lecture 2:
Basic cardiac arrhythmia and their sources
1. Anatomy of the heart

1. Anatomy of the heart
2. Normal function of the heart
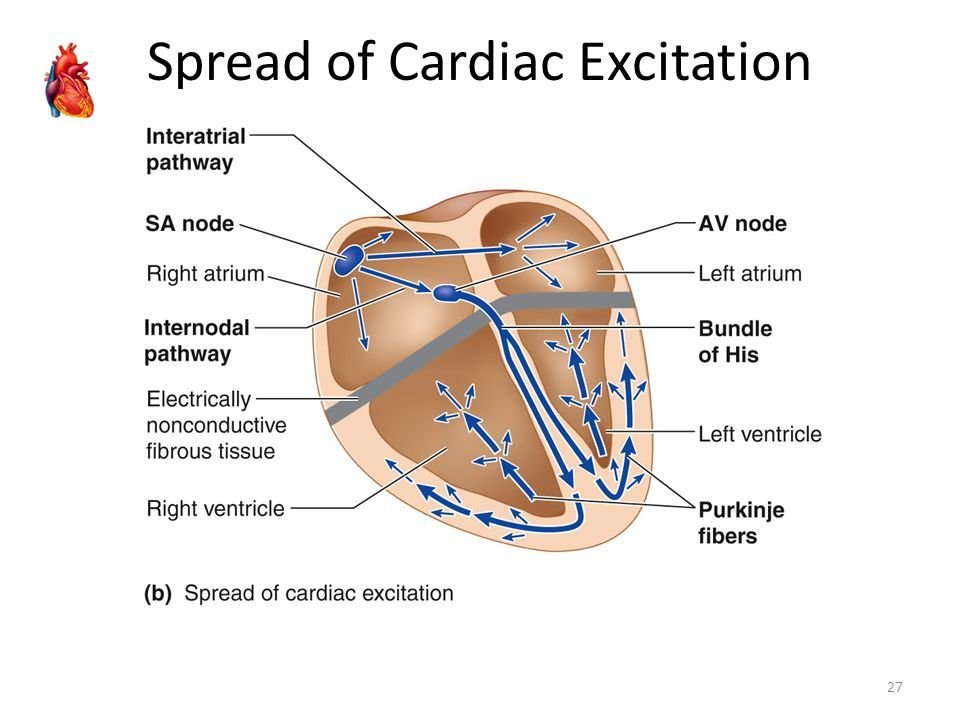
Normal rhythm 60 beats/min: determined by the SA node
=> 100.000 beats per day.
:delay of the signal
2. Normal function of the heart

- conduction of a wavefront
- refraction: during the wavefront: no new wave can be excited
- resting state: new wave can arrive

Single cell
2D tissue
2. Normal function of the heart

Colliding waves annihilate
2. Normal function of the heart
During normal rhythm => ECG


2. Normal function of the heart
2. Normal function of the heart
3. Cardiac arrhythmia

- Ischaemic heart disease: includes sudden cardiac death which is caused by arrhythmias
- Stroke can also be caused by cardiac arrhythmia: e.g. atrial fibrillation
3. Cardiac arrhythmia: 3 main different types of mechanisms
A. Rotors or functional reentry
Rotors are waves of cardiac excitation like a tornado causing cardiac arrhythmia (Pandit and Jalife, Circulation research (2013))
Rotors act like a source and take over the normal rhythm
Anatomical reentry are waves of cardiac excitation rotating around an obstacle (scar tissue, veins, etc )
B. Anatomical reentry
3. Cardiac arrhythmia: 3 main different types of mechanisms
Focal sources are waves with most likely a centrifugal activation pattern
C. Focal sources
3. Cardiac arrhythmia: 3 main different types of mechanisms
3. Cardiac arrhythmia: fast and slow
- Reentry: the period is usually much faster than the period of the SA node and takes over the normal rhythm (mechanism A-B)
- Focal source: can also be very fast, but depends on the type of arrhythmia (mechanism C)
- There exist also slow arrhythmia: bradyarrhytmia, but they have different mechanims
3. Cardiac arrhythmias: treatment
Functional and anatomical reentry

Rotation is only possible is the lenght of the ring (L) is longer than the product of the refracory period and velocity of the wave: L> Rv
3. Cardiac arrhythmias: treatment
Functional and anatomical reentry: drugs
L > Rv
so we need a drug which
increases R: Class III anti-arrhythmtic class
increases v:? Some drugs decrease v
3. Cardiac arrhythmias: treatment
Functional and anatomical reentry: ablation
Ablation: cut the reentry path

3. Cardiac arrhythmias: treatment
Focal source: ablation
Ablation: ablate the source
3. Cardiac arrhythmias: types
A. Supraventricular arrhthymias
A1. Atrial Flutter & Atrial Tachycardia
A2. Atrial fibrillation
A3. AV nodal reentrant tachycardia
etc
3. Cardiac arrhythmias: types
A1. Atrial Tachycardia:
- AT is a regular arrhythmia
- Symptoms may include palpitations, feeling lightheaded, sweating, shortness of breath, and chest pain.
- AT is a common cardiac arrhythmia: incidence of 2.3 per 1000 people. Also, radiofrequency ablation of AF may result in AT.
- Ablation of cardiac arrhythmia is one of the most often performed procedures in cardiac electrophysiology.
- Different types of sources possible for this type of arrhythmia:
- focus
- functional reentry or localized reentry
- macro-reentry

real example of 1 .localized reentry
A1. Atrial Tachycardia

Focal sources (3)
Anatomical reentry (2)
(e.g. reentry around mitral valve)

A1. Atrial Tachycardia
-
Atrial fibrillation (AF): will be the most common disease in the West causing a sixfold increase in stroke risk, leading to anxiety, depression, and reduces individuals' quality of life
-
Treatment: ablation: burning away different areas of the heart: only about 50% success rate!
-
Reason for poor success: the underlying mechanism is heatedly debated
-
Is AF due to rotors? World leading groups have opposing views:


A2. Atrial fibrillation
-
Treatment is unclear:
-
E.g. FIRM (Focal Impulse and Rotor Modulation) approach is being used in the clinical practice to detect rotors by using phase mapping (Narayan et at J Am Coll Cardiol, 2014)
-
Initially very high success rates (90%) were reported for patients with persistent AF.
-
The company which developed FIRM for clinical practice (Topera Inc.) was sold for 250 million dollar to Abbott
-
However, newest results show that FIRM does not work, results are again back to 50% success rate for persistent AF
A2. Atrial fibrillation
A2. Atrial fibrillation
A2. Atrial fibrillation
A2. Atrial fibrillation
B. Ventricular arrhthymias
B1. Ventricular tachycardia
B2. Ventricular fibrillation
3. Cardiac arrhythmias: types
4. Computer modeling: integrative model of the human heart

4. Computer modeling: integrative model of the human heart

- Velocity (value,+-)
- How initiate wave
- Spiral properties (wavelength,period)
- Vortex dynamics + chaos
- Mechanisms of initiation of spirals
- Control (remove from the heart)
- Not only heart