Anticipatory Diagnosis Pulmonary Hypertension in Fibrotic Lung Disease Through AI-leveraged Zero-Burden Longitudinal Risk Modeling Using Routine Electronic Health Records
Girish Nair , MD
Professor of Pulmonary Critical Care and Sleep Medicine
Ishanu Chattopadhyay, PhD
Assistant Professor of Biomedical Informatics & Computer Science
University of Kentucky

-
Pulmonary hypertension is a common and clinically important complication of fibrotic ILD, including IPF.
-
PH is often detected late in routine care because confirmatory workup is usually triggered only after clear functional decline or cardiopulmonary deterioration.
-
Late recognition reduces the opportunity for timely specialty referral, risk-adjusted monitoring, and proactive care planning.
-
There is a major unmet need for a scalable way to identify fibrotic ILD/IPF patients who are entering a near-term high-risk phase for PH.
-
The proposed concept is an anticipatory-diagnosis AI approach that predicts near-term PH risk before overt clinical decompensation.
-
The model would forecast PH risk over clinically actionable horizons of 1 month, 6 months, and 1 year.
-
The approach is designed to be zero-burden at deployment, with no imaging, hemodynamic data, pulmonary function tests, laboratory values, or patient-reported outcomes as input.
-
Instead, it uses routinely collected longitudinal EHR data already available in standard care.
-
Key model inputs include time-resolved patterns in diagnoses, procedures, medications, and healthcare utilization.
-
These longitudinal patterns are intended to capture evolving cardiopulmonary stress and progression of disease.
-
The overall goal is to enable earlier identification of PH risk and support earlier intervention in fibrotic ILD/IPF care.
Anticipatory Diagnosis Pulmonary Hypertension in Fibrotic Lung Disease Through AI-leveraged Zero-Burden Longitudinal Risk Modeling Using Routine Electronic Health Records
Zero-Burden Co-morbid Risk Score (ZCoR*)
Zero Burden Risk Assessment (ZeBRA)
- Universal point-of-care screening via AI-driven pattern recognition
- No new tests or blood-work
- Uses routine data (EHR) already in patient file
- No specific data demands
- Generalizable in future to other targets beyond PF, ILAs

CKD
PF
ZCoR
ICD
Enable early diagnosis
Target PF/IPF or ILDs broadly
Seamless background integration with Epic workflows
Primary care
*Onishchenko, Dmytro, Robert J. Marlowe, Che G. Ngufor, Louis J. Faust, Andrew H. Limper, Gary M. Hunninghake, Fernando J. Martinez, and Ishanu Chattopadhyay. "Screening for idiopathic pulmonary fibrosis using comorbidity signatures in electronic health records." Nature Medicine 28, no. 10 (2022): 2107-2116.
Raising Flags before patient or their doctor notice symptoms
downstream care modulation
model published, retrospectively validated*
TimestampedDiagnostic procedural codes & prescriptions
MASH
Rx
Px
Validation
CELL Reports
AI-driven Test-Free Prediction of ICU Admission, Insulin Dependence, and Exocrine Dysfunction after Acute Pancreatitis



Under Review
Technology Overview
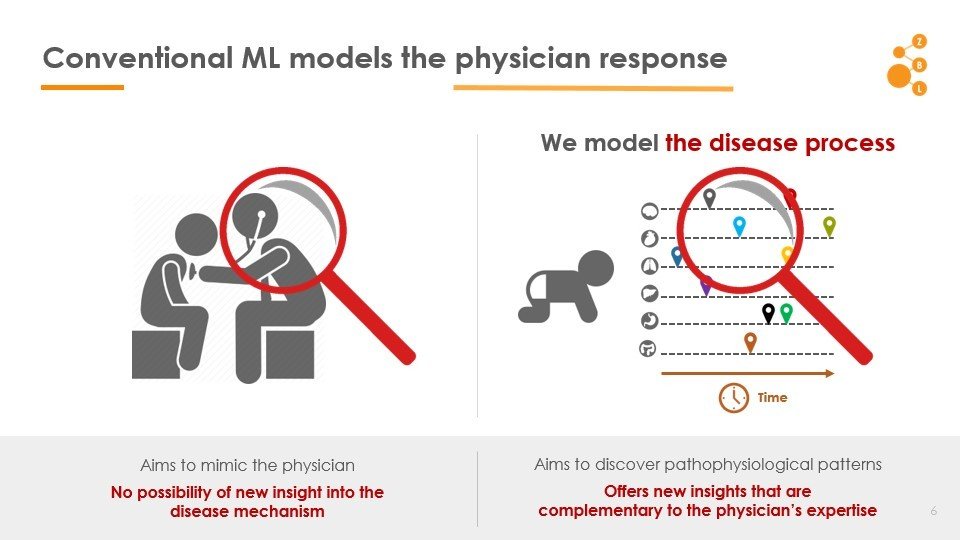
2. Conventional AI attempts to model the physician
Current State of Art
1. Use of AI in point-of-care diagnostic workflow is limited
ZeBRA
- Use under-utilized diagnostic modalities
- Discover co-morbidity patterns
- Go beyond know risk factors
- Personalized risk patterns
*Chattopadhyay, Ishanu, and Hod Lipson. "Abductive learning of quantized stochastic processes with probabilistic finite automata." Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences 371, no. 1984 (2013): 20110543.
Curated Disease-agnostic Features | Odds ratio dictionaries combined with multi-stage LGBMs | Specialized HMM based Longitudinal Tracking*
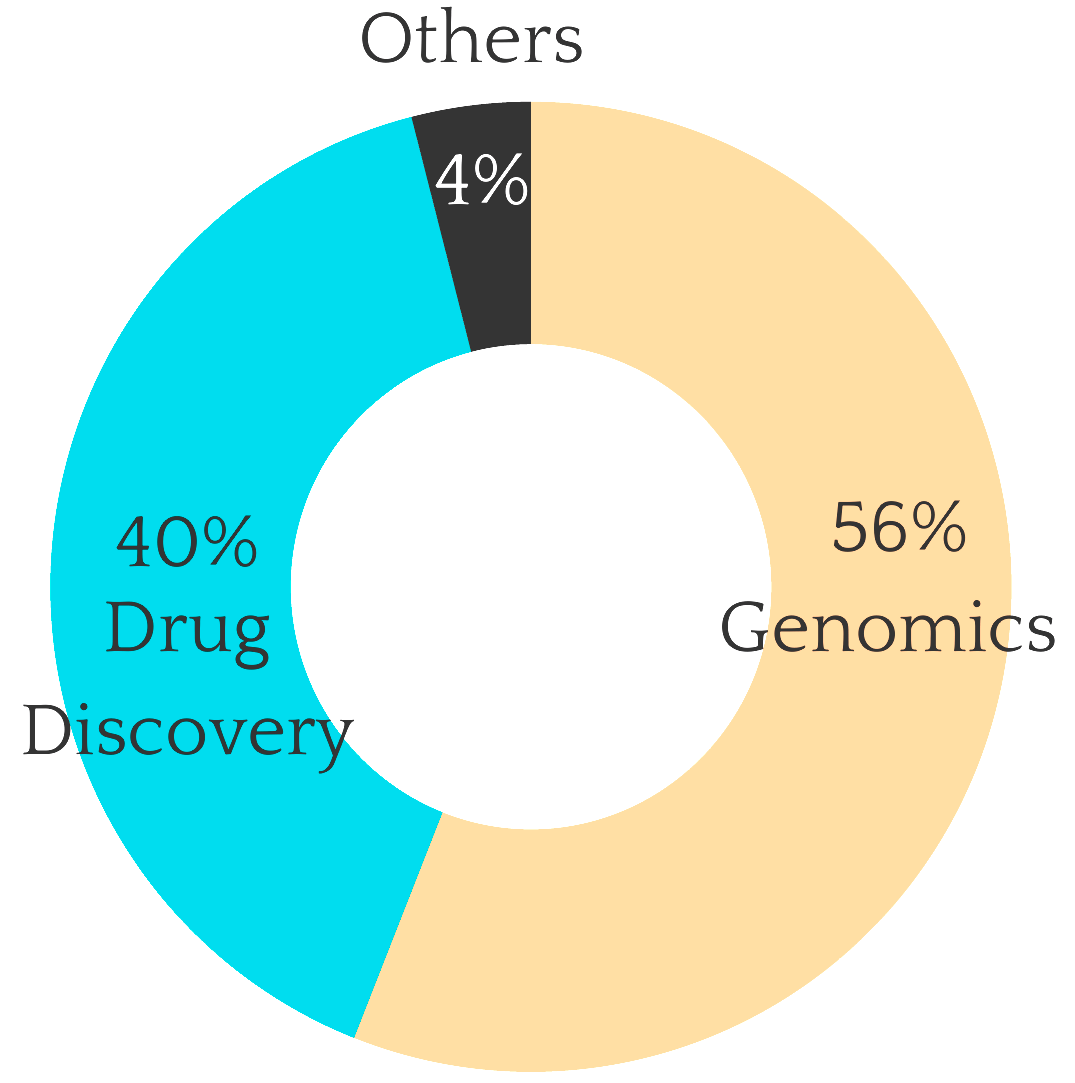
Predictive AI platforms, including those from Merative, PathAI, Tempus, Google Health, and Microsoft, often rely on imaging data for early detection.
State of the art screening approaches are inadequate
Standard AI

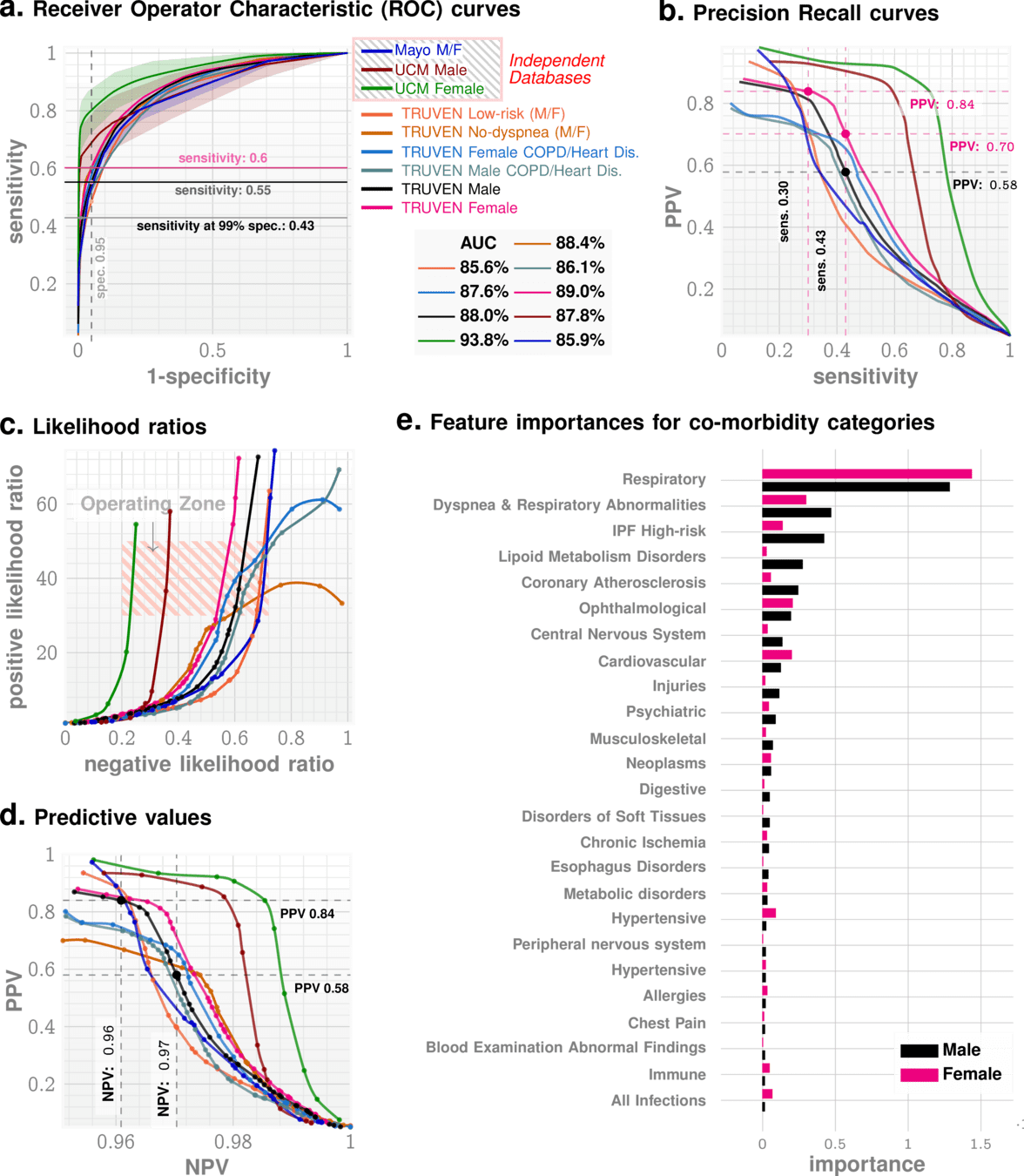
Predictive Performance*
High AUC across high and low risk sub-cohorts
Highlights:
- 1 yr out AUC ~88%
- Positive Likelihood ration ~40
*Onishchenko, D., Marlowe, R.J., Ngufor, C.G. et al. Screening for idiopathic pulmonary fibrosis using comorbidity signatures in electronic health records. Nat Med 28, 2107–2116 (2022). https://doi.org/10.1038/s41591-022-02010-y
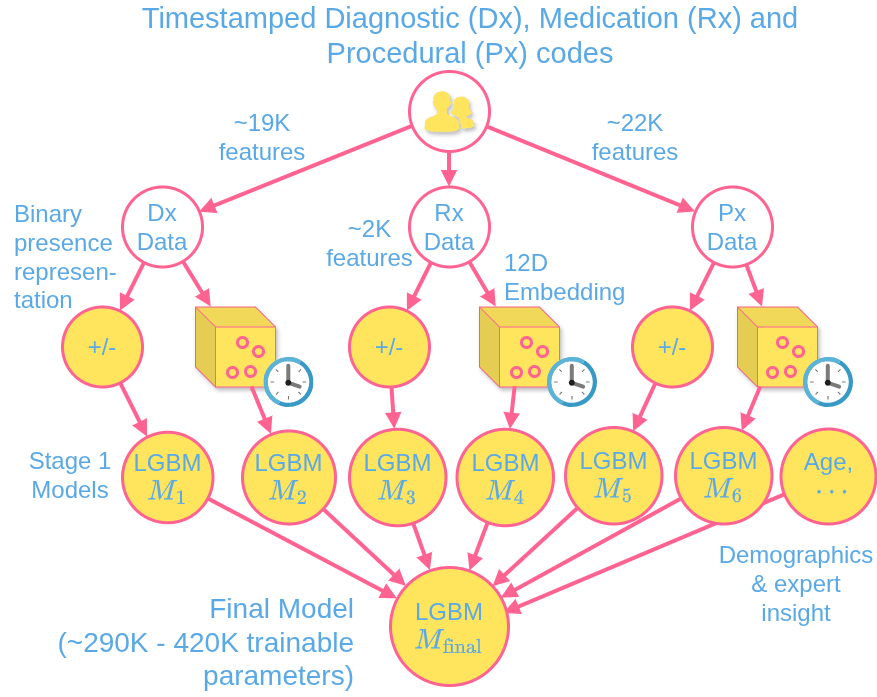
Model
ZeBRA Algorithmic Suite

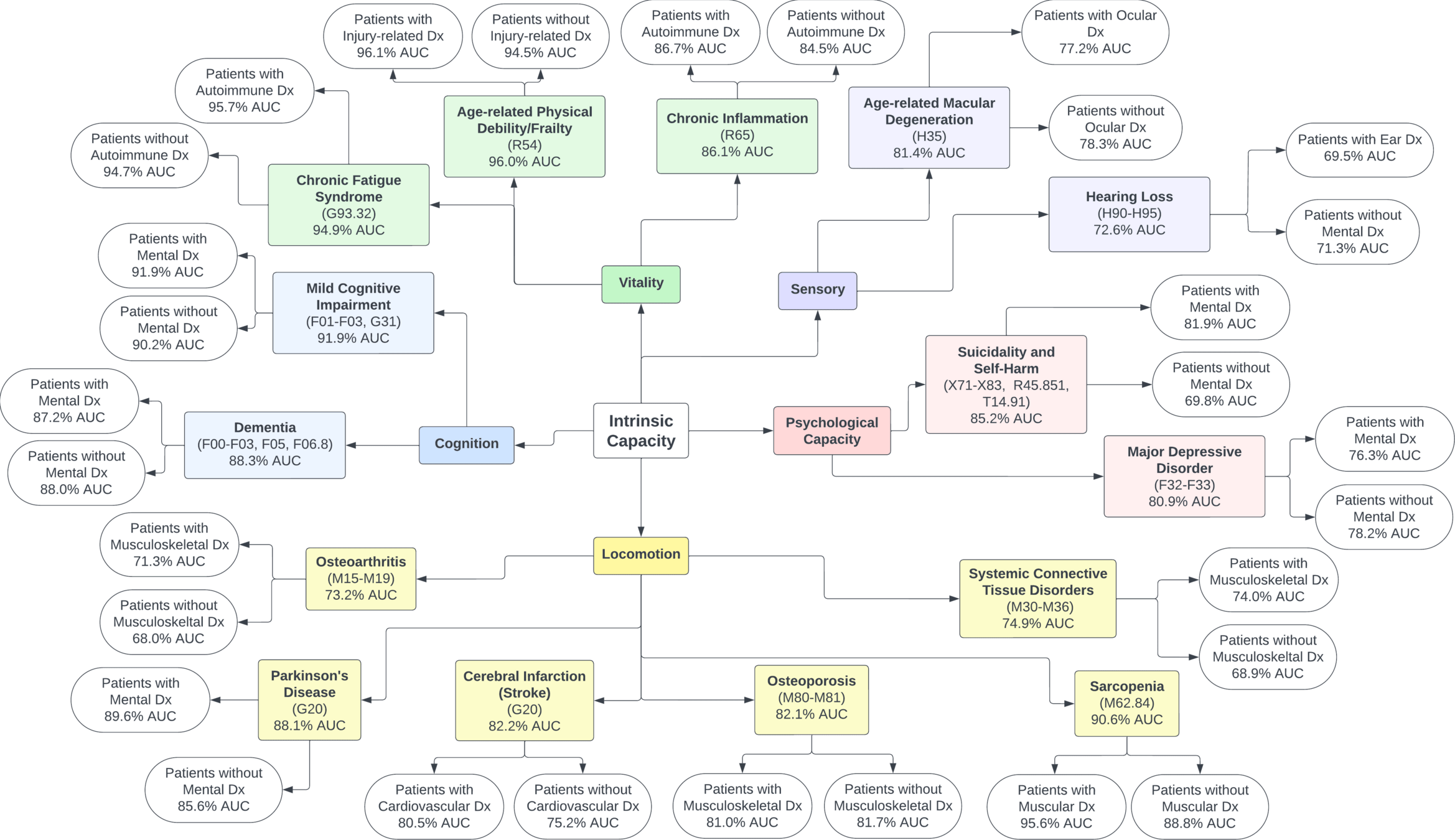
Natural History of Fibrosing ILD

Performance in Claims data

Performance in Claims data