Prognostic value of stress echocardiography assessed by the ABCDE protocol
Journal Club Nov 4, 2021 | Atul Jaidka
Background
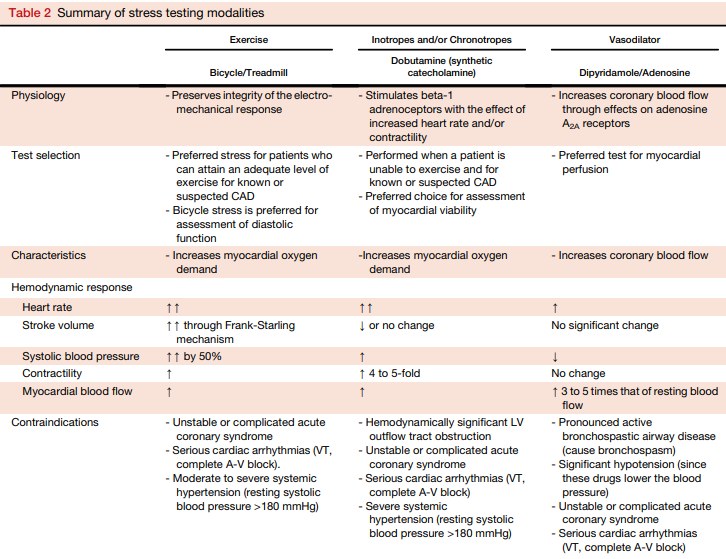
Traditional Stress Echo
-
Identification of regional wall motion abnormalities to identify coronary artery disease
- Qualitatively assessed
- Other prognostic parameters:
- Exercise duration, BP response, ST-T changes and LV dilation (not reliably reported)
Compared to Alternatives
-
Advantages
- Inexpensive
- No radiation
- Portable
- Exercise and non-exercise
-
Disadvantages
- Functional testing thus may not pick up non-obstructive clinical atherosclerosis that can cause events
- Compared to Coronary CT
- WMA are later in the ischemic cascade (not capturing perfusion changes)
- Compared to MIBI
- Functional testing thus may not pick up non-obstructive clinical atherosclerosis that can cause events
Rest
Post Exercise
LAD Ischemia
Why New Protocol?
- Incidence of coronary disease on stress testing has significantly decreased over the years
- Traditional stress testing does not capture the heterogeneity of patients
- Goal of new protocol is to provide new metrics to further risk stratify patients
- Different variables to independently and incrementally assess points of vulnerability in a patient
- When functional test is "normal", can be confidently tell patients they are "low risk"
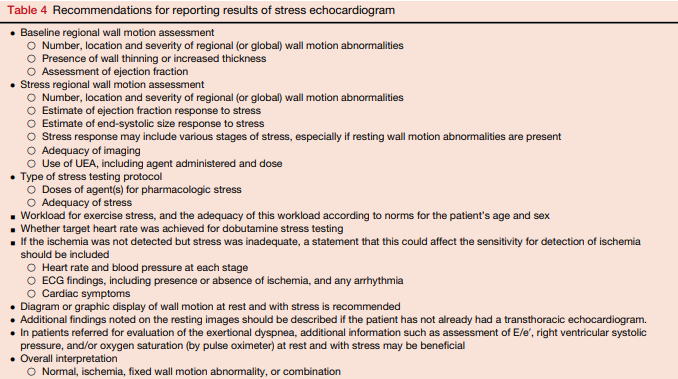
ABCDE-SE Protocol
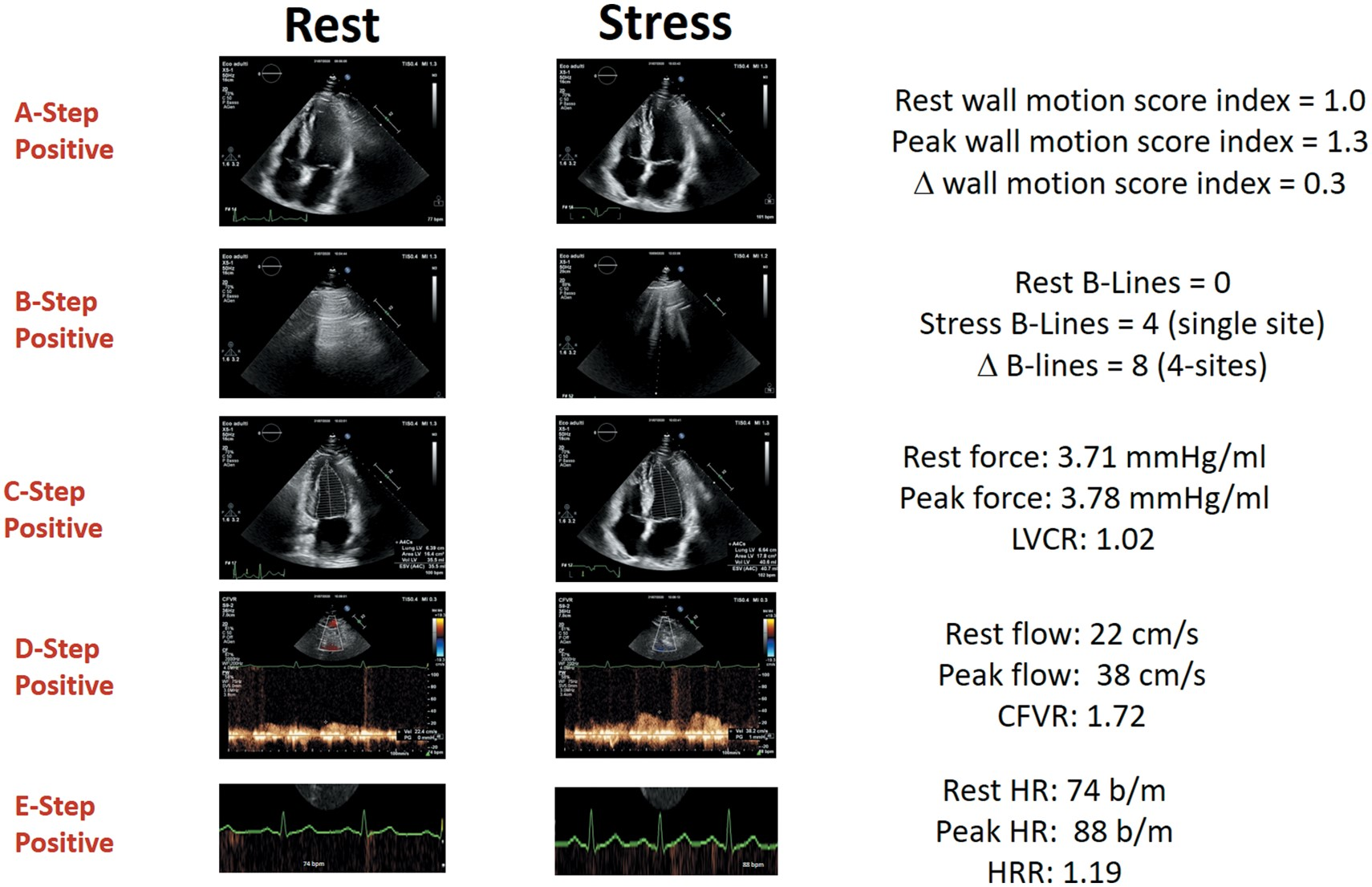
ABCDE Stress Echo
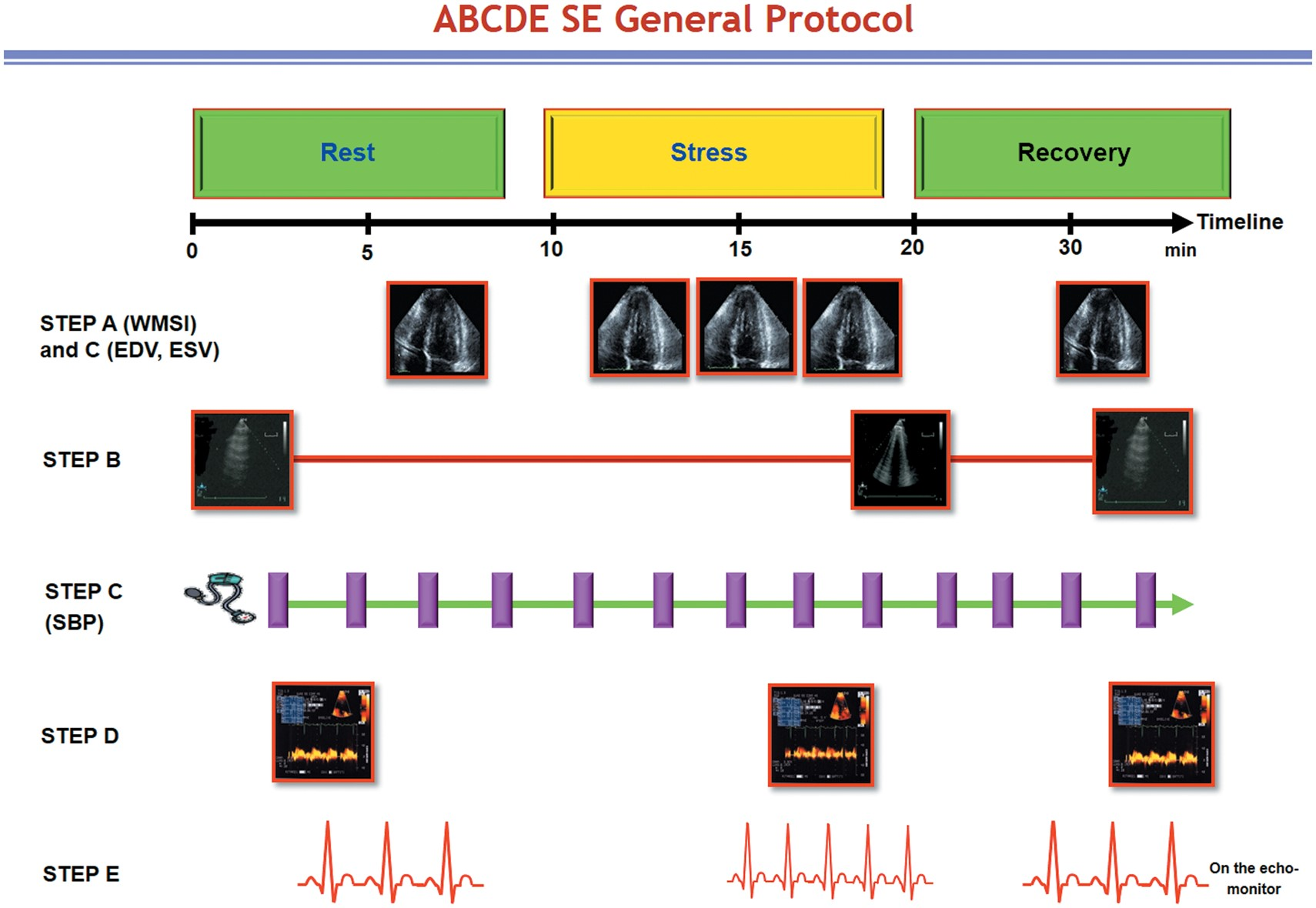
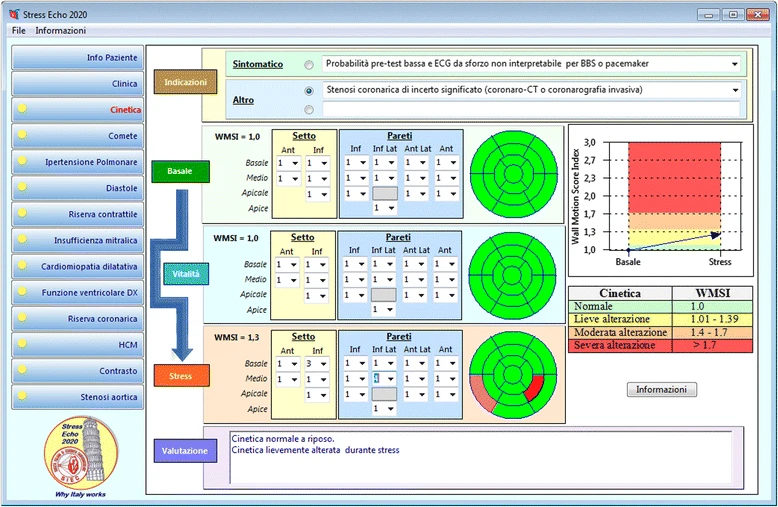
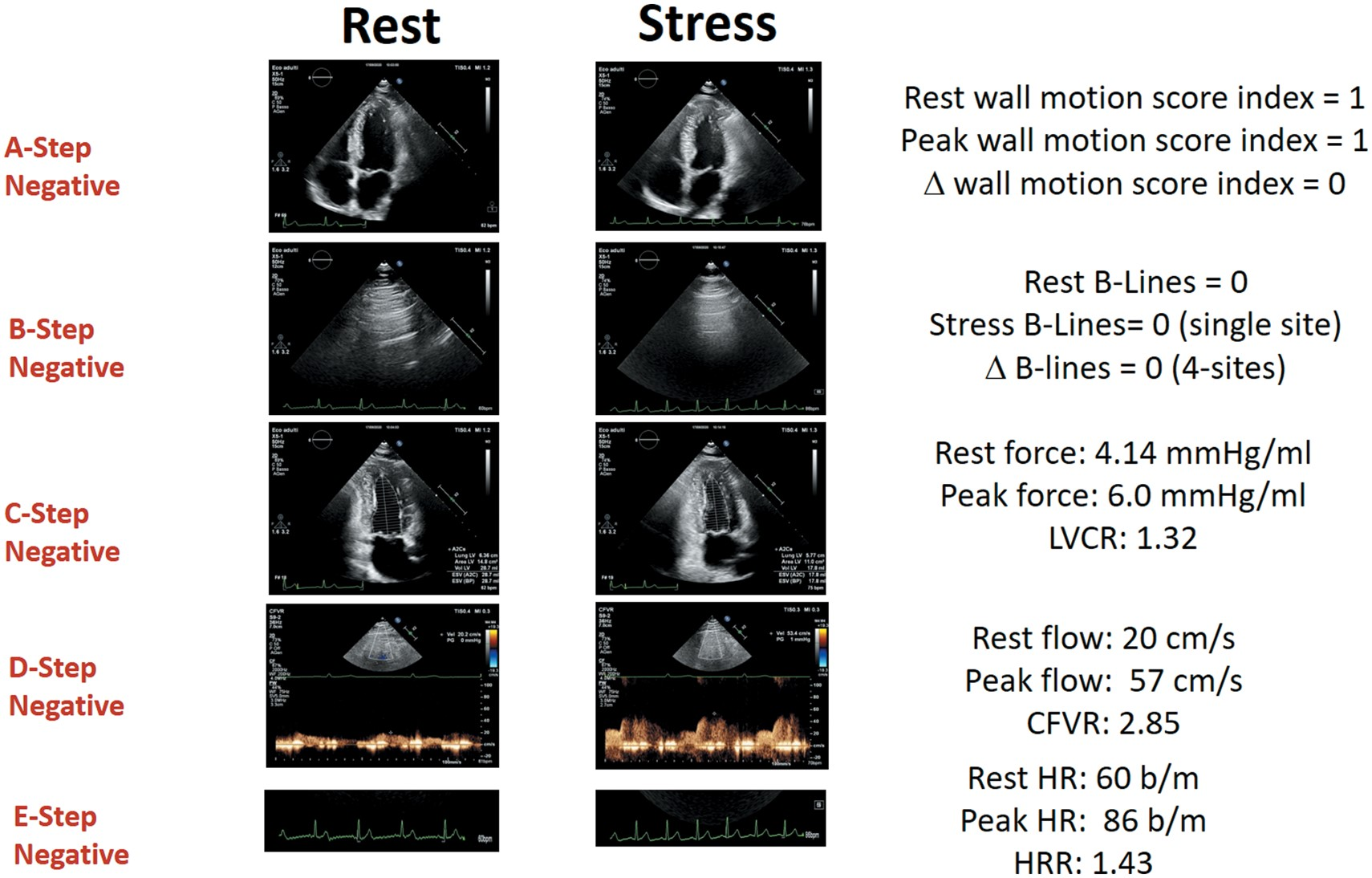
Step A: Myocardial Ischemia
- Assessment: Wall motion score index, 1 (normal) - 4 (dyskinetic) in a 17 segment LV model
- Positivity: 2 adjacent segments of same vascular territory increment by at least 1 point
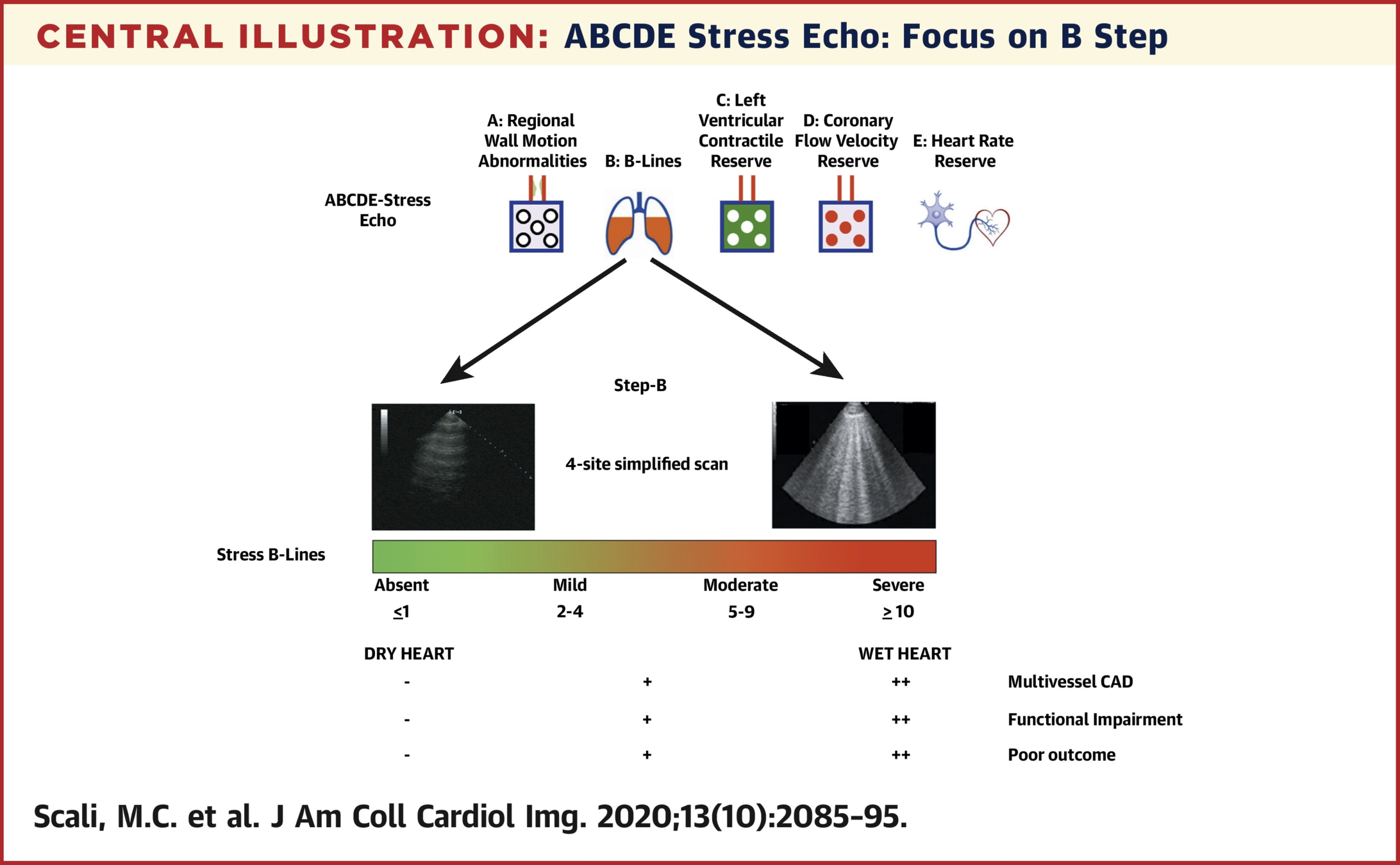
Step B: B Lines
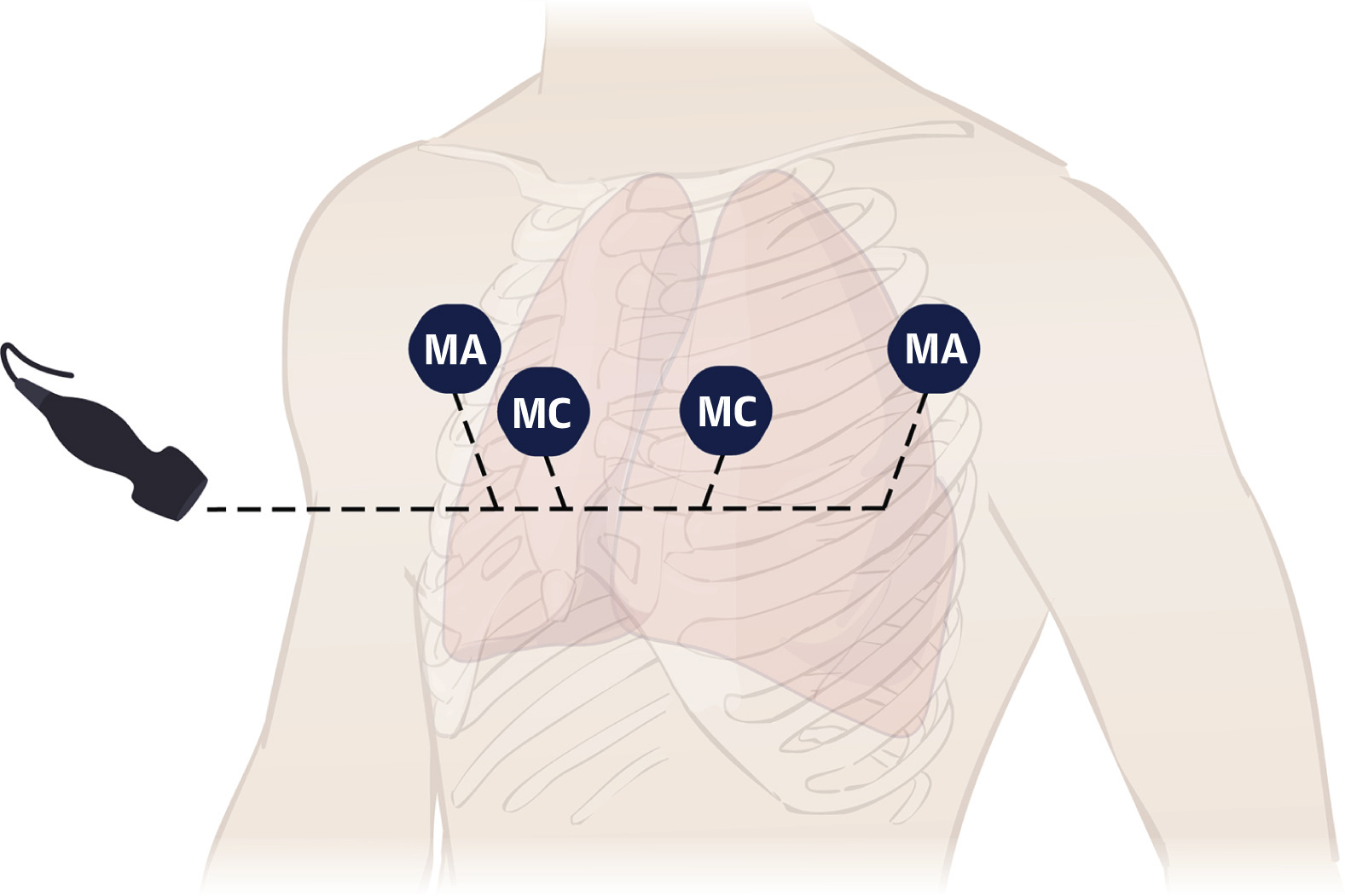
- Assessment: 4 quadrant lung ultrasound for b lines
- Positivity: 2 or more
Step B: B Lines
- Assessment: 4 quadrant lung ultrasound for b lines
- Positivity: 2 or more
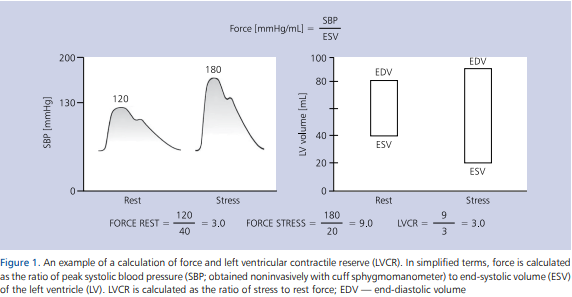
Step C: LVCR
- Assessment: Left ventricular contractile reserve is calculated as systolic blood pressure/end-systolic volume
- Positivity: LVCR < 2 for exercise/dobutamine or <1 for vasodilators
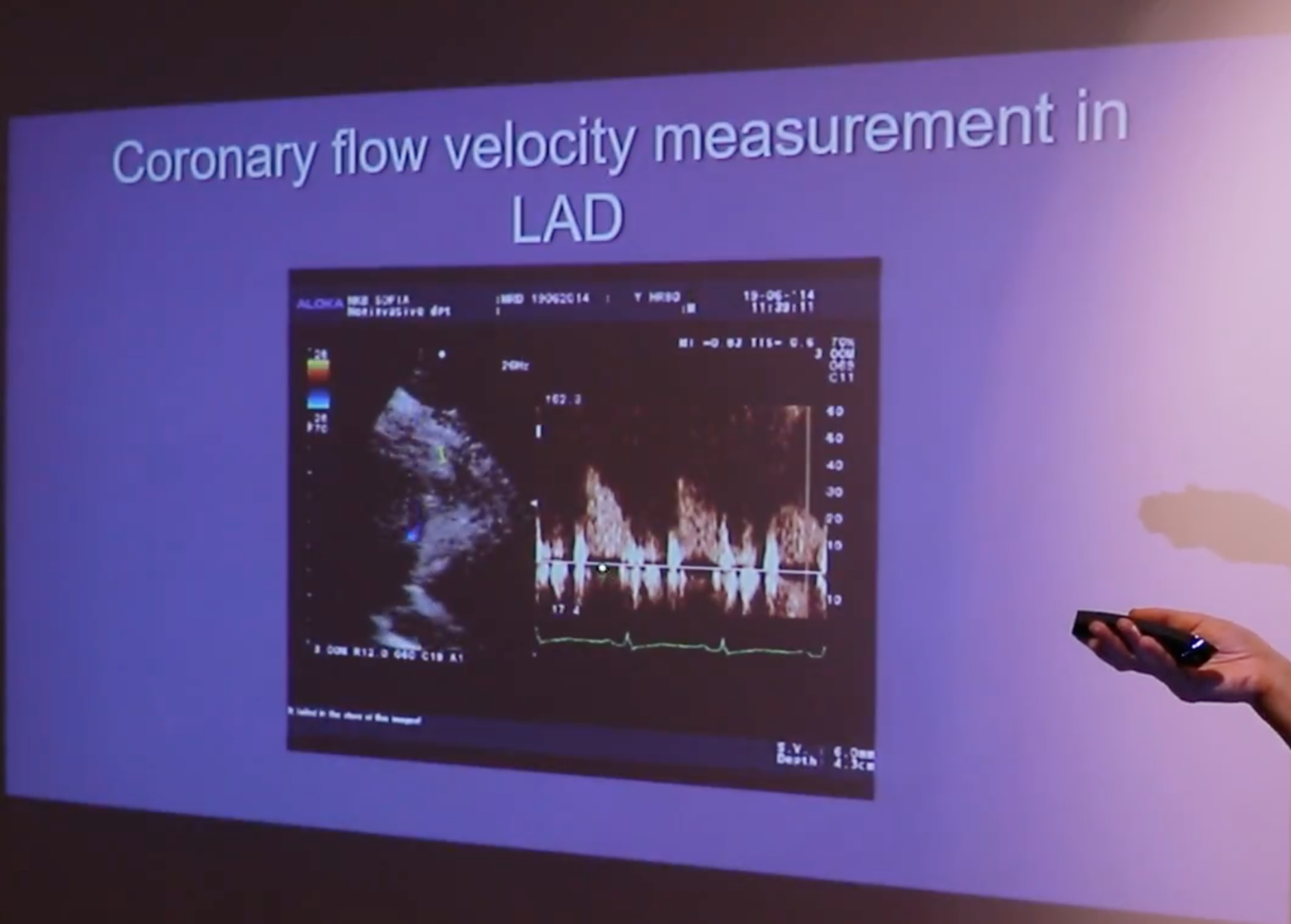
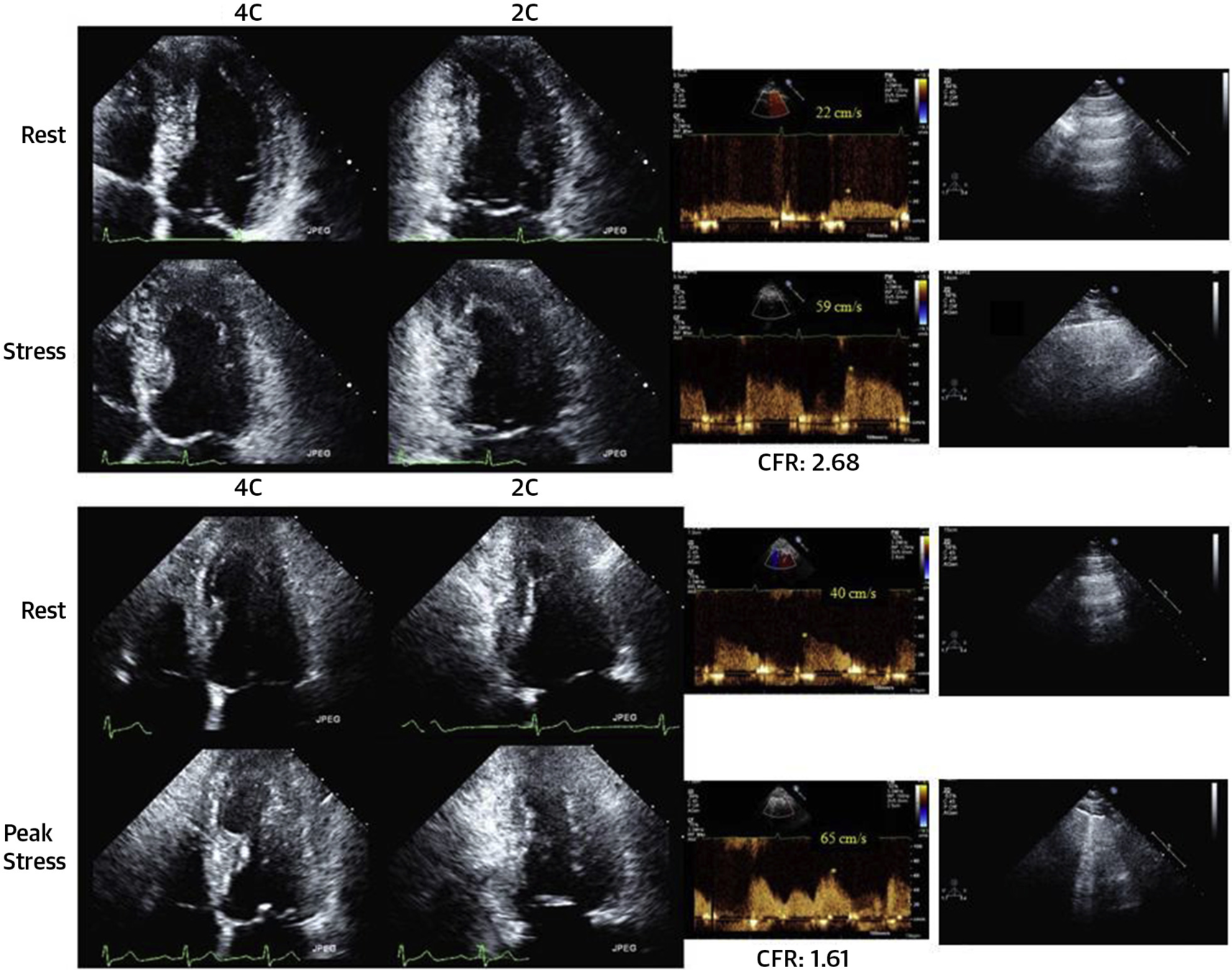
Step D: CFVR
- Assessment: Coronary flow velocity reserve of mid-distal LAD (low PLAX or modified A2/3/4)
- Positivity: CFVR < 2
- Success rate of 88% in obtaining CFVR on LAD (3000/3410). Acquisition and Interpretation in < 4 minutes
Step D: CFVR
Step D: CFVR
Step E: HRR
- Assessment: Heart rate reserve peak/rest heart rate
- Positivity: HRR <1.8 for exercise/dobutamine or <1.22 for vasodilator
- Previous studiers show blunted HRR is a predictor or adverse events in vasodilator stress echo independent of inducible ischemia and beta blocker therapy
Example: Normal
Example: Abnormal
Study
Design
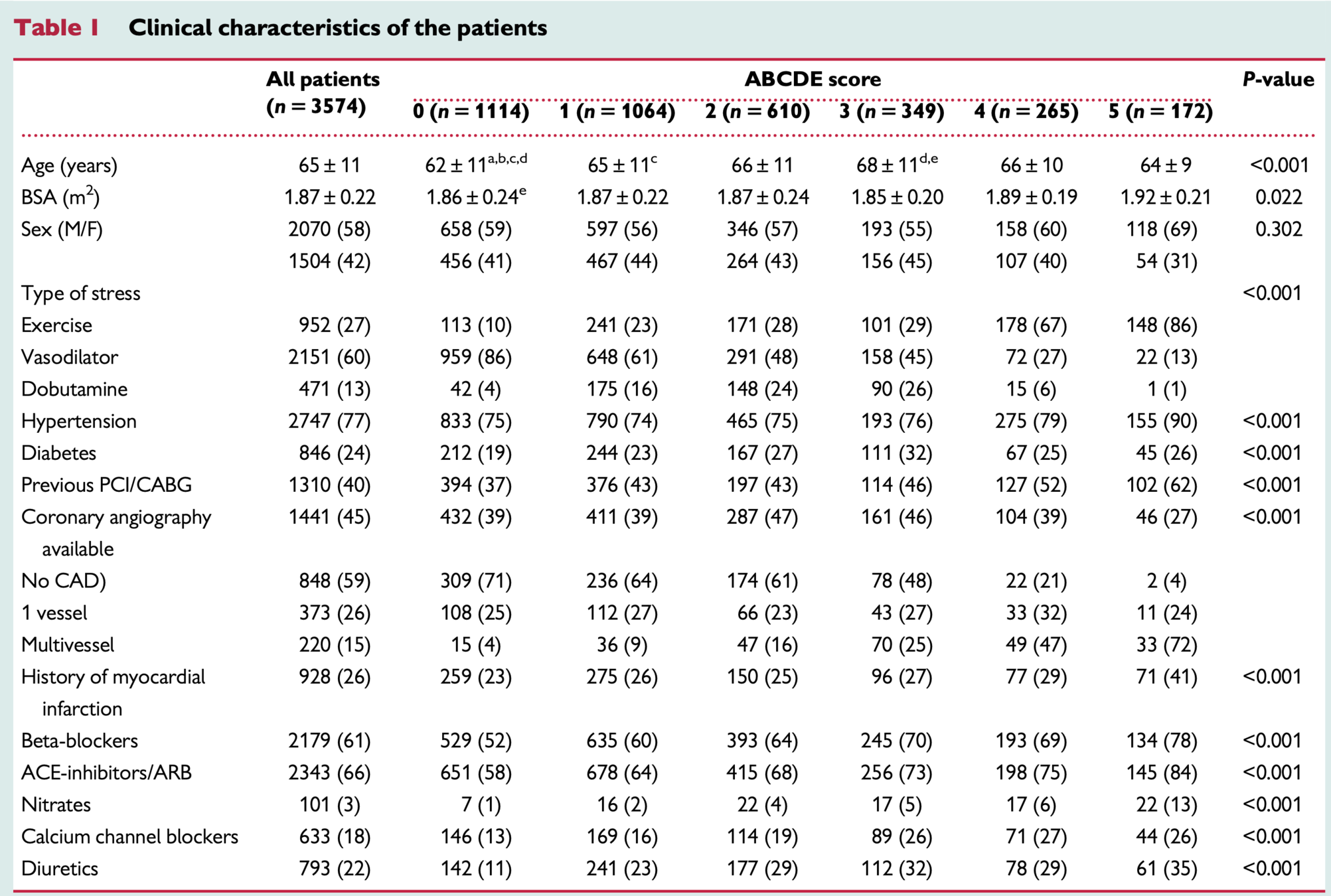
- Design: prospective, multi-centre, international, effectiveness study
- Intervention: ABCDE stress echo protocol
- Patients: known or suspected chronic coronary syndrome
- Outcomes: All cause death
Inclusion/Exclusion
- age >18 years
- referral for known or suspected CAD
- no severe primary valvular or congenital heart disease, or presence of prognosis-limiting comorbidities, such as advanced cancer, reducing life expectancy to <1 year
- echocardiography of acceptable quality at rest and during stress
Results
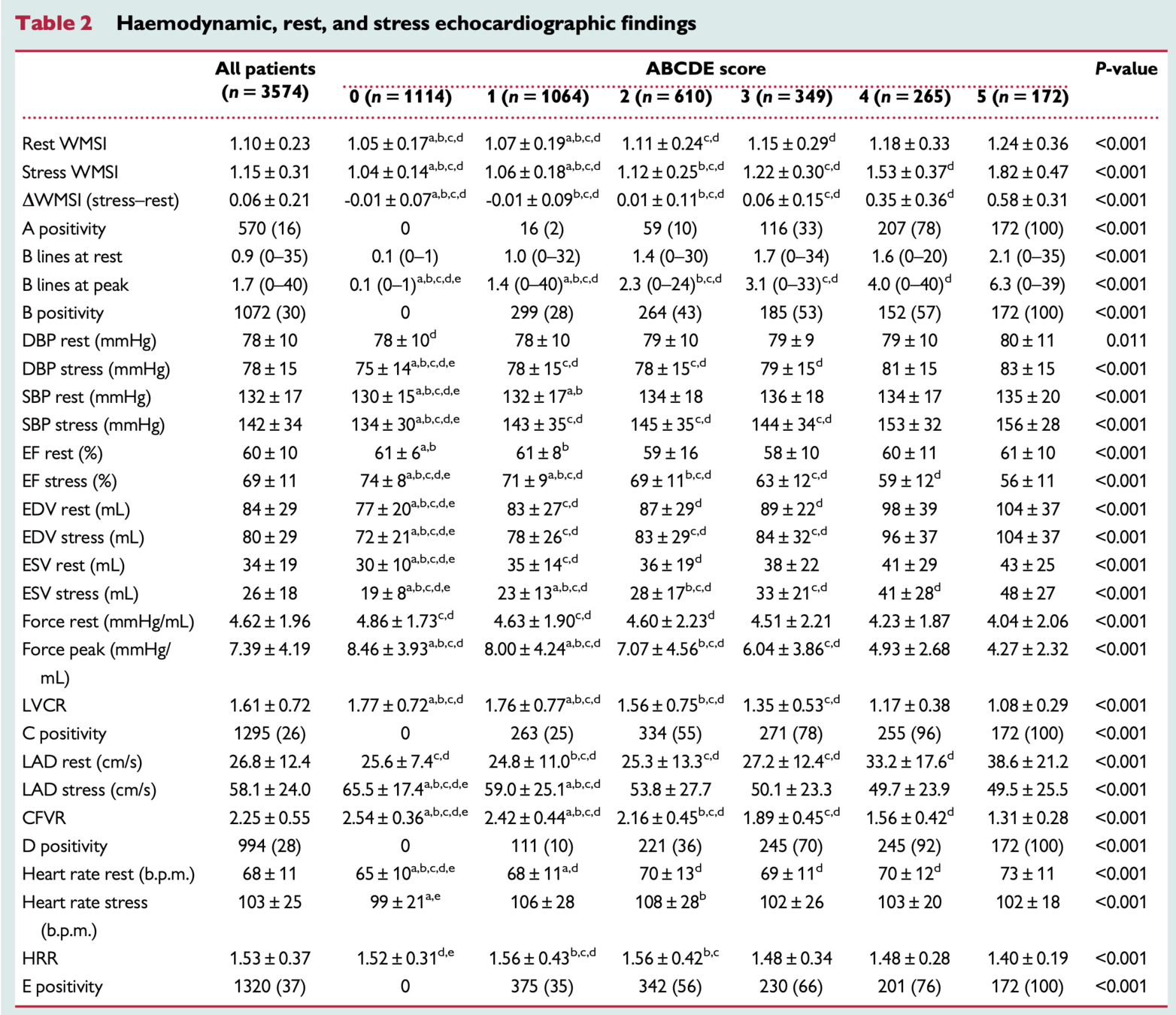
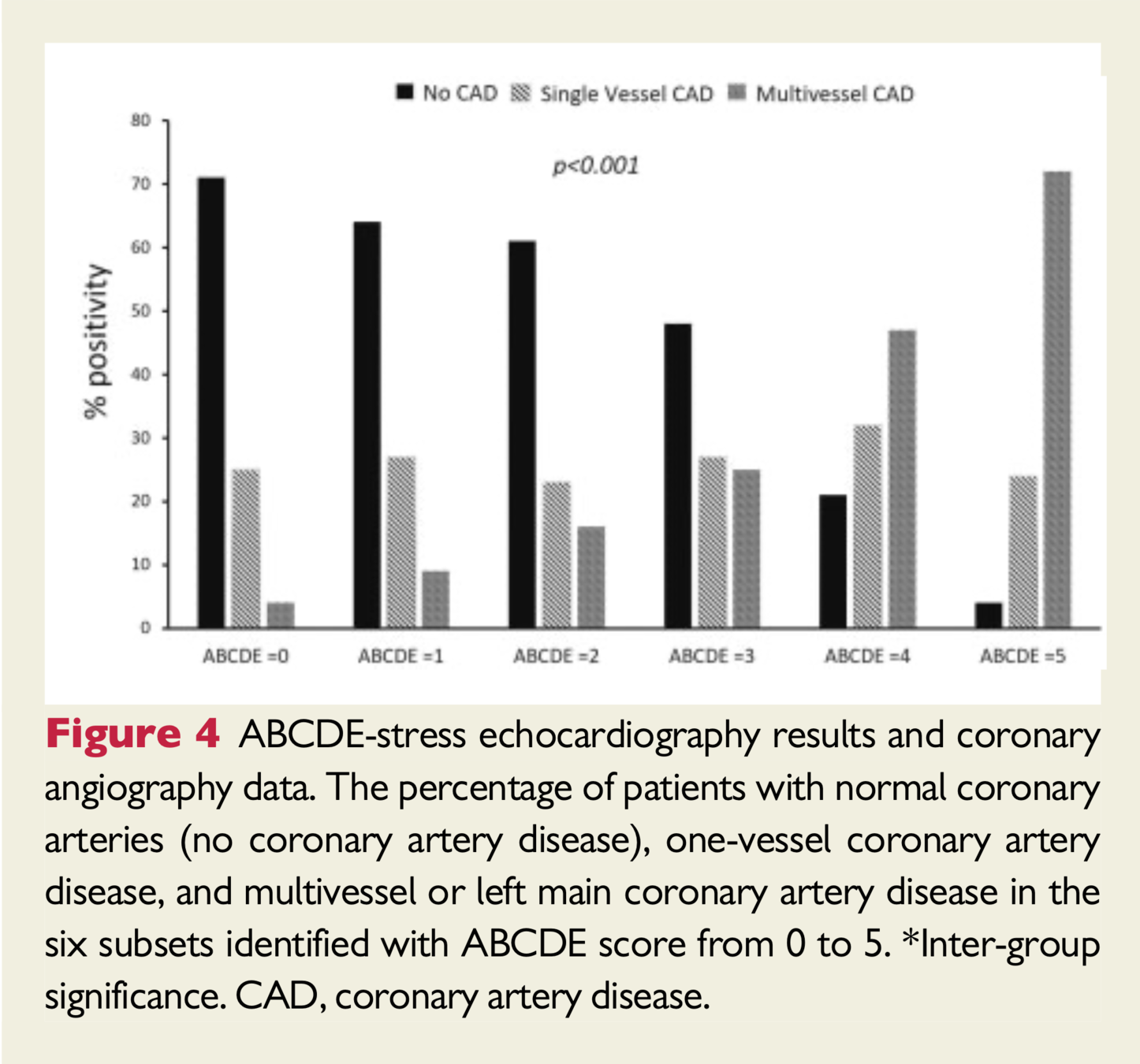
- Of those with normal SE who underwent coronary angiography, 30% demonstrated obstructive CAD, whereas in those with all five abnormal steps on SE, 95% had significant CAD.
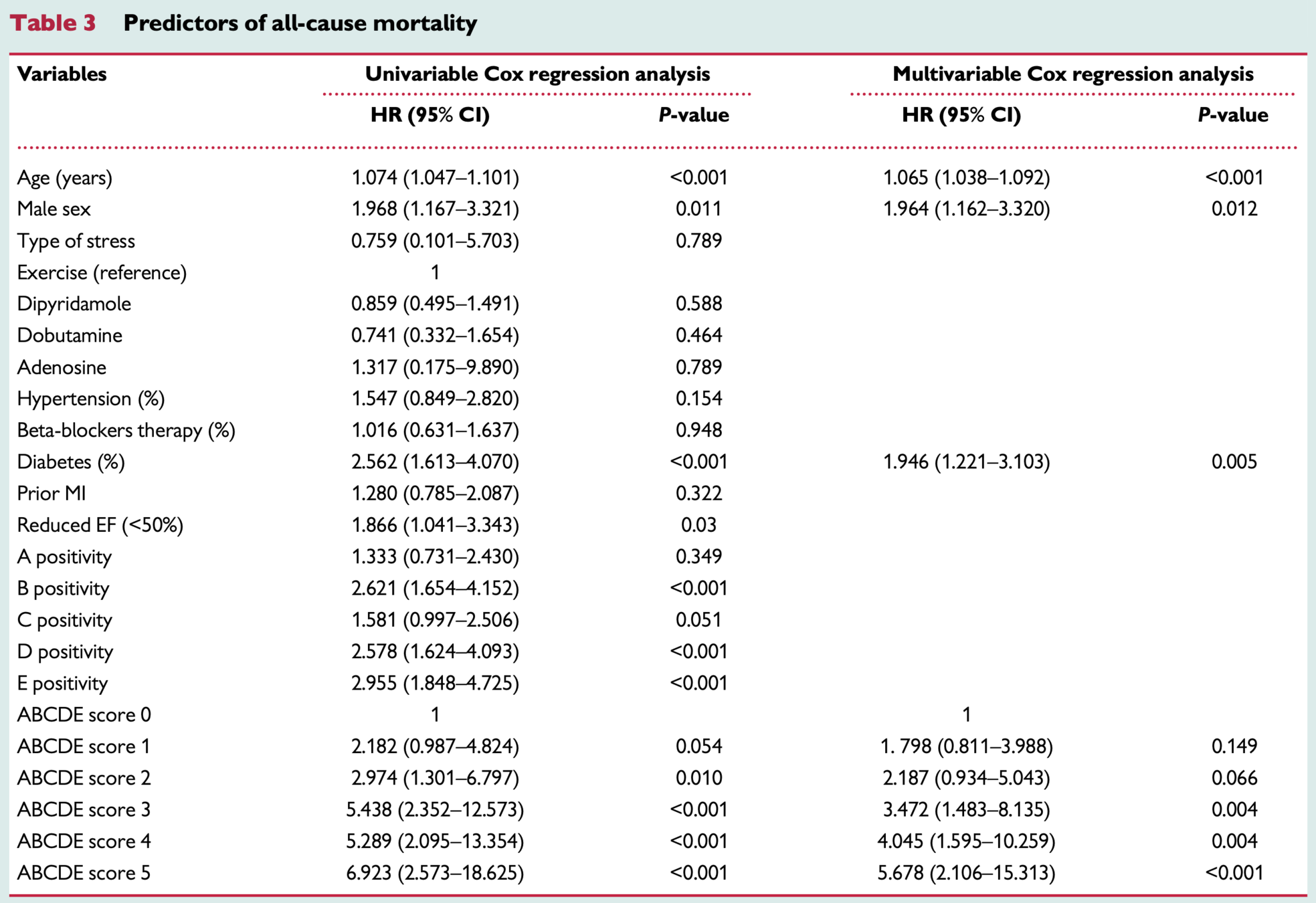
Predictors of Mortality
-
Postive:
- B-lines
- Coronary flow velocity reserve
- Heart rate reserve
- ABCDE Score 3 or greater
-
Negative:
- Regional Wall Motion Abnormalities
- Left ventricular contractile reserve
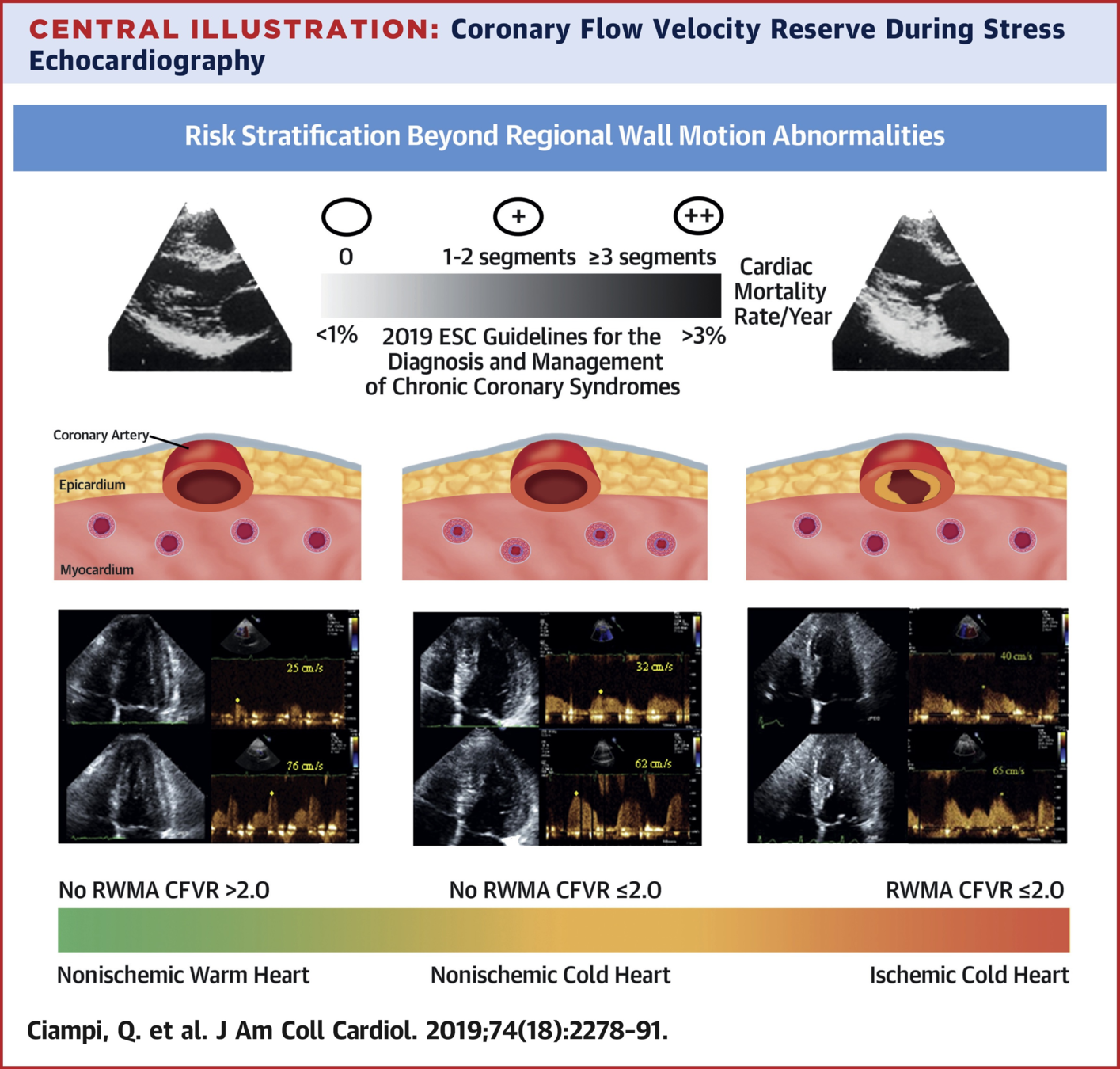
- The mortality rate was 0.4%/year for a normal SE compared with 2.7%/year when all SE steps were abnormal.
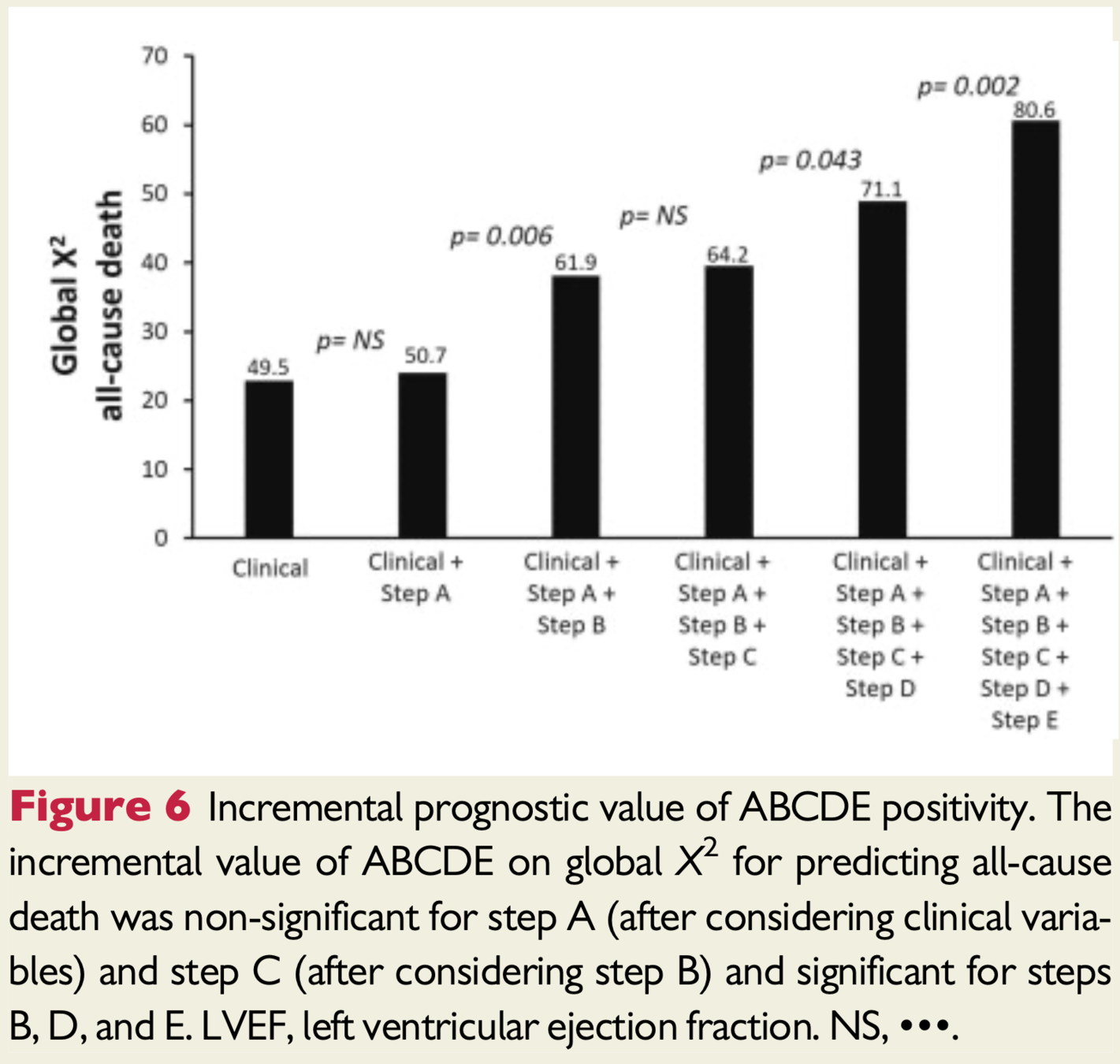
Incremental Benefit
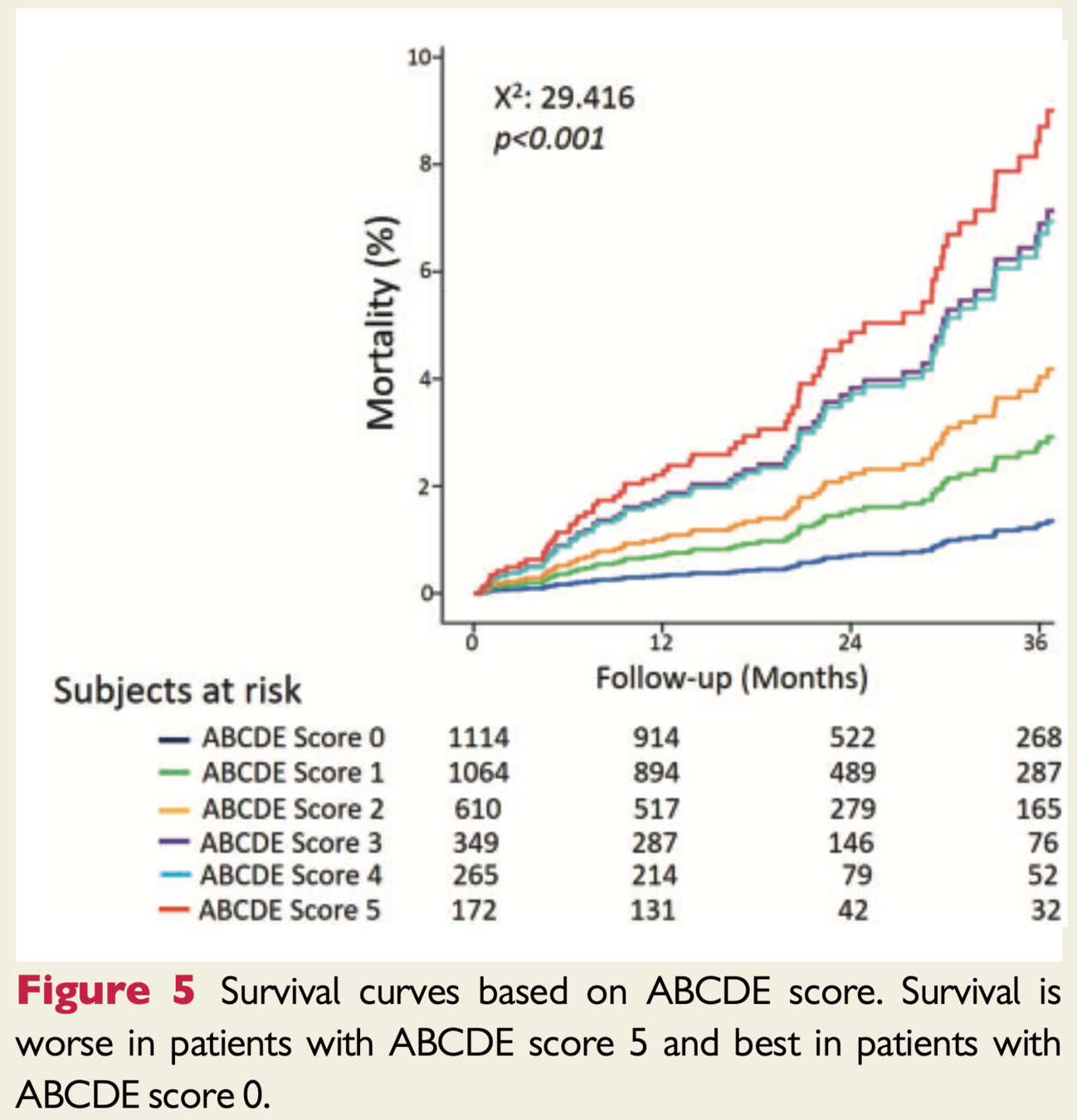
Study Conclusions
- Higher ABCDE score predicts less benign outcome
- Regional wall motion abnormalities, most used measure, less helpful in predicting prognosis
- Steps B-E are feasibly added to current stress echo protocols
- Shift assessing only coronary stenosis to patient as a whole
- Other vulnerabilities including coronary microvascular dysfunction and autonomic dysfunction
Study Conclusions
- Consider targeting treatments towards the identified abnormal steps
- Stress echo low cost/risk/environmental impact and no radiation
- ABCDE protocol can be used with any stress - exercise or pharmacological (ie. in a global pandemic pharm preferred)
Proposed Tailored Therapy
- Step A identifies inducible ischemia --> BB/CCB/nitrates or possible revasc
- Step B identifies pulmonary congestion --> diuretics
- Step C (LVCR) identifies LV dysfunction --> ACEi
- Isolated Step D identifies microvascular dx --> statin
- Step E abnormalities can be targets by neurohormonal modulation (ie. BB/ACEi/MRA/renal denervation)
Treatments potentially titratable to ABCDE risk score
Discussion
Discussion
- Dedicated training required to implement protocol
- Specifically coronary flow of LAD is most challenging
- Originally planned 5000 patients and 3 year followup but achieved ~3600 and 21 month followup
- 2020 was planned last year of study but COVID
- No other end points other than mortality to assess predictive power of protocol steps
- Ie. B-lines and HF admissions
Discussion
- Images were not reviewed by core lab
- Practical for effectiveness study as has real-world applicability
- Parameters were binary, positive or negative, future studies plan to consider mild-mod-severe stratification
- Most patients underwent dipyridamole stress, would be beneficial to compare predictive value of the steps by stress modality (could explain why physiological measures such as LVCR were not predictive)
- High score 4-5 were mostly in exercise group
Discussion
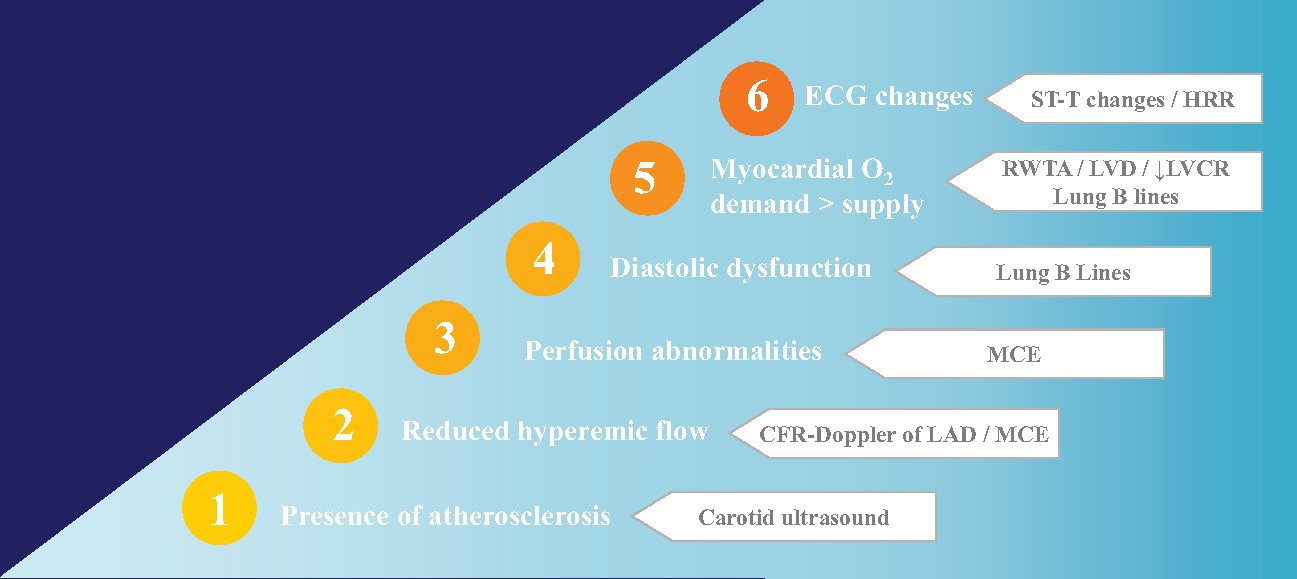
- RWMA may not be a strong enough tool to assess for ischemia as significant oxygen supply demand mismatch is needed
- Future protocols could employ myocardial contrast echocardiography to assess perfusion
- Low usage of contrast in general in the study
- Functional testing may not pick up non-obstructive lesions which can still lead to to events
- Critics recommend carotid ultrasound to pick up on clinical atherosclerosis
Future Direction
Modified ABCDE?
Stress Echo 2030

ABCDE + F (regurgitant flow) G (LVOT gradients) L (left atrial volume/function) P ( pulmonary and LV pressures) L (RV function)
Stress Echo 2030
- 1-SE in coronary artery disease (SECAD)
- 2-SE in diastolic heart failure (SEDIA)
- 3-SE in hypertrophic cardiomyopathy (SEHCA)
- 4-SE post-chest radiotherapy and chemotherapy (SERA)
- 5-Artificial intelligence SE evaluation (AI-SEE)
- 6-Environmental stress echocardiography and air pollution (ESTER)
- 7-SE in repaired Tetralogy of Fallot (SETOF)
- 8-SE in post-COVID-19 (SECOV)
- 9: Recovery by stress echo of conventionally unfit donor good hearts (RESURGE)
- 10-SE for mitral ischemic regurgitation (SEMIR)
- 11-SE in valvular heart disease (SEVA)
- 12-SE for coronary vasospasm (SESPASM)
Questions?