Case
Case
- 79M with mechanical aortic valve replacement (1972 and re-do 1987) and ascending aorta/arch replacement for aneurysm in 2012
- PMH:
- Atrial fibrillation
- DM type II
- Dyslipidemia
- Prostate Cancer
- CVA
- Presented to hospital with fevers and chills
- Found to have blood cultures positive for strep infantarius (strep bovis group)
Echo
TTE
TTE
Baseline Periop TEE
TEE
TEE
TEE
Echo
- Status post mechanical aortic valve replacement (1972 and re-do 1987) and non-coronary sinus resection,ascending aorta/arch replacement 2012. Posterior aortic root appears thickened with mobile wall and echolucency. There appears to be flow into this space - likely represents root abscess. Appearance quite different from post-op TEE 2012. Unable to determine if this change is chronic but given positive blood cultures concern re:abscess.
- Bjork-Shiley valve appears well seated and functioning normally. No prosthetic valve or paravalvular regurgitation. There are small, mobile echoes seen on aortic valve (Image 30/frame 28) suspicious for vegetations. Also ill-defined mobile echo seen in LVOT (image 82) which is difficult to define given micro-cavitations but mat also represent vegetation.
Microbubbles
https://onlinelibrary-wiley-com.myaccess.library.utoronto.ca/doi/full/10.1111/echo.15945
Microbubbles
- Can be misinterpreted as endocarditis
- Different physics phenomena proposed
- degassing, cavitation, and vortex
- Last for milliseconds but if high HR can last longer
- Can coalesce into gaseous mass resembling vegetation or thrombus
- Mech AV - microbubbles seen in diastole when valve closes
- If microbubbles suspected, review in slow motion (bubbles dissipate) and/or turn off harmonics
https://onlinelibrary-wiley-com.myaccess.library.utoronto.ca/doi/full/10.1111/echo.15945
PET
PET
PET
PET
FDG Imaging:
- FDG is used to visualize metabolism. Within the myocardium there is no significant FDG uptake. However in the aortic annulus there is significant uptake of FDG. It is patchy throughout the annulus being most prominent in the posterior aspect. SUV max is 11.4. A similar picture is noted on the nonattenuation corrected images.
Conclusion:
- There is evidence highly suggestive of active acute inflammation of the annulus of a prosthetic valve.
- Given the clinical condition, this is likely prosthetic endocarditis.
PET Repeat
3 months later
PET Repeat
FDG Imaging:
- FDG was used to assess inflammation. There are multiple areas of FDG uptake. The regions are similar to previous. They are in the aortic annulus. The prominence in the posterior part of the aortic annulus has resolved. However, there are still areas in the lateral segment and in the proximal ascending aorta as well as in the more distal portion of the ascending aorta. The total FDG burden is significantly reduced. Maximum SUVs on the previous study was 11.4. Maximum SUVs on this study are in the range of 4.5-5.
Conclusion:
- The study suggests ongoing inflammation in a similar pattern, but reduced compared to previous.
Case Resolution
- Patient seen by Cardiac Surgery, ID and Cardio in followup
- ID concerned about ongoing inflammation, recommended suppressive ABX after 6 weeks of therapy
- Cardiac Surgery/Cardio discussed and patient deemed very high risk for re-operation thus medical therapy
- Today ( almost 4 years later), patient maintains on ABX and is doing well (serial repeat TTE unchanged from previous)
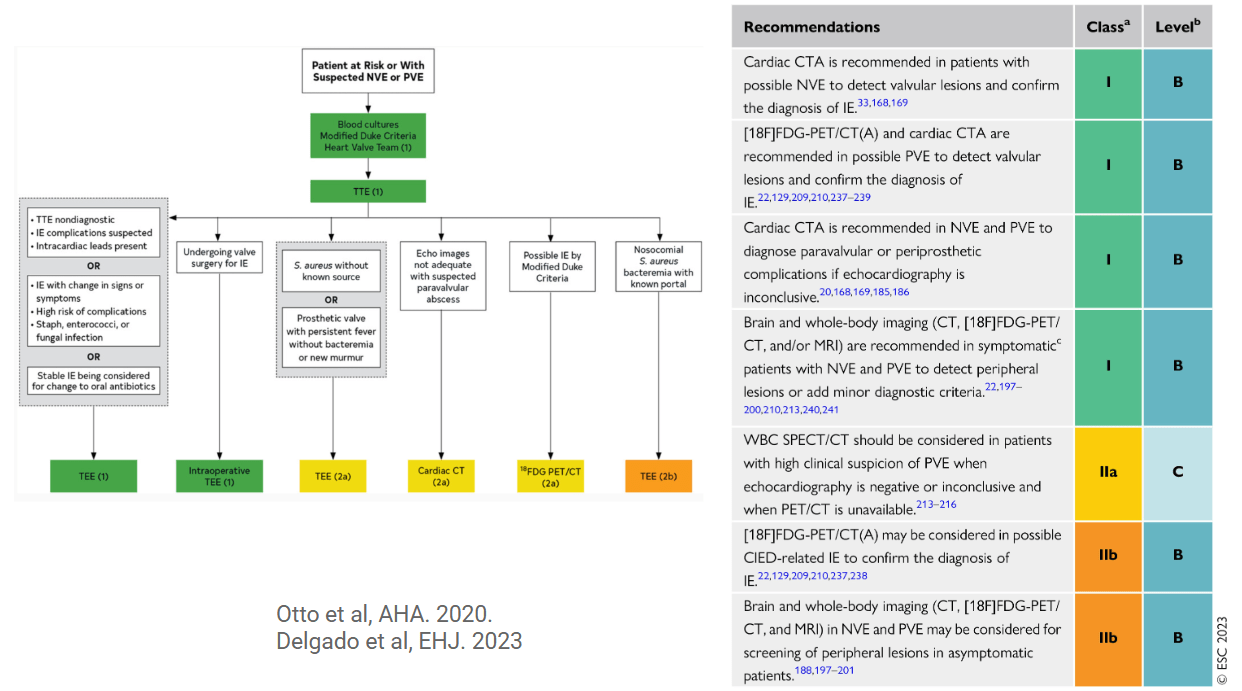
PET and IE