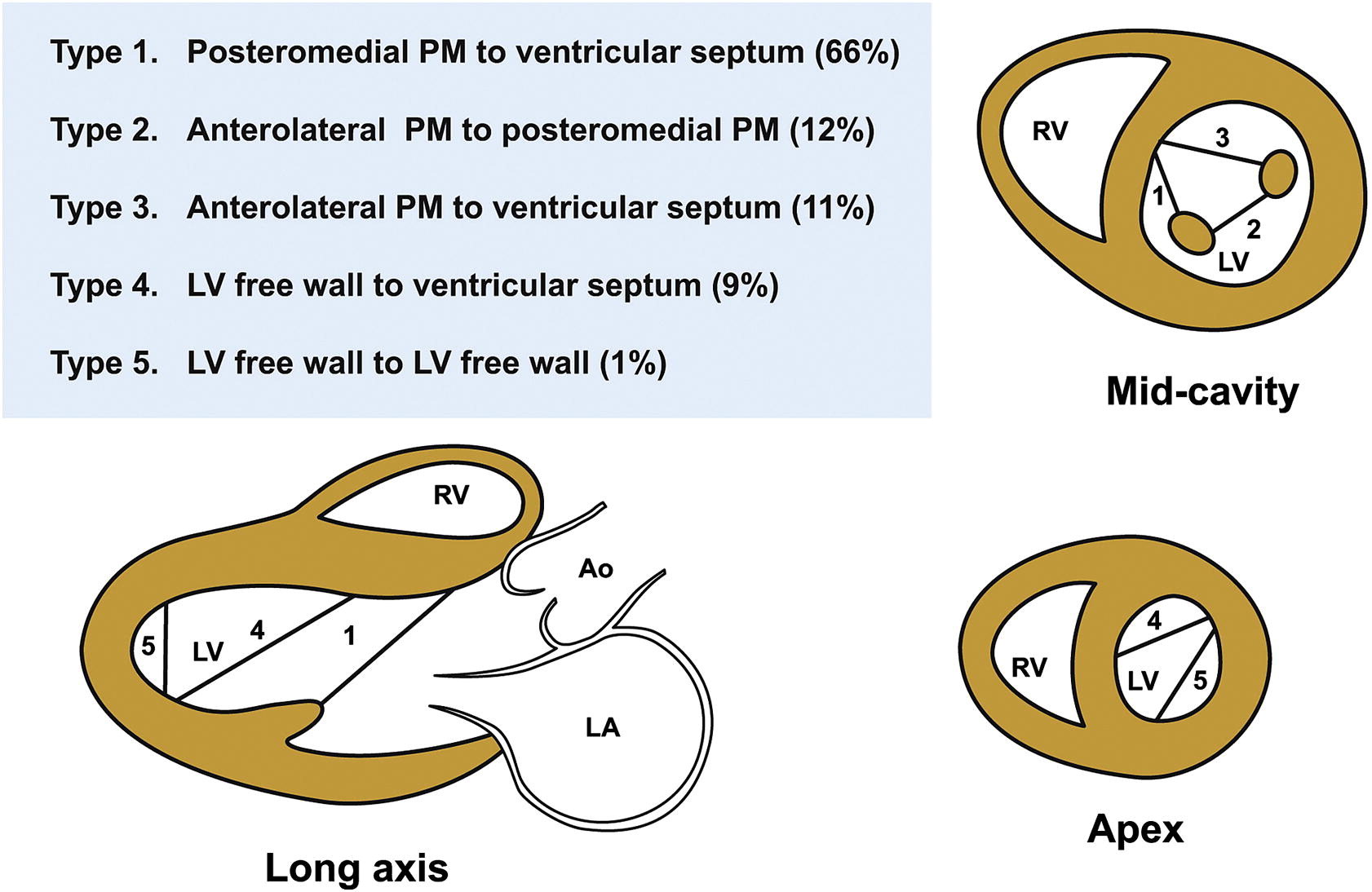
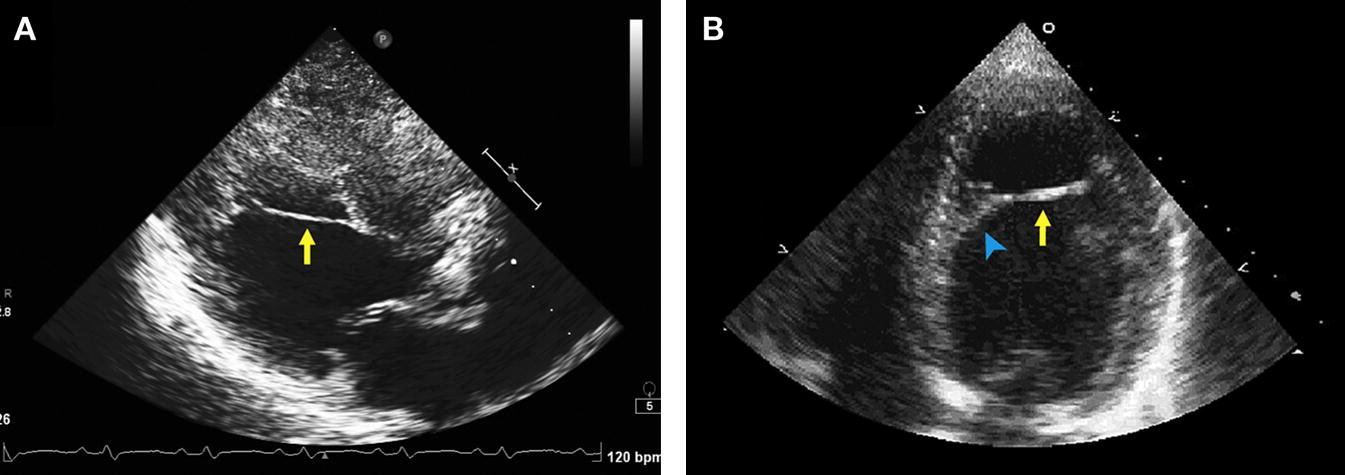
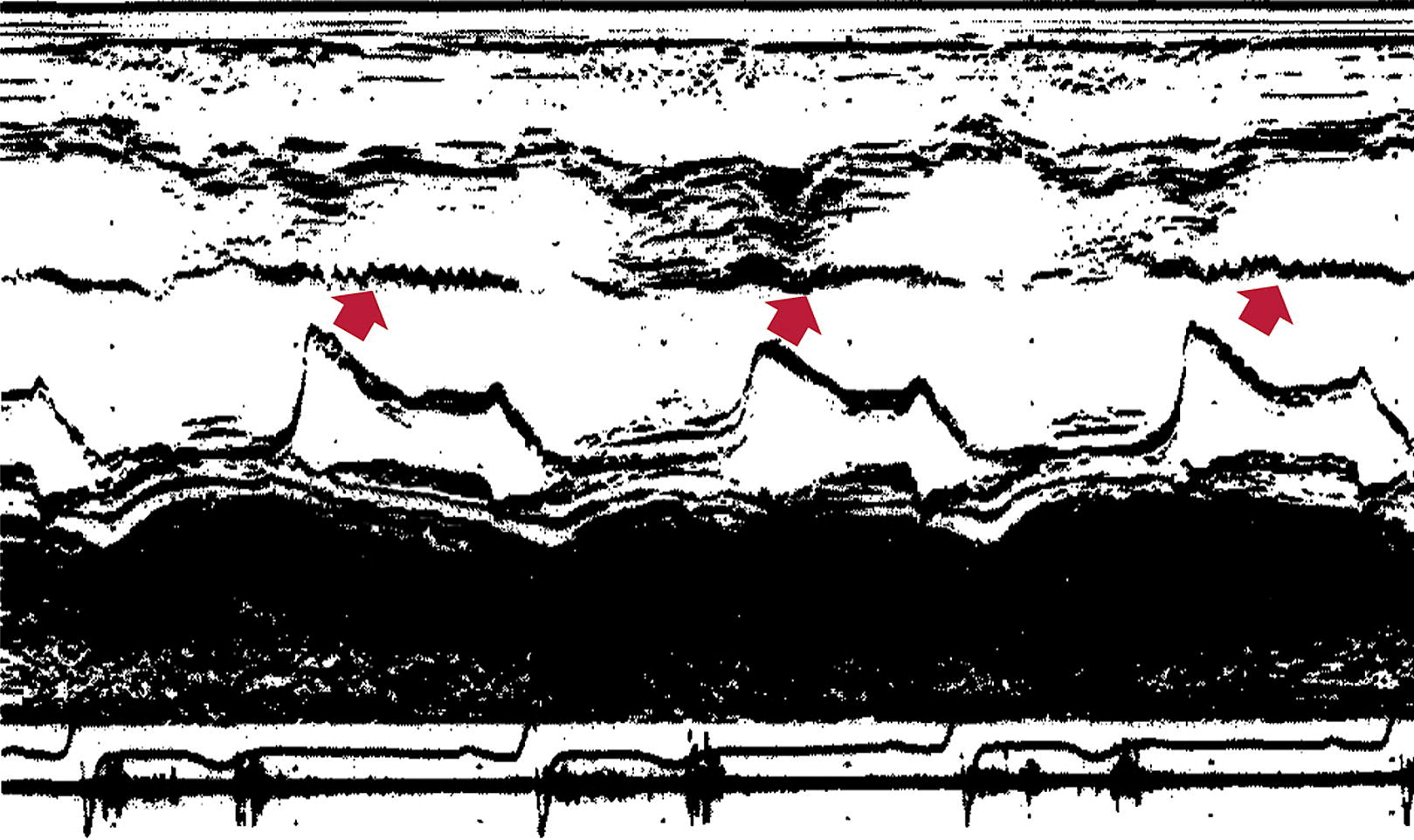
False Tendon
- Found in over 50% of LV in autopsy studies
- Unlike trabeculations, they traverse the LV cavity
- Echo free space on both sides
- Taut in diastole, laxe in systole
- Can have broad base attachment
- Can rupture in MI or spont
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731713001764?via%3Dihub
LV Bands
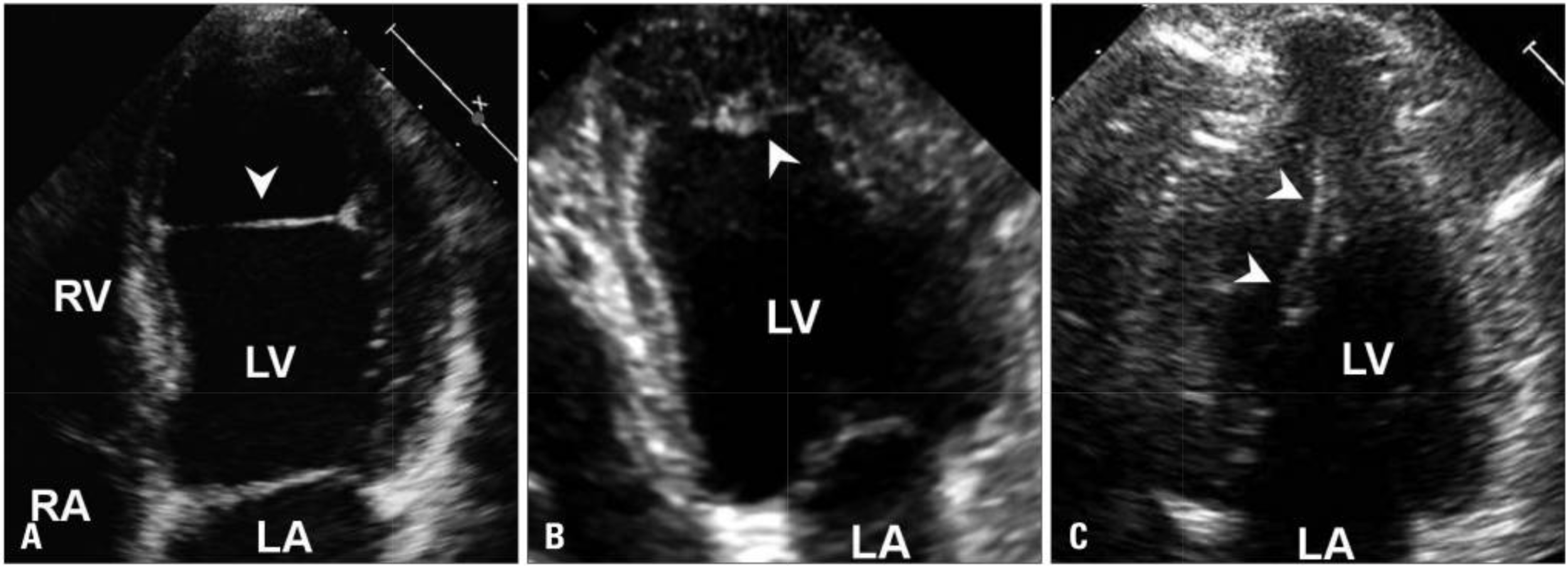
False Tendon
Muscular Band
Papillary Muscle
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3816159/
https://www.sciencedirect.com/science/article/pii/S2468644120300931
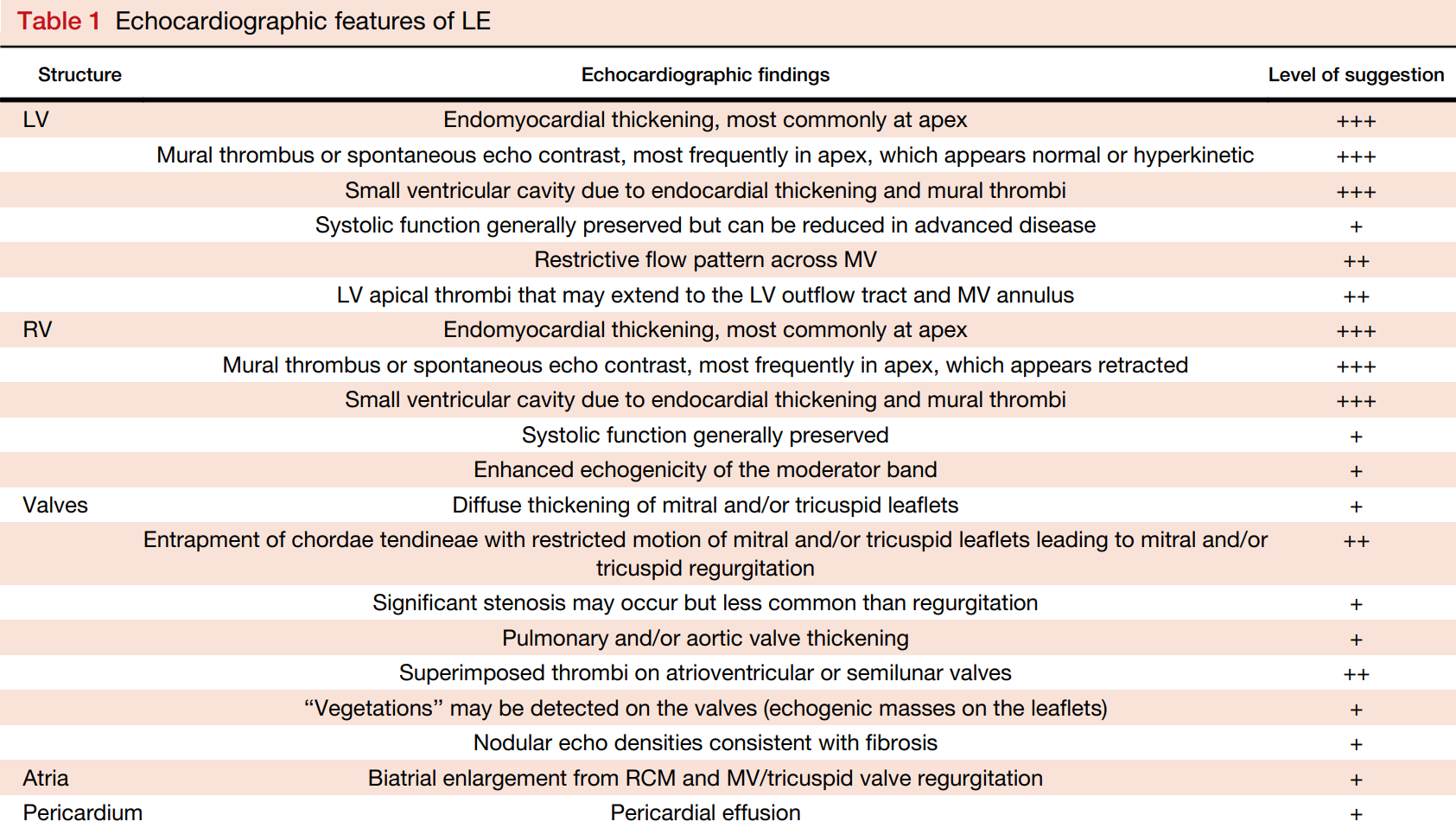
Loefflers
- 3 stages: necrotic (generally cannot see on TTE), thrombotic, and fibrosis (restriction and HF)
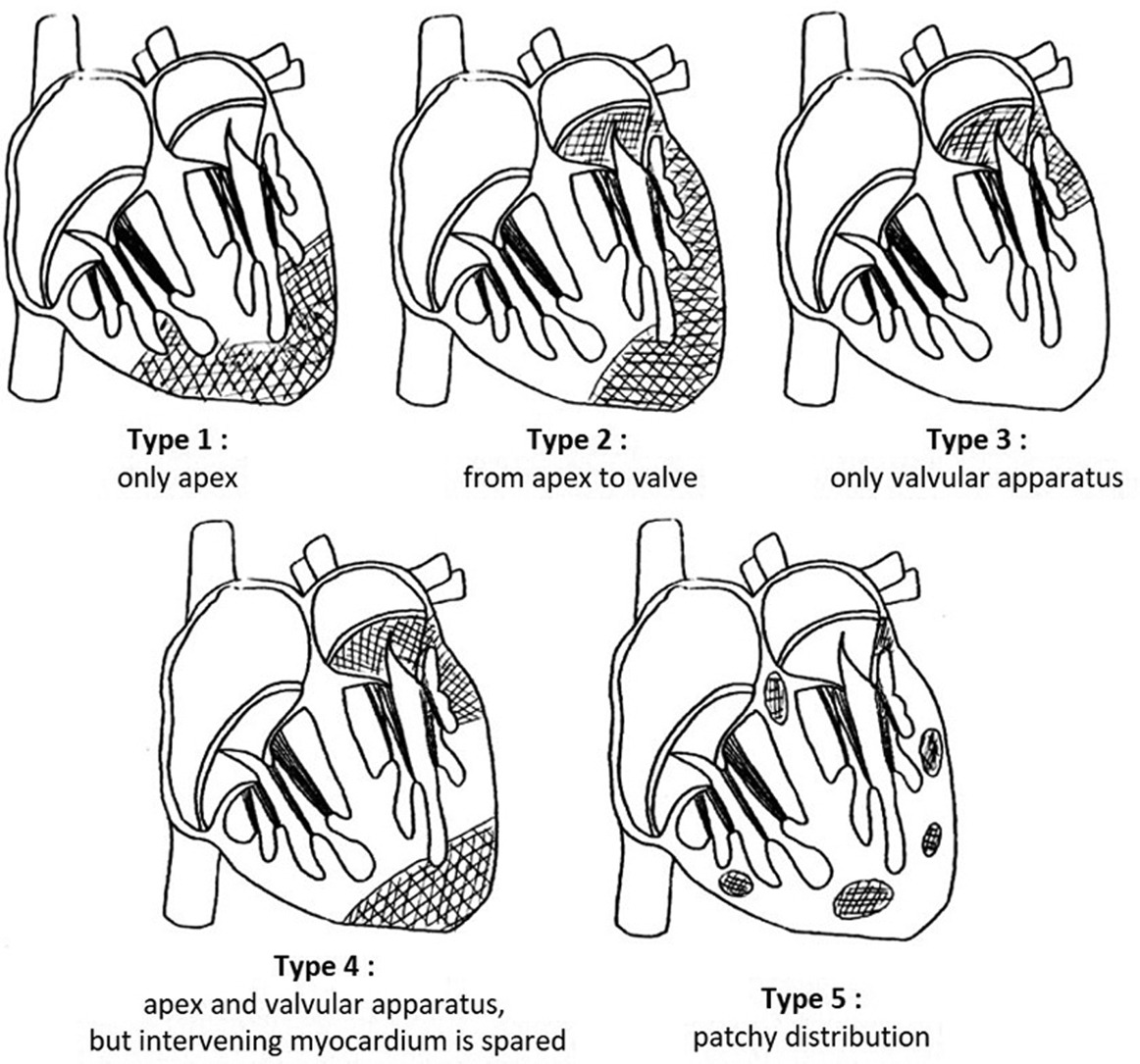
- Hallmark is apical obliteration of LV and or RV
- Clues: normal apical wall motion (vs isolated LV thrombus), hypereosinohilia, and valve involvement
- Can mimic isolated LV thrombus and apical HCM
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7520398/
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731720305940?via%3Dihub
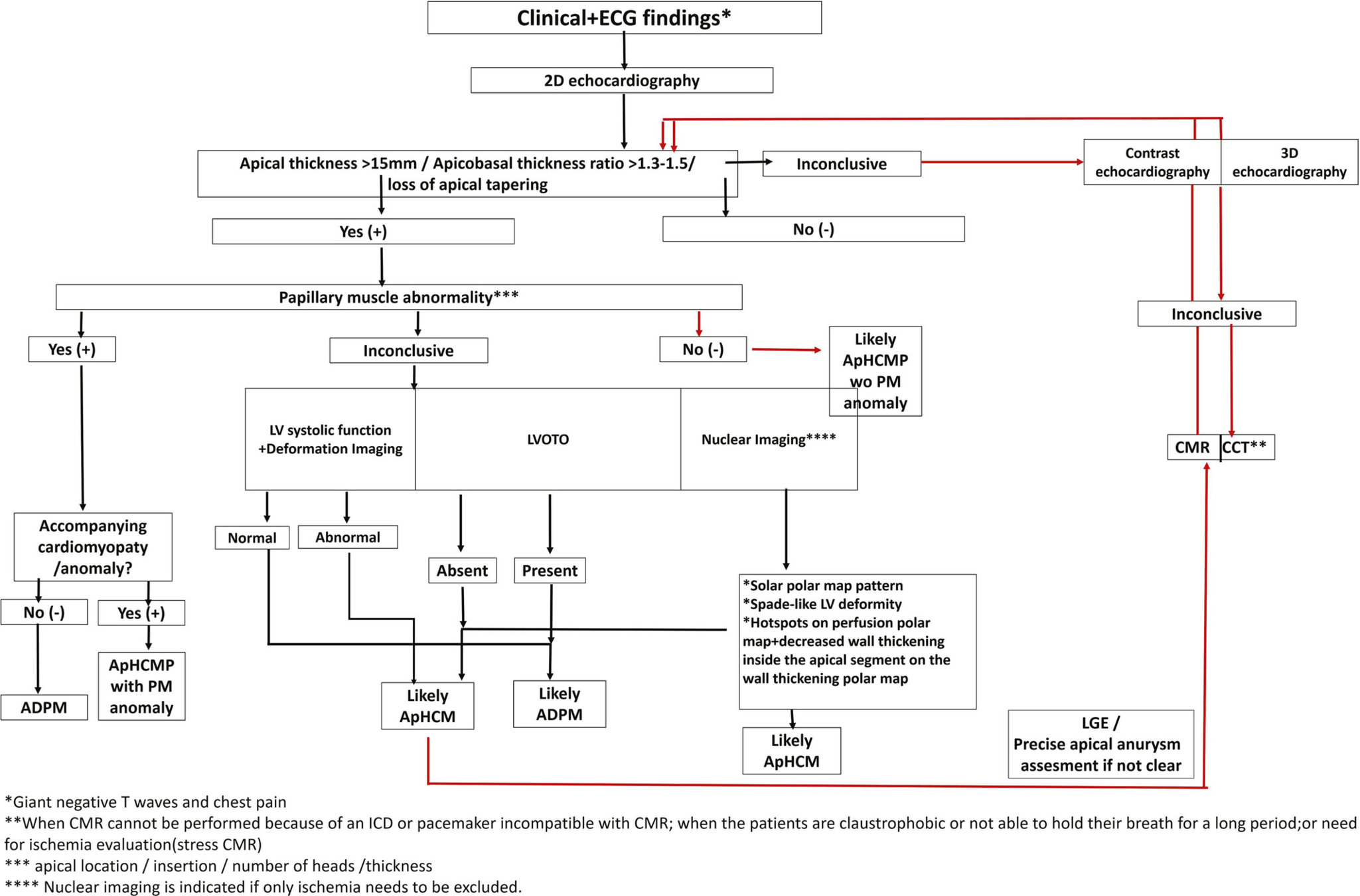
Apical HCM
- "Spade-like" LV cavity on diastole
- Can have apical wall motion abnormalities (hypokinesis and aneurysm formation)
- Early dx can be missed (giant negative t waves are a clue)
- Strain may demonstrate apical dyskinesia
- Mid-cavity obliteration and gradient may be present
Mimic
Apically Displaced Papillary Muscle
Text
https://onlinelibrary.wiley.com/doi/epdf/10.1111/echo.14895
https://onlinelibrary-wiley-com.proxy1.lib.uwo.ca/doi/full/10.1111/echo.12900
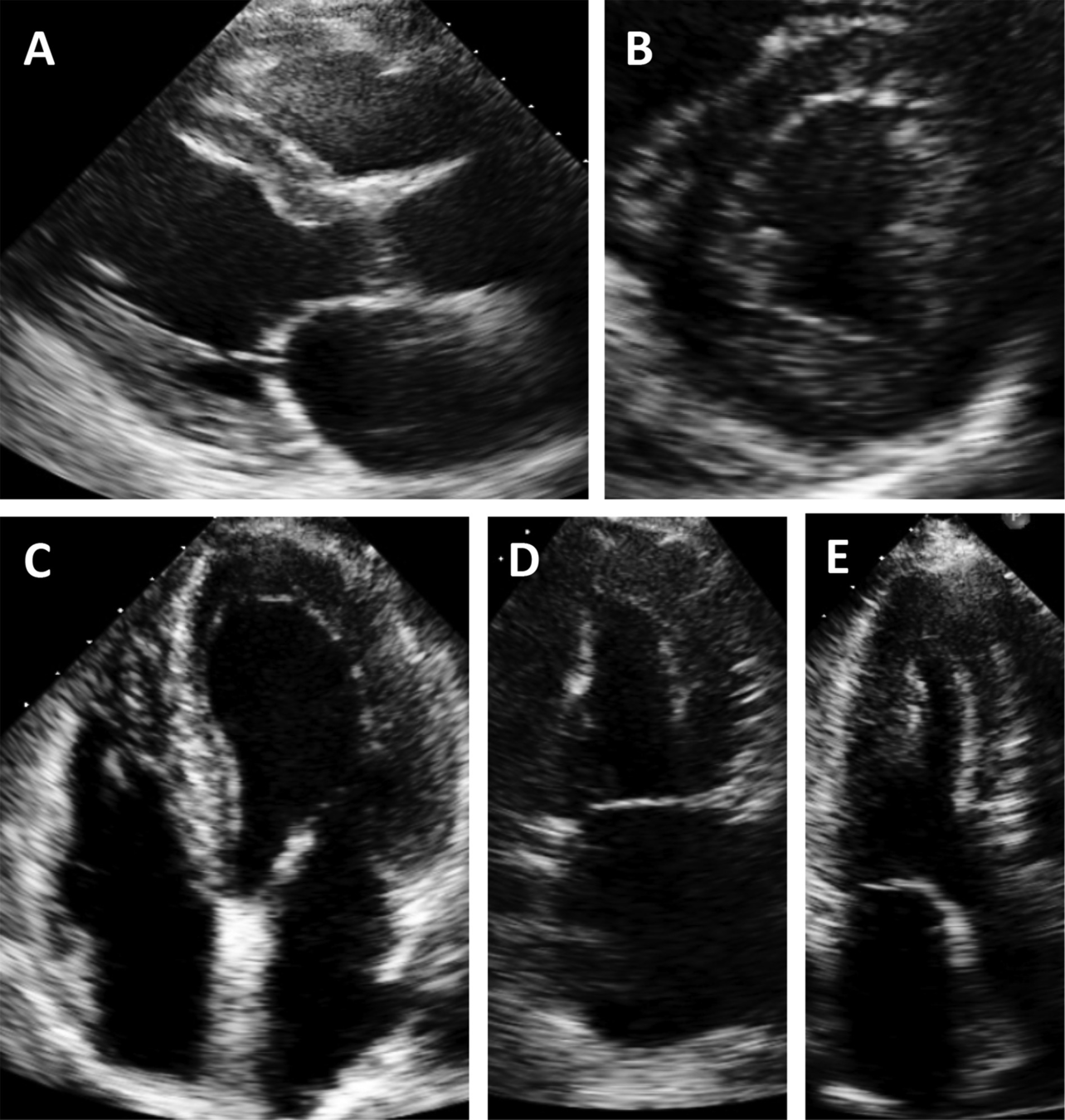
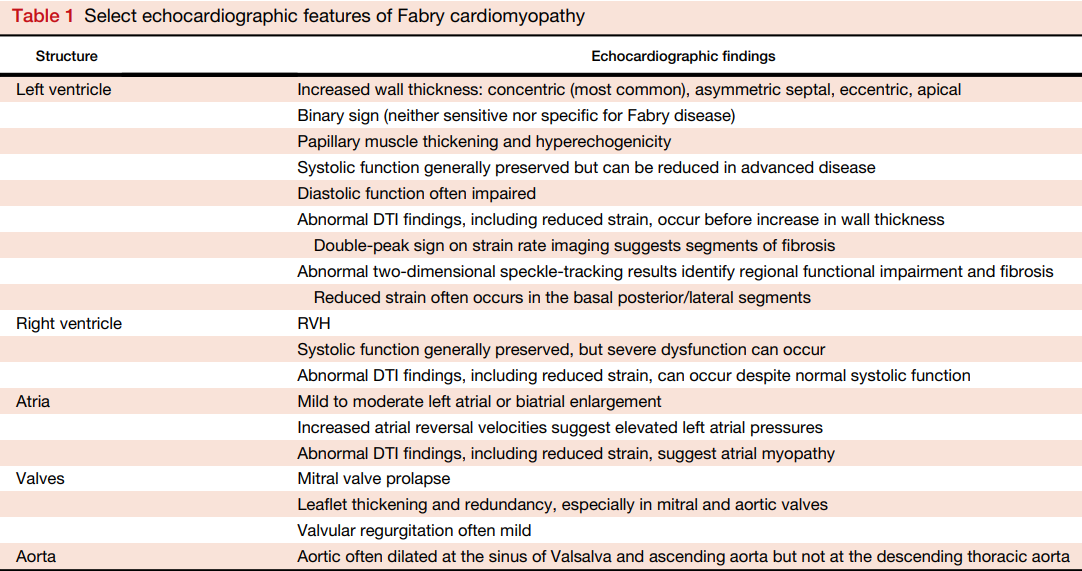
Fabrys
- Concentric thickness is most common phenotype
- Asymmetric septal hypertrophy, eccentric hypertrophy, and apical hypertrophy also possible
- HCM cohorts, up to 12% diagnosed as Fabrys
- Should be on differential for HCM or unexplained hypertrophy
- Abnormalities in the atria, valves, aorta, and papillary muscles can also be seen
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731718300415?via%3Dihub#bib20
Fabrys
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731718300415?via%3Dihub#bib20
- Binary Sign: "hyperechogenic endocardial surface adjacent to a relatively hypoechogenic subendocardial layer"
Non-Compaction
- Multiple criteria exist
- Jenni:
- Thick non-compacted and thin compacted layer (>2:1)
- Flow in the intertrabeculated recess
- Prominent trabecular mesh
https://www-internationaljournalofcardiology-com.proxy1.lib.uwo.ca/article/S0167-5273(14)02384-5/fulltext
https://www-internationaljournalofcardiology-com.proxy1.lib.uwo.ca/article/S0167-5273(14)02384-5/fulltext
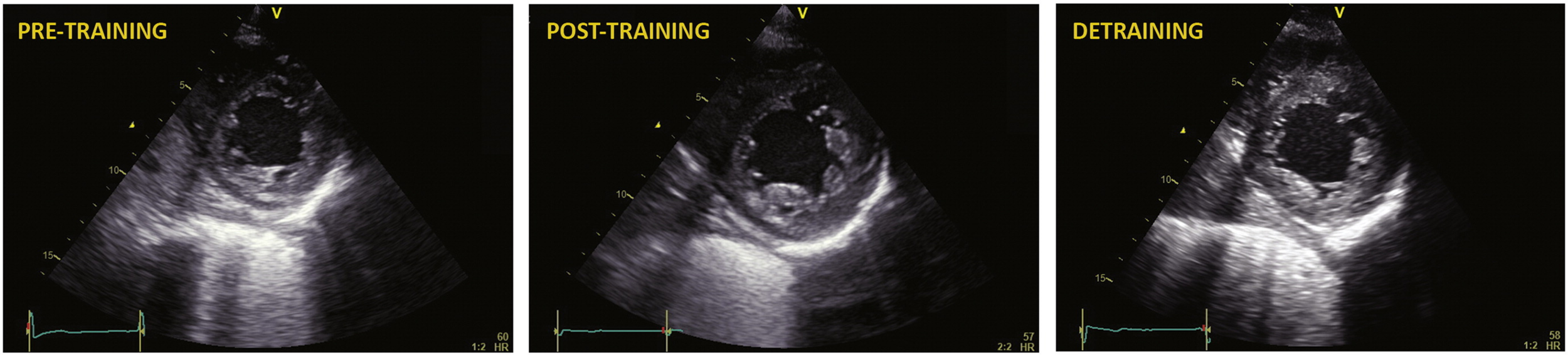
Mimic - Hypertrabeculation
- One study showed 18% of athletes have an increased LV trabeculation and 8% fulfilling the conventional criteria for LVNC
- Especially in African/Afro-Carribean athletes
- Longitudinal study needed
Back to the Case
LV Thrombus post Anterior MI