Applied Econometrics and Natural Experiments
Economic effects
The goal of applied research is often to identify the impact of some economic effect or policy. For example:
- Did the jobs training program make workers more productive?
- Did the public health intervention lower the unemployment rate?
- If credit card companies disclose their annualized interest rates, do consumers borrow less?
Economic effects
- Did the jobs training program make workers more productive? The most proactive workers decided to get more training...
- Did the public health intervention lower the unemployment rate? States that undertook public health interventions also made other investments to grow the economy...
- If credit card companies disclose their annualized interest rates, do consumers borrow less? Only companies with favorable rates choose to disclose...
The big challenge is that the companies or people who get/use these types of interventions might be systematically different than one another...
Economic effects
We call the fact that different types of people tend to get different types of treatments/interventions the "selection effect."
For your own setting, ask yourself:
why did some companies do this and other companies did not?
how did these decisions get made?
what is the process for people getting a treatment or intervention?
An "Effect" or just selection?
When the people who get vs refuse an intervention are systematically different, it's hard to know what the effect would be in the absence of the intervention.
Sick people tend to be in the hospital.
But going to the hospital doesn't make you sicker.
Safe to say that going to the hospital usually makes you healthier!
Need the counterfactual.
What would happen to the exact same people if they DIDN'T receive the treatment/intervention
How to find the counterfactual?
Causal effect of a "treatment": What would have happened if the treatment never took place?
Ways of finding the counterfactual:
- A/B testing: randomize who gets vs doesn't get some intervention
- Not always ethical!
- Compare companies who got an intervention to those who we know are similar (but how to be sure?)
- Look before and after in the same company (but are you sure other things are not changing?)
You might need to get creative!
Goals of the ACA
•Expand insurance coverage
•Reduce the growth of health spending
•Strengthen quality incentives
Builds on the existing system of private insurance.
What was Coverage Like Before the ACA?
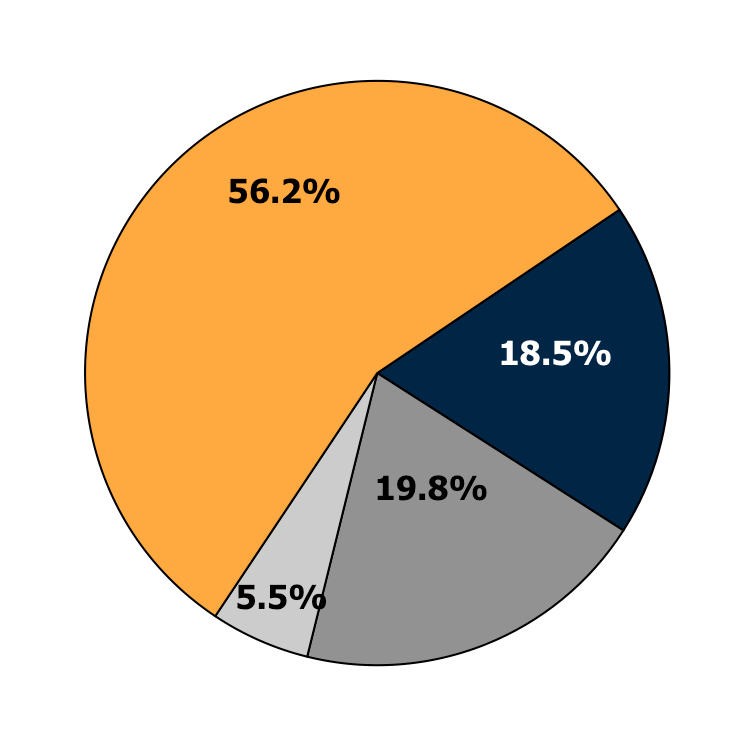
Employer-Sponsored
Health Insurance
Private Non-Group
Medicaid or other
public programs
Uninsured
Source: 2011 CPS ASEC, Non-Elderly Only
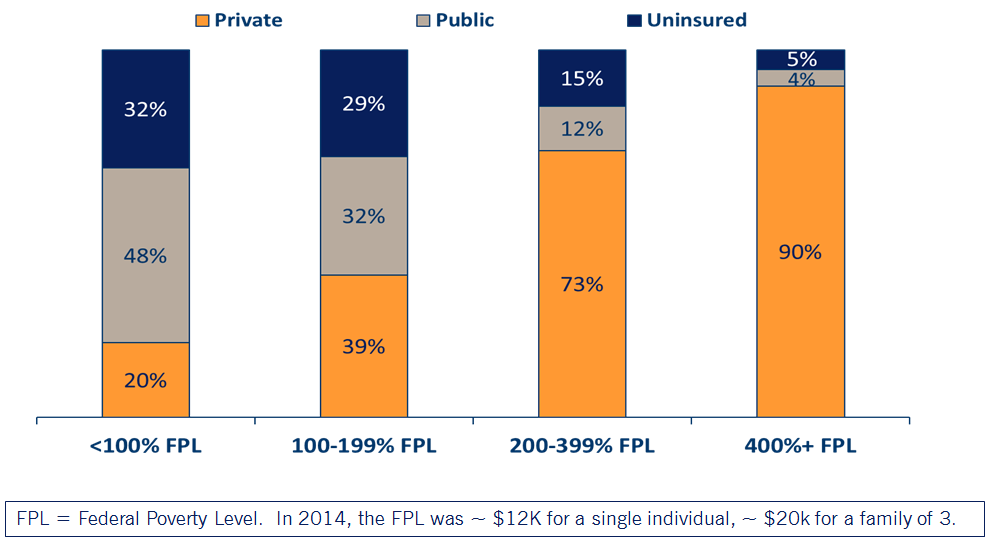
Health Insurance by Income Level
ACA Expanded Coverage in 3 Ways
1.Young adults allowed to stay on their parents’ private insurance until age 26 (effective September 2010)
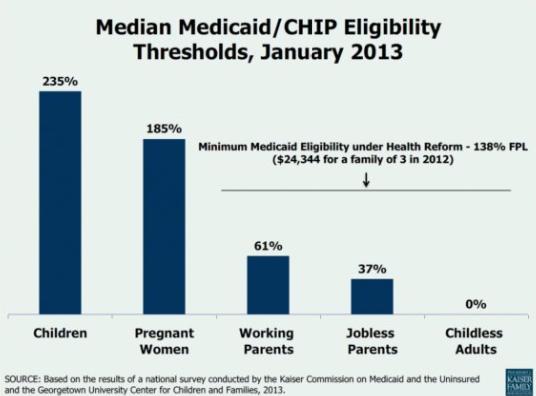
2.Eligibility for Medicaid extended to everyone with incomes below 138% of the Federal Poverty Level (effective Jan 2014*)
3.New tax credits for private insurance for families between 100 and 400% of the Federal Poverty Level (effective Jan 2014)
* Several states elected to expand Medicaid at different times, or not at all!
Medicaid Expansion
NFIB v Sibelius 2012
High profile supreme court case challenging constitutionality of the ACA:
SCOTUS ruled the threat of losing all Medicaid funding was unconstitutionally coercive, a "gun tot he head" as Roberts wrote in his majority opinion.
Because of this ruling, states could opt not to expand Medicaid without risking losing additional funding.
Also gave states some negotiating power to expand on their terms.
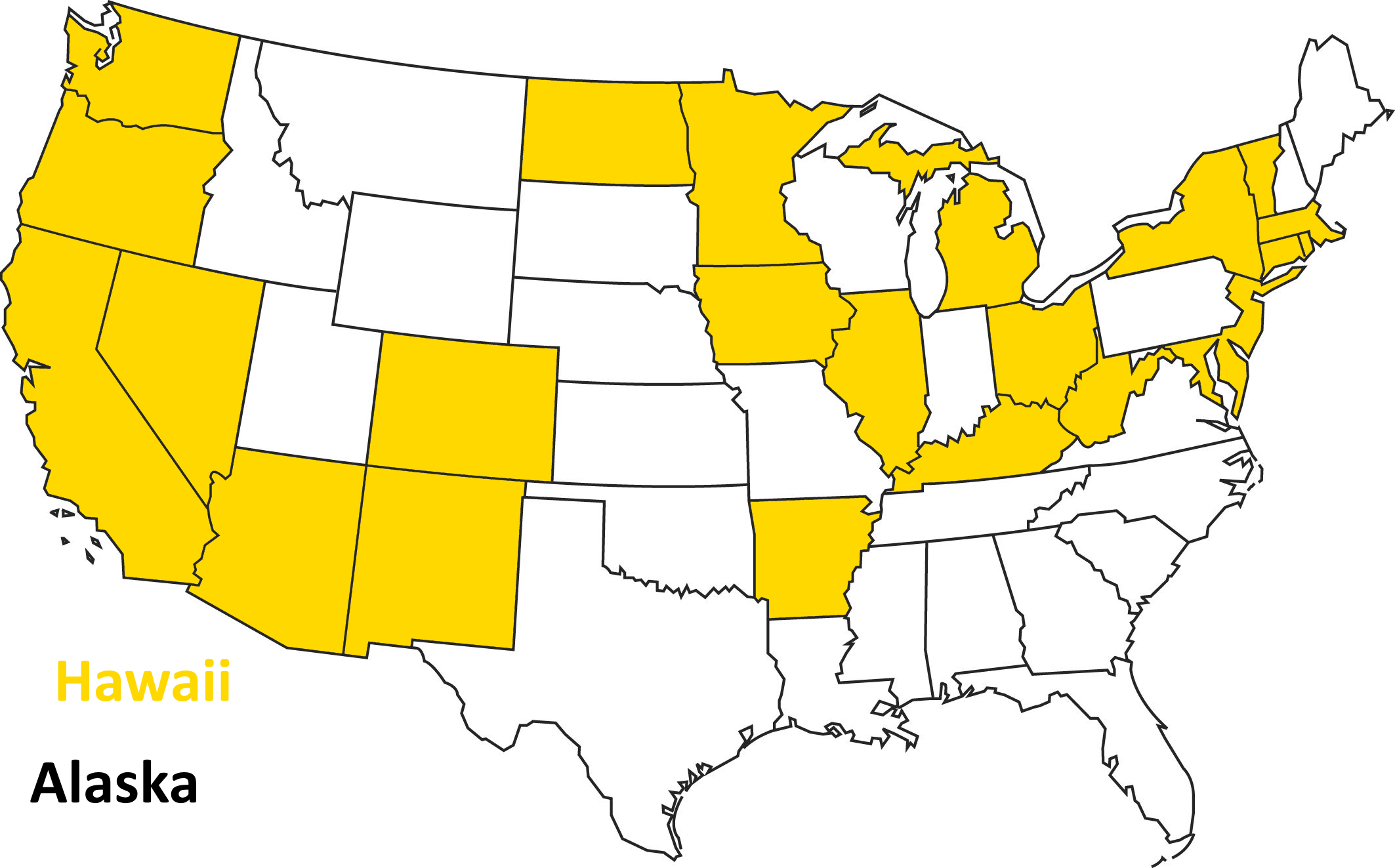
Opted to Expand in 2014
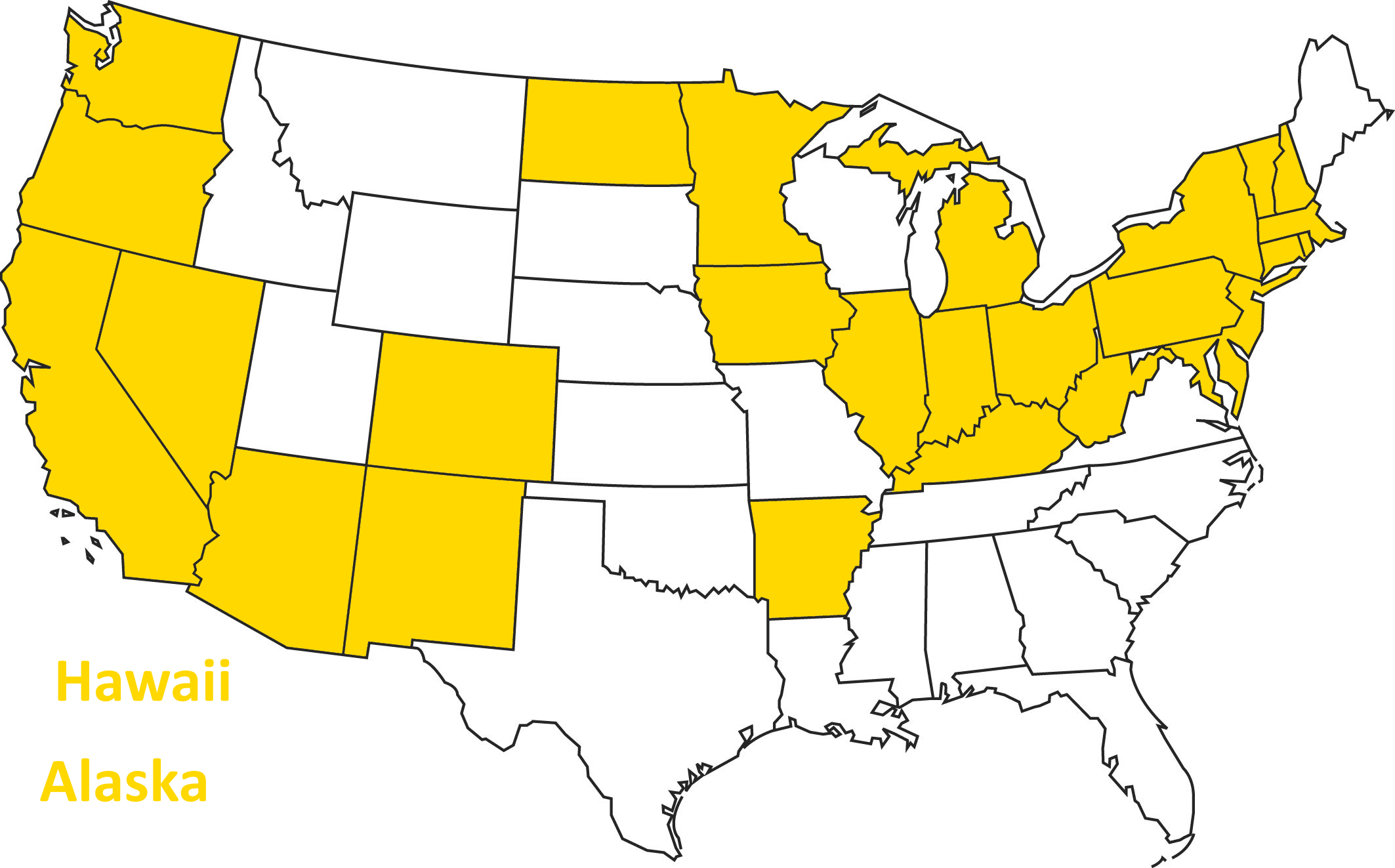
As of 2015...
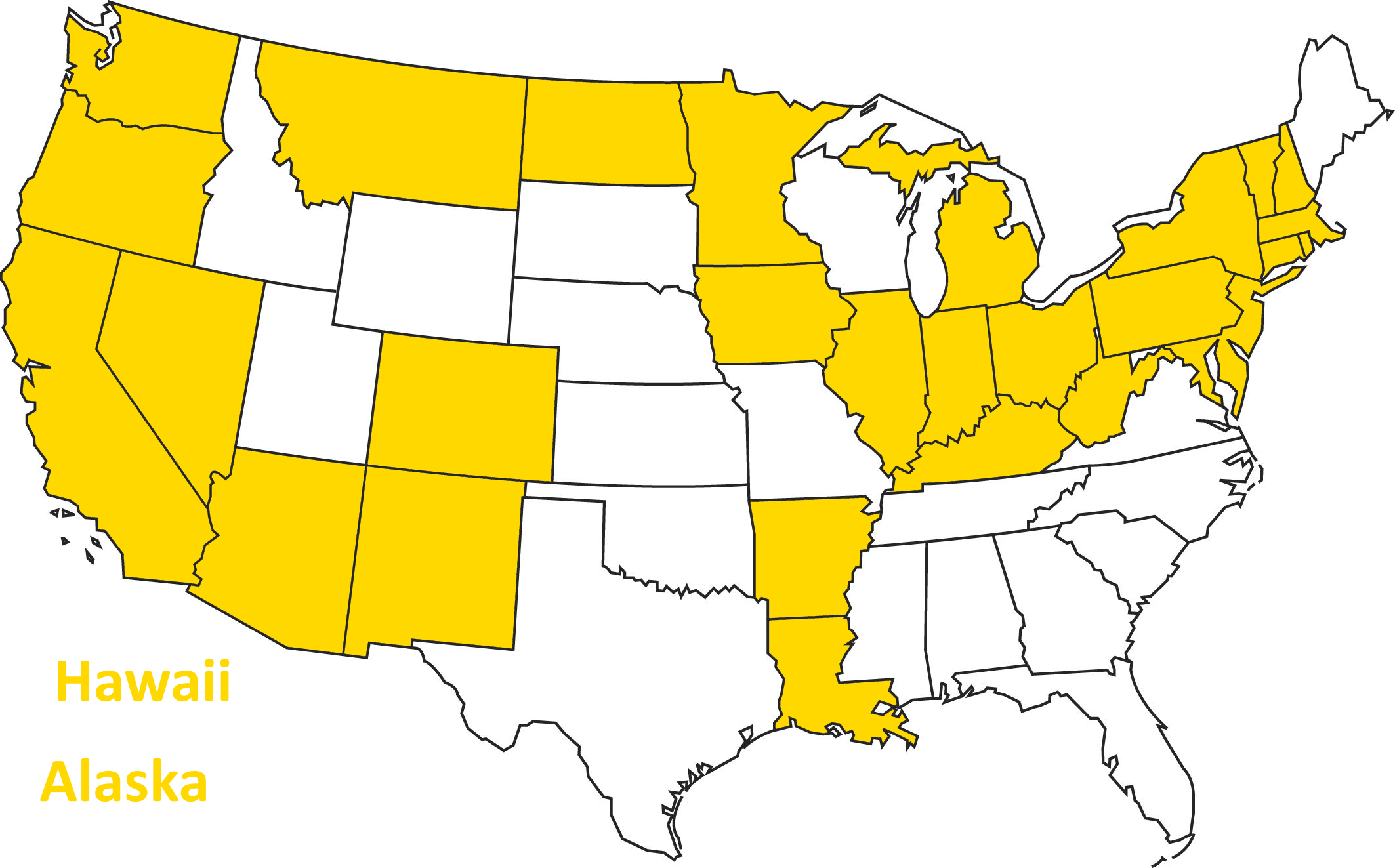
As of 2016...
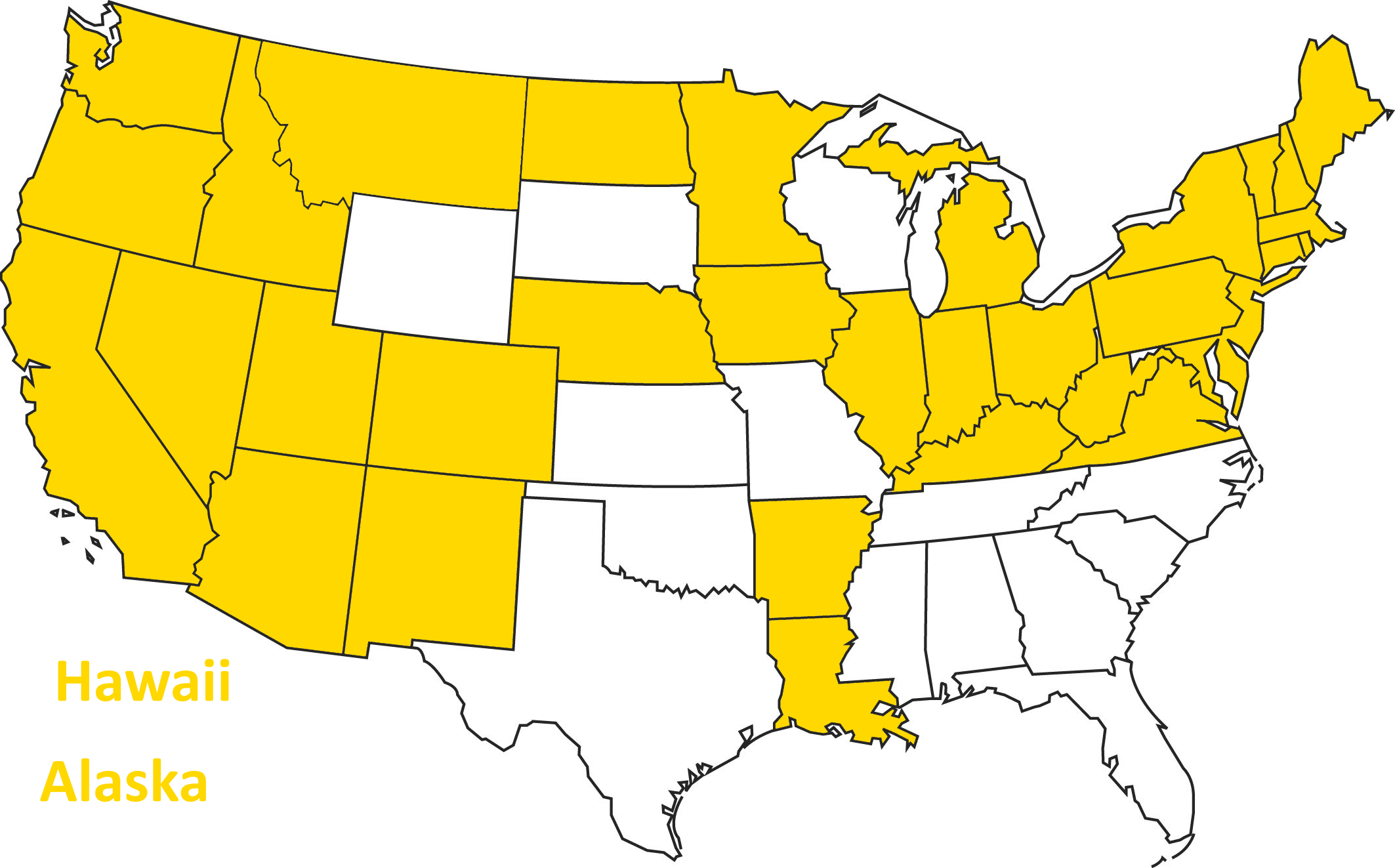
Today
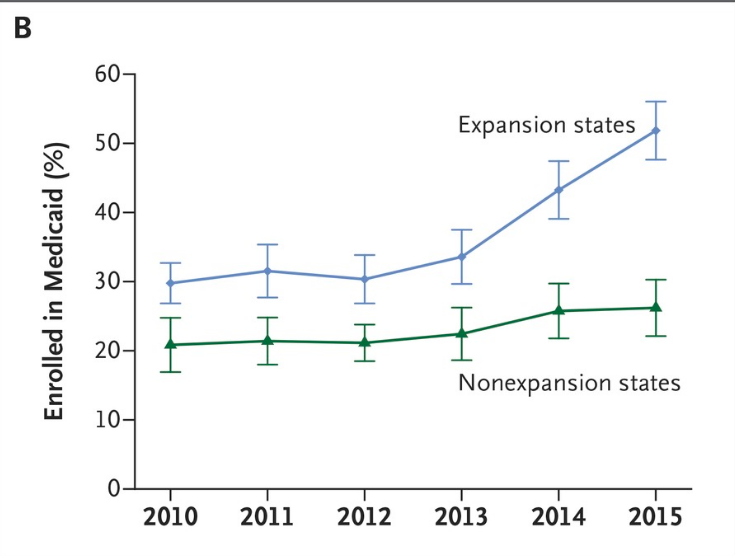
Coverage Gains Largest in states that expanded Medicaid
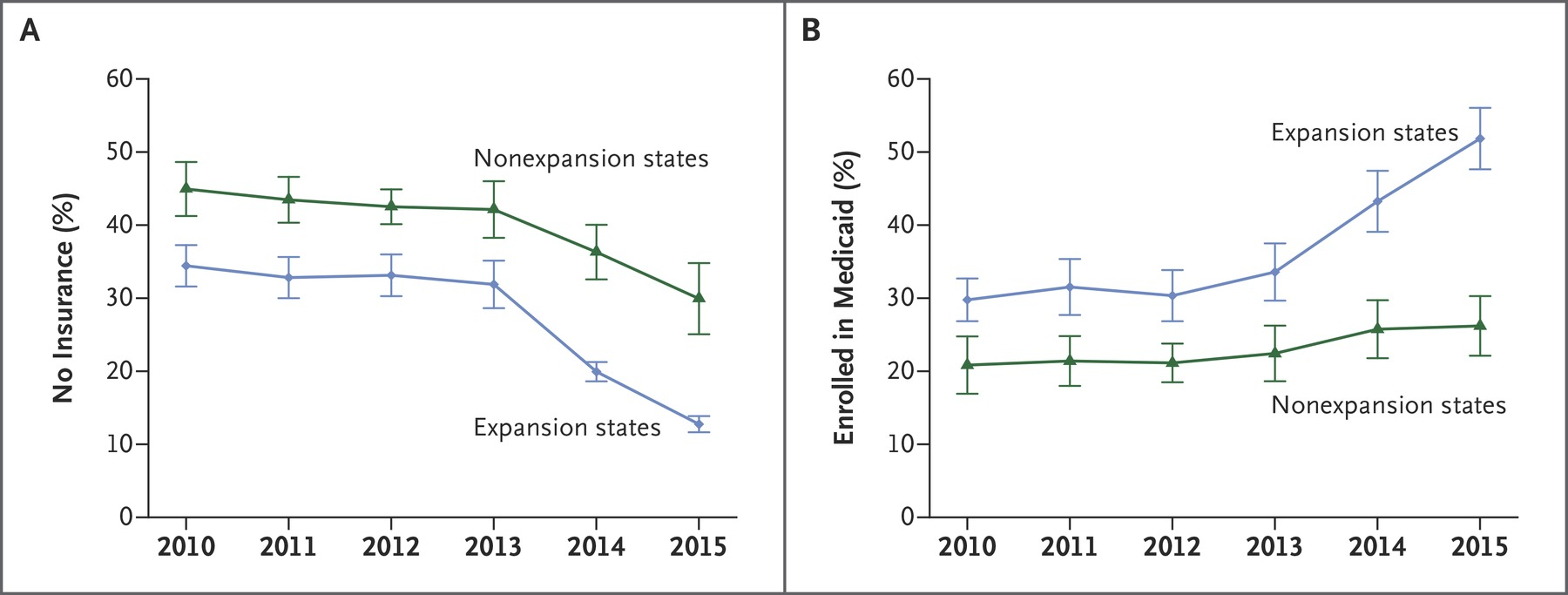
Sample among low income adults, Miller and Wherry 2016 New England Journal of Medicine
Analysis of ACA Medicaid Expansions
- Take advantage of non-universal adoption of the Medicaid expansion that resulted from the 2012 Supreme Court decision.
- Use a "difference in differences" quasi-experimental empirical design
Compare changes in outcomes across expansion and non-expansion states.
Expansion states and non-expansion states might be at different levels, but are they on the same trajectory?
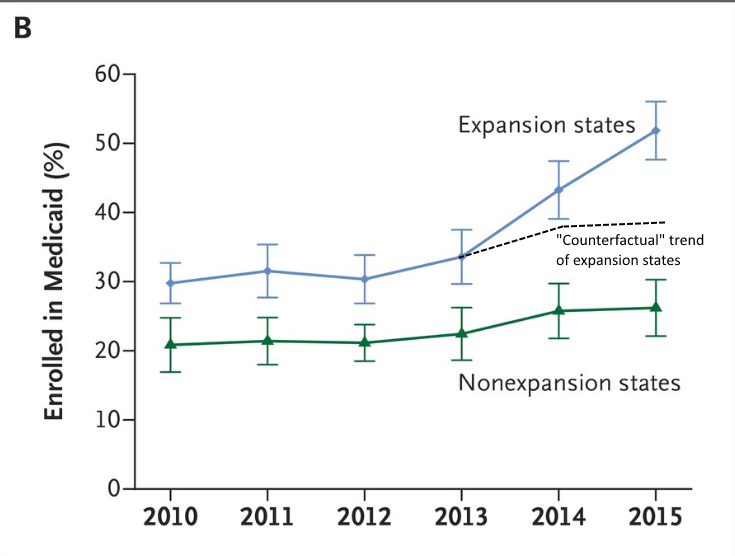
Difference in Differences
Let's go back to this figure:
Difference in Differences
Let's go back to this figure:
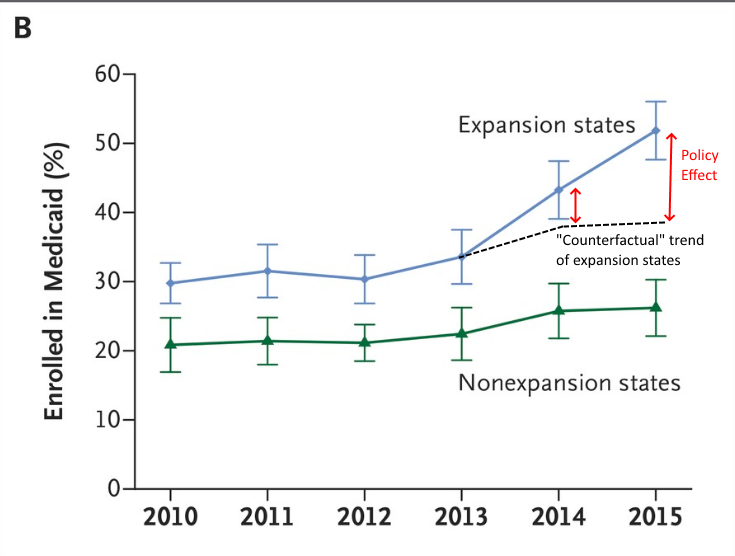
Difference in Differences
Let's go back to this figure:
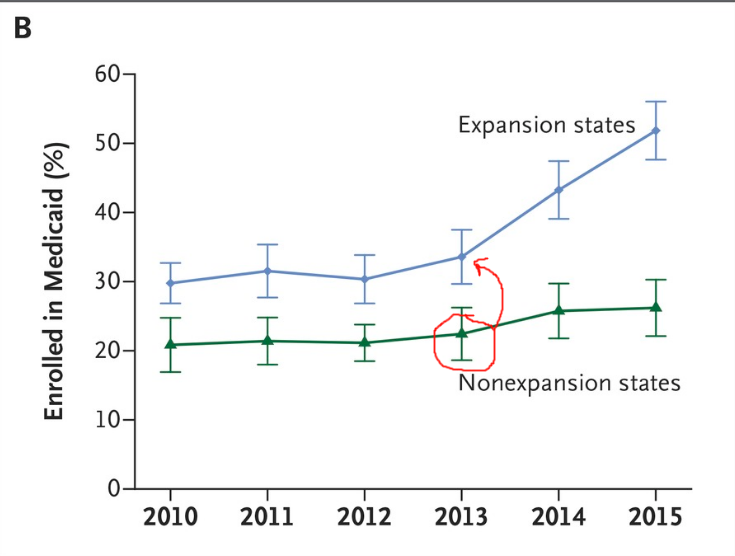
Difference in Differences
Let's go back to this figure:
Difference in Differences
One way to represent this would be to subtract out the difference in one year (normalize to zero) and then plot the remaining difference.
Difference in Differences
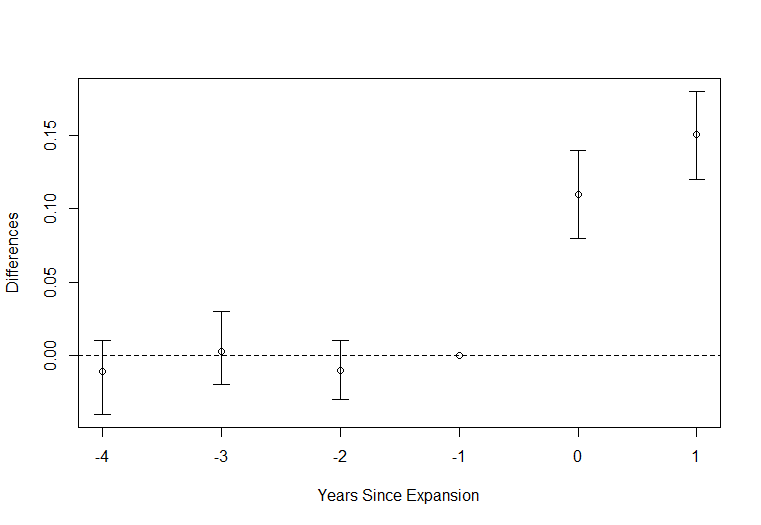
Difference in Differences
"Are you worried about medical bills?"
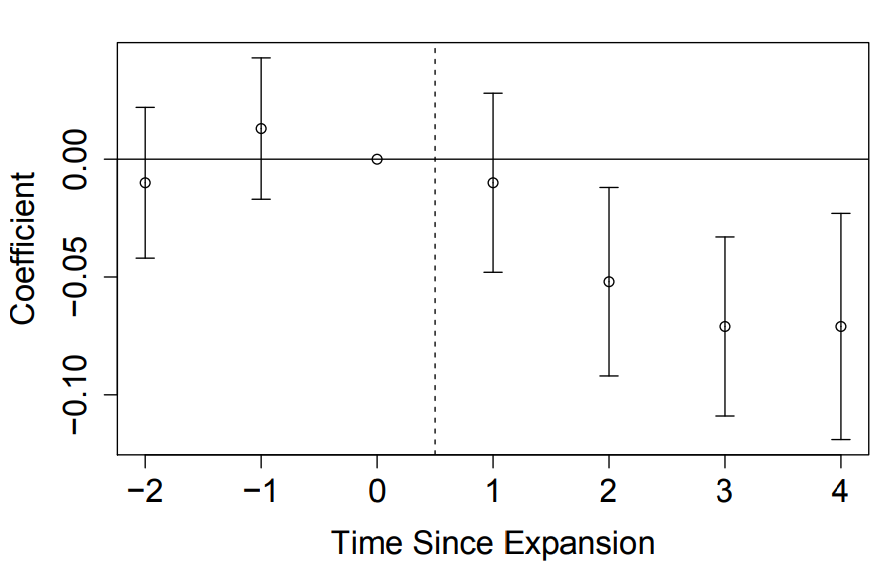
Difference in Differences

"Are you unable to afford necessary medical care?"
Difference in Differences
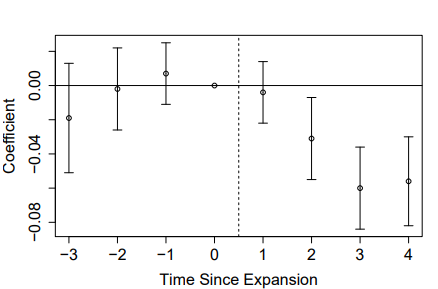
"Did you delay medical care due to costs?"
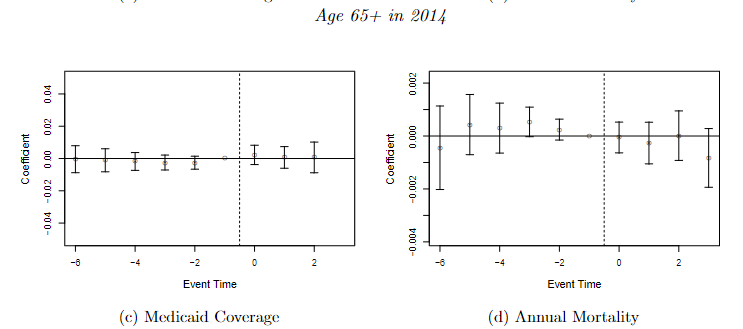
Mortality
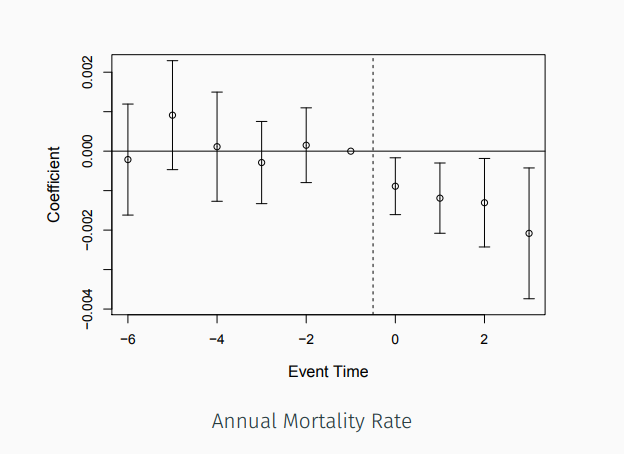
Probability of mortality for all who were alive at the beginning of the year (age 55+)


"Placebo" Test
Where to find data?
American Community Survey: Employment, earnings, occupation, demographics, education
National Health Interview Survey: Health care access, health, mental health, insurance coverage
Bureau of Labor Statistics: State and county characteristics such as unemployment rate
Center for Disease Control/National Center for Health Statistics: Disease prevalence