Evaluating The Affordable Care Act Medicaid Expansions
Goals of the ACA
•Expand insurance coverage
•Reduce the growth of health spending
•Strengthen quality incentives
Builds on the existing system of private insurance.
What was Coverage Like Before the ACA?
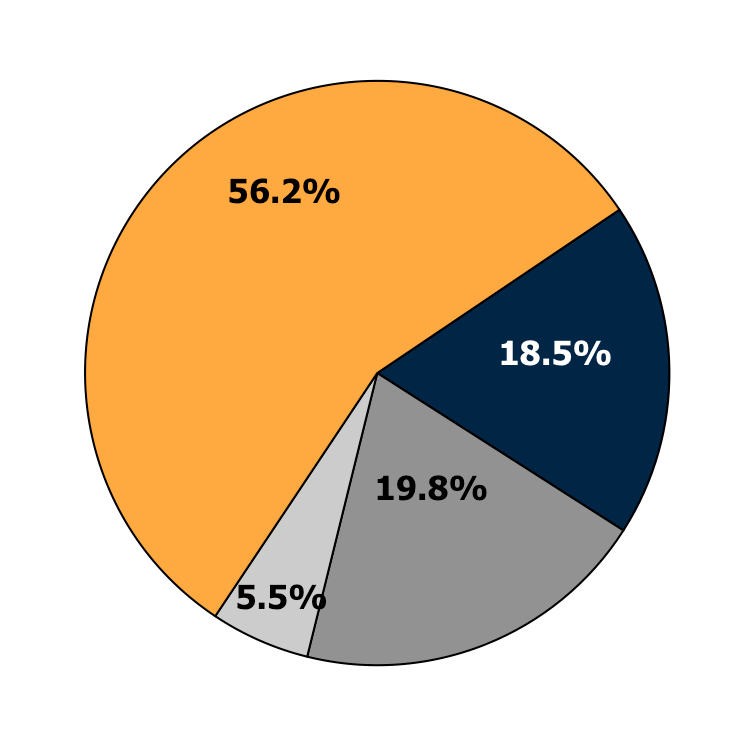
Employer-Sponsored
Health Insurance
Private Non-Group
Medicaid or other
public programs
Uninsured
Source: 2011 CPS ASEC, Non-Elderly Only
Declines in Coverage
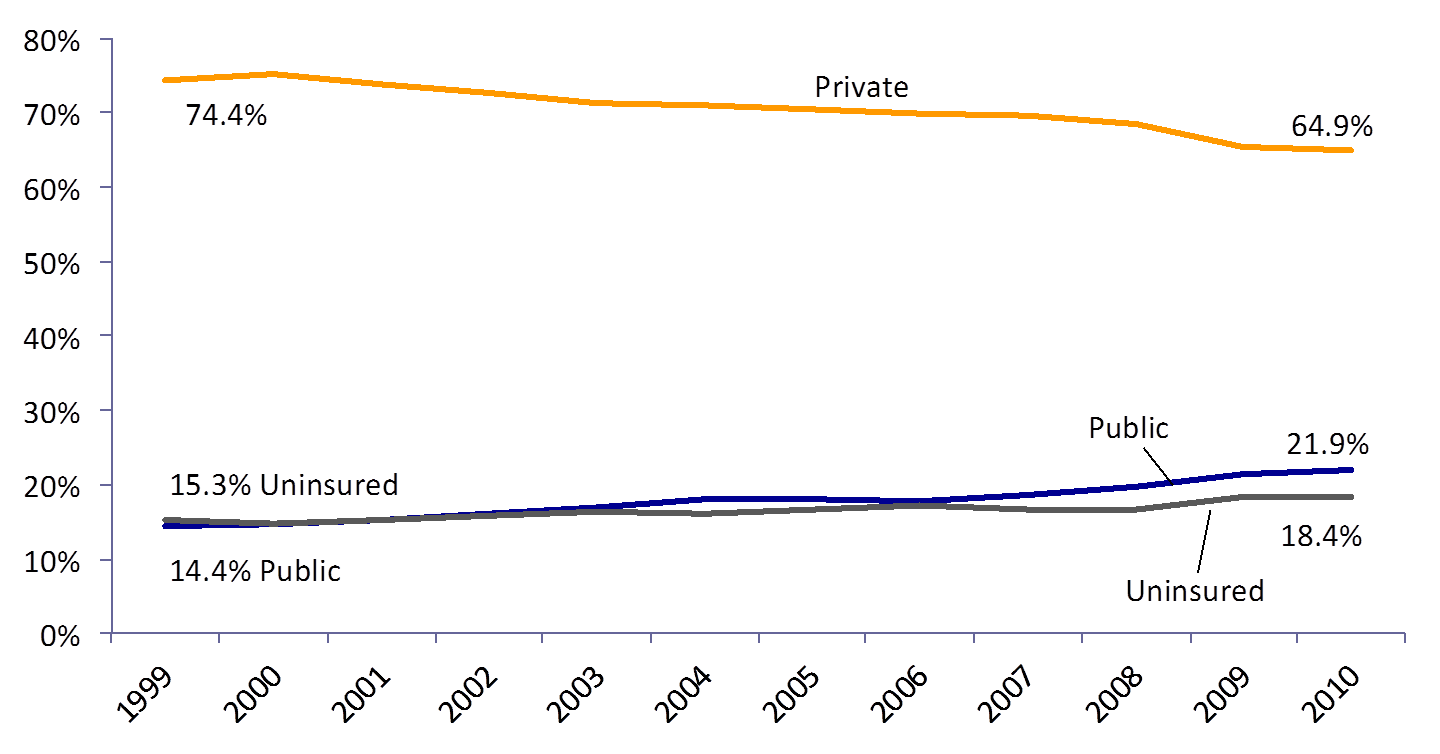
Source: DeNavas-Walt et al. Income, Poverty and Health Insurance Coverage in the United States: 2011, US Census Bureau (2012)
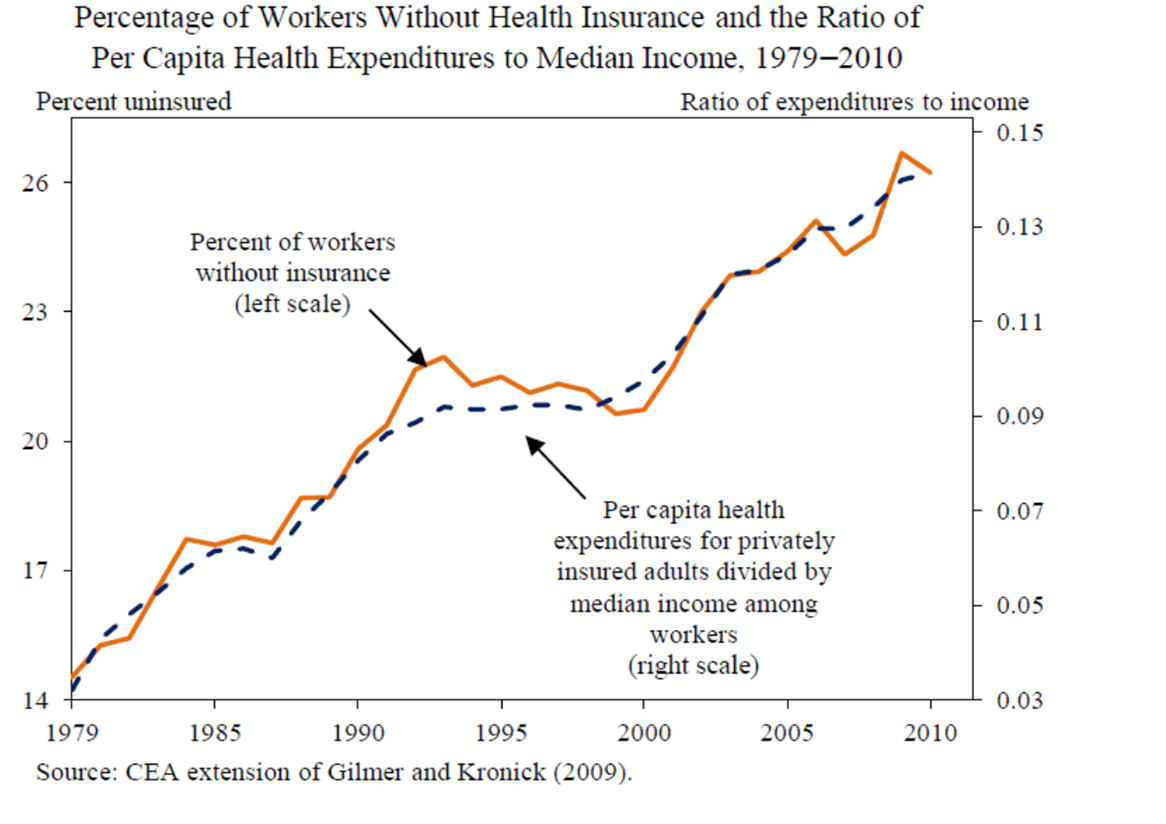
Cost Growth Drove Declines in Coverage
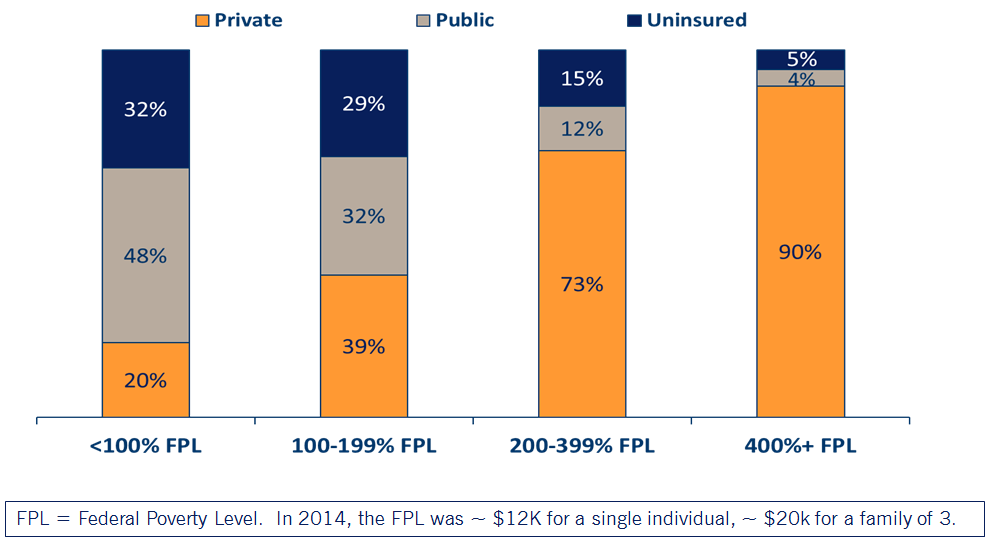
Health Insurance by Income Level
ACA Coverage Provisions
ACA Expanded Coverage in 3 Ways
1.Young adults allowed to stay on their parents’ private insurance until age 26 (effective September 2010)
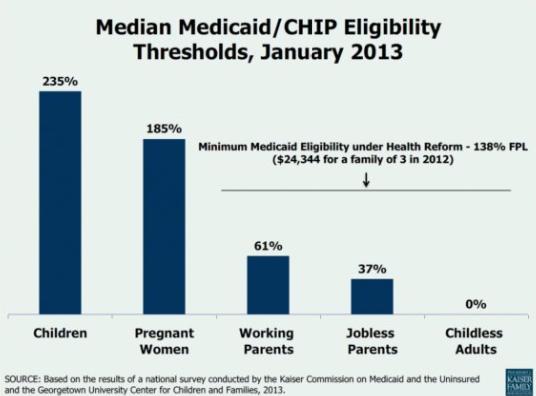
2.Eligibility for Medicaid extended to everyone with incomes below 138% of the Federal Poverty Level (effective Jan 2014*)
3.New tax credits for private insurance for families between 100 and 400% of the Federal Poverty Level (effective Jan 2014)
* Several states elected to expand Medicaid at different times, or not at all!
Medicaid Expansion
Medicaid Expansion
How does the government plan to expand Medicaid?
- Federal match assistance percentage (FMAP): States were historically guaranteed at least a 1-to-1 match from federal government.
- Higher match rate for lower income states (highest is MS, 2.8 to 1 in 2015)
- Under ACA, federal government pays 100% of additional costs during 2014-2016, then phases down to 90% by 2020.
- Under the original law, states have to expand Medicaid or risk losing all of their funding
NFIB v Sibelius 2012
High profile supreme court case challenging constitutionality of the ACA:
SCOTUS ruled the threat of losing all Medicaid funding was unconstitutionally coercive, a "gun tot he head" as Roberts wrote in his majority opinion.
Because of this ruling, states could opt not to expand Medicaid without risking losing additional funding.
Also gave states some negotiating power to expand on their terms.
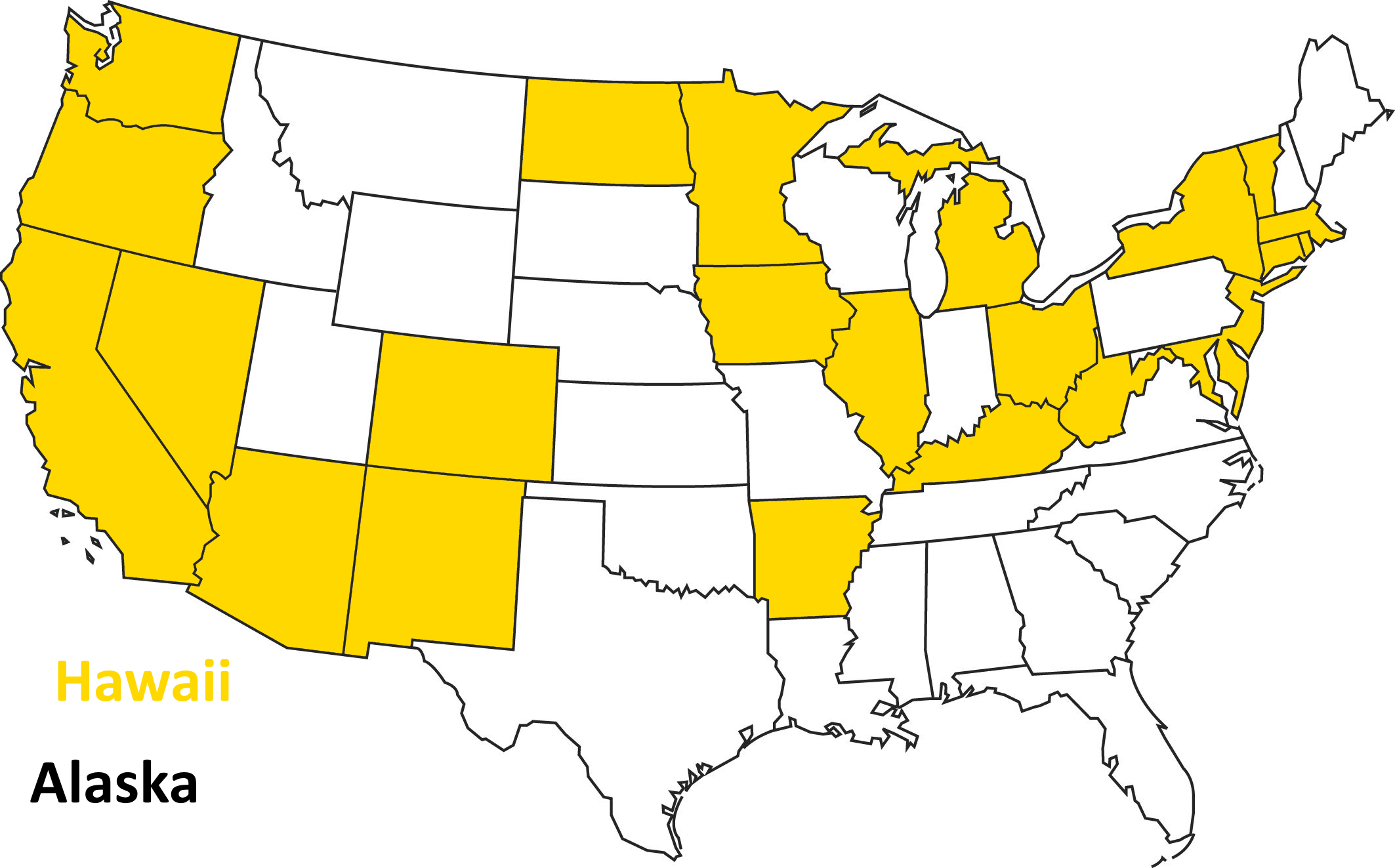
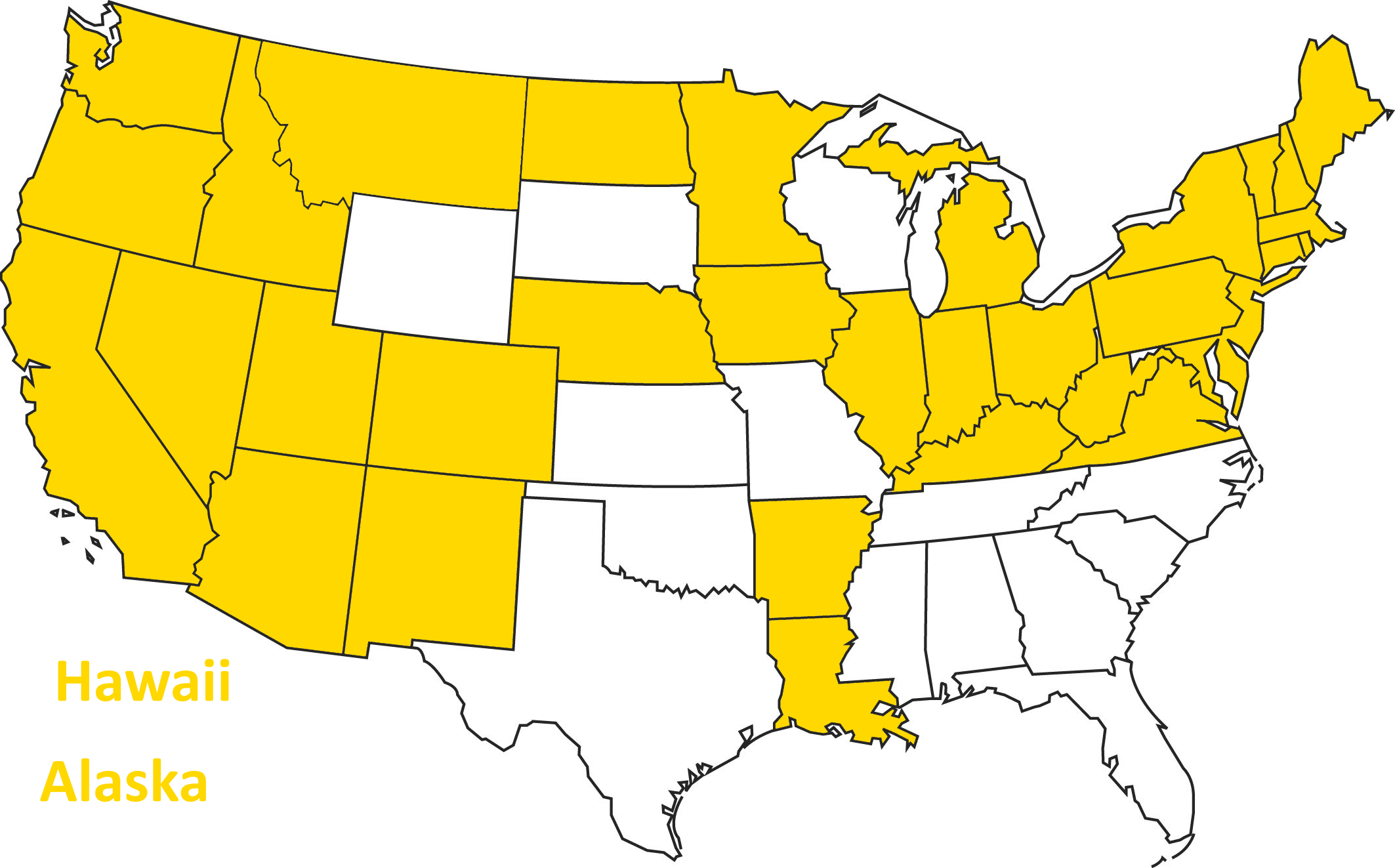
Opted to Expand in 2014
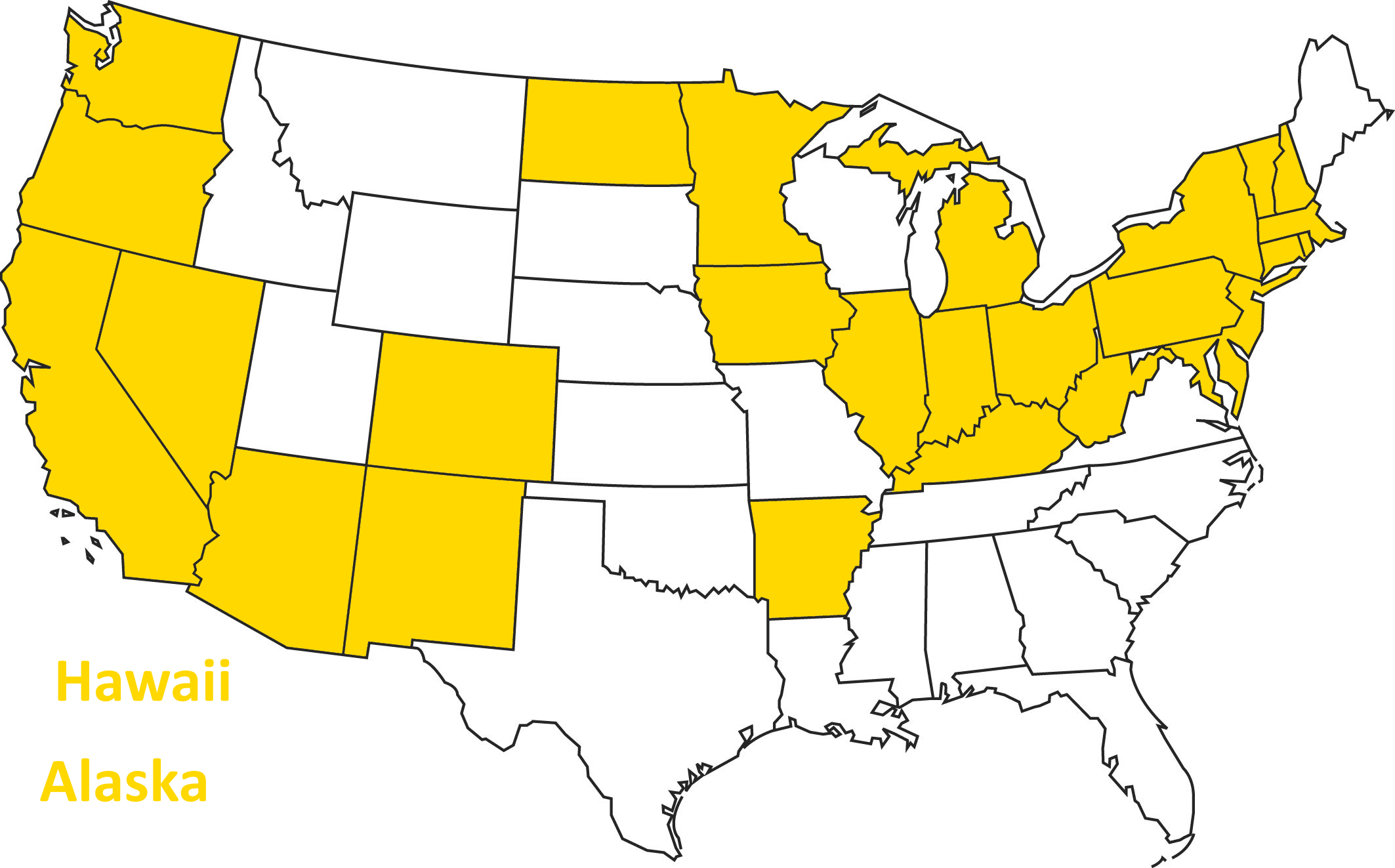
As of 2015...
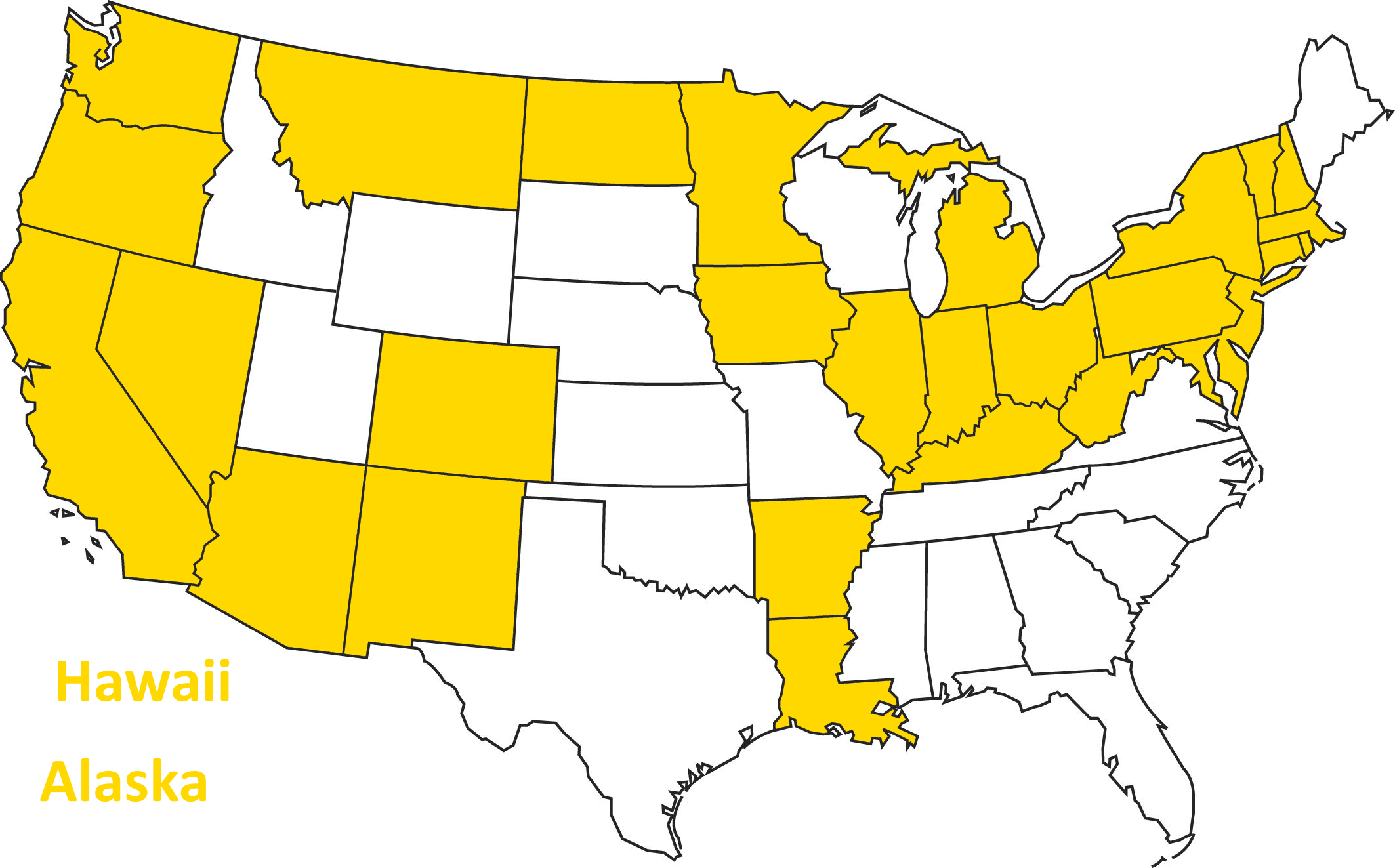
As of 2016...
Today
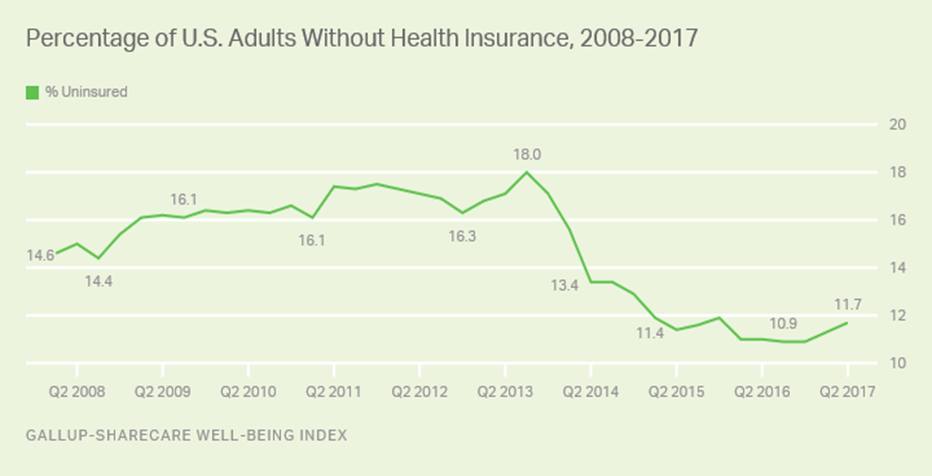
Overall Coverage Gains
The number of people with insurance increased by 20 million between 2010 and 2015
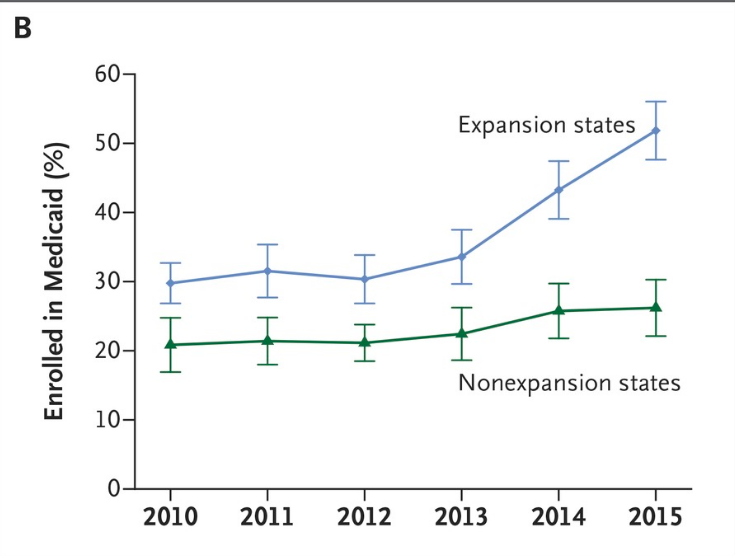
Coverage Gains Largest in states that expanded Medicaid
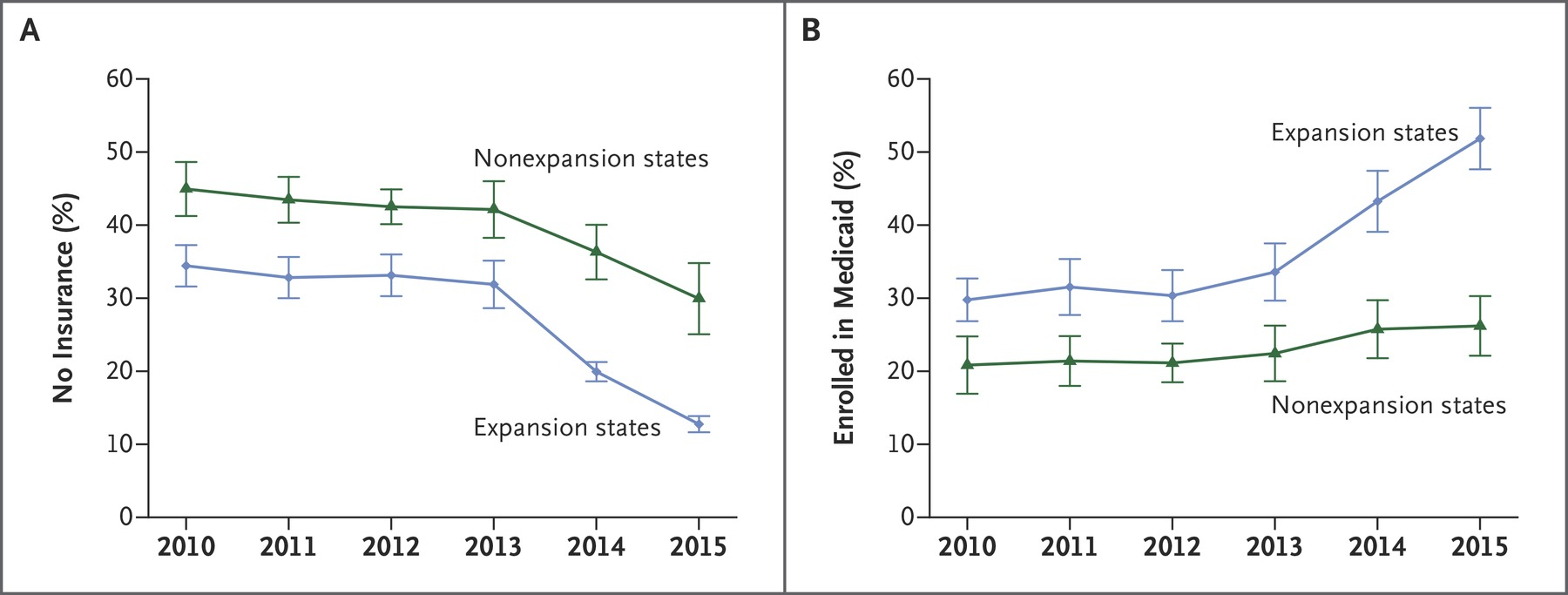
Sample among low income adults, Miller and Wherry 2016 New England Journal of Medicine
Analysis of ACA Medicaid Expansions
- Take advantage of non-universal adoption of the Medicaid expansion that resulted from the 2012 Supreme Court decision.
- Use a "difference in differences" quasi-experimental empirical design
Compare changes in outcomes across expansion and non-expansion states.
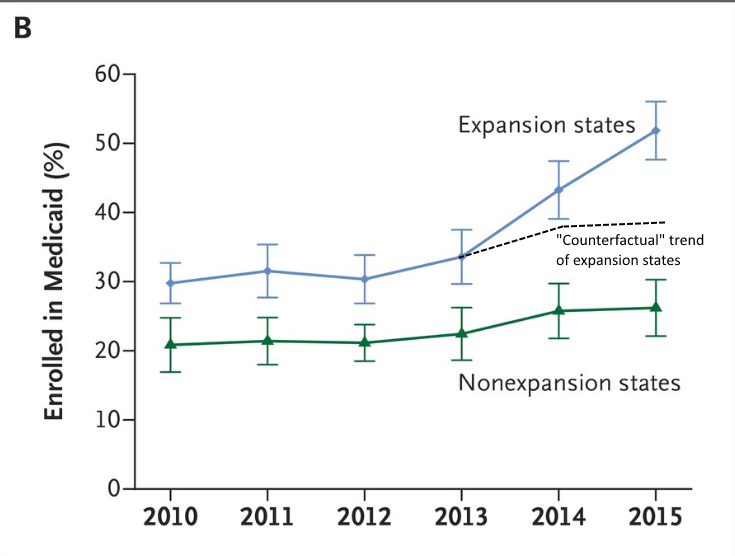
Expansion states and non-expansion states might be at different levels, but are they on the same trajectory?
Difference in Differences
Let's go back to this figure:
Difference in Differences
Let's go back to this figure:
Difference in Differences
Let's go back to this figure:
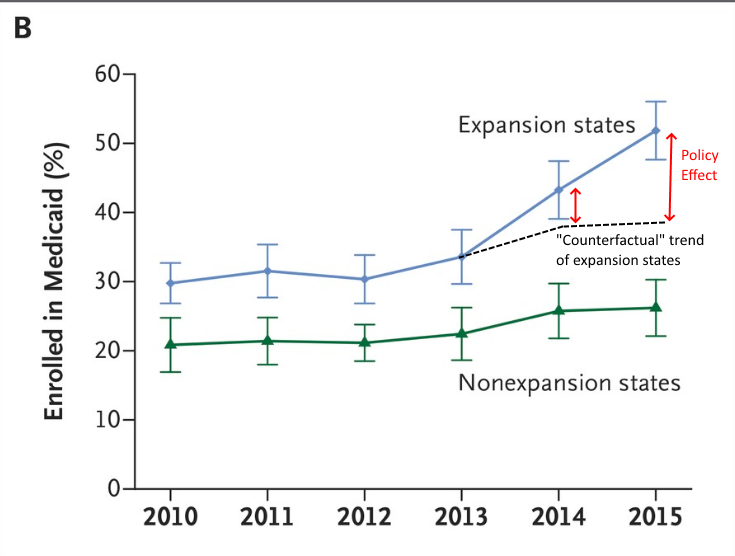
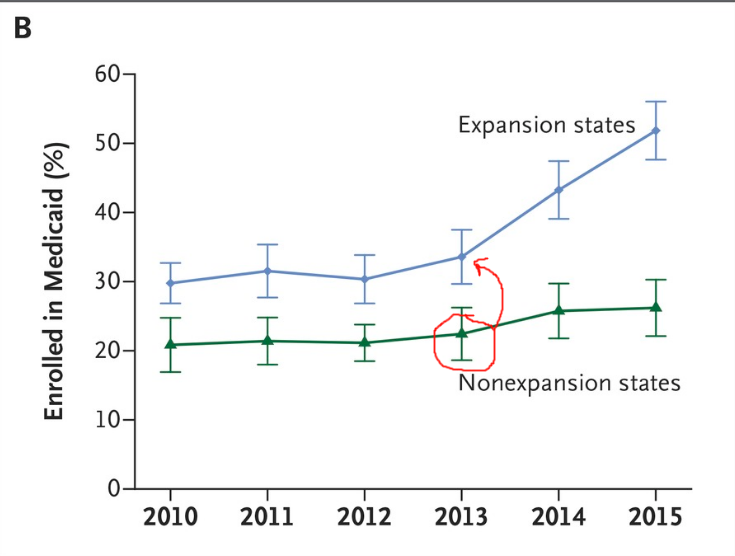
Difference in Differences
Let's go back to this figure:
Difference in Differences
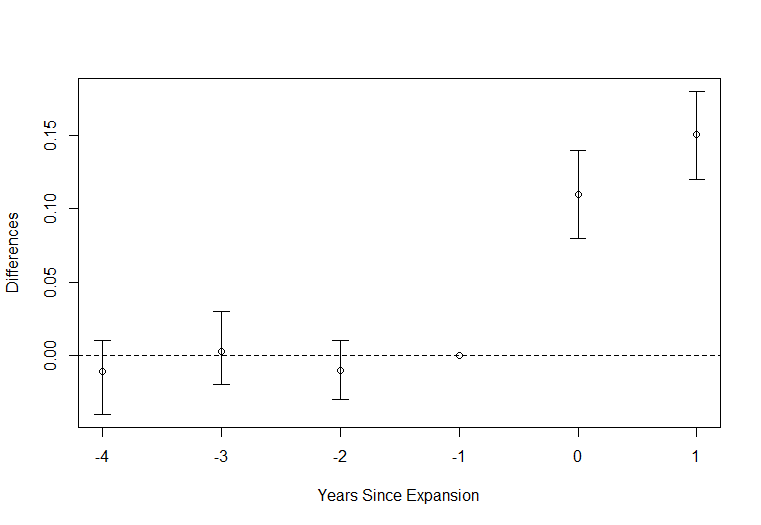
One way to represent this would be to subtract out the difference in one year (normalize to zero) and then plot the remaining difference.
Difference in Differences
Mortality Impacts of ACA Medicaid Expansions
Context
High degree of inequality in health outcomes by income.
- 55-64 year olds in households earning under 138 FPL have annual mortality rate of 1.7pp. In households earning 400%FPL+: 0.4pp. 4x higher for low income households.
- 787% higher chance of dying from diabetes, 552% higher chance of dying from cardiovascular disease, 813% higher chance of dying from respiratory disease.
- Correlation between income and health exists in all countries, correlation is higher in the US than in other wealthy countries (Semyonov, Lewin-Epstein and Maskileyson 2013).
Could the Medicaid expansions help reduce these very high mortality rates?
Data Challenge
Typically data on mortality does not contain information on socio-economic characteristics such as income or insurance coverage.
- Makes it difficult to analyze mortality impact of Medicaid because you don't know who would actually be eligible.
Mortality is not a very common outcome for the non-elderly (elderly are covered by Medicare already so not relevant).
- You need a really big sample to have enough statistical power.
Data Solution
Solution for this paper: link data from American Community Survey (ACS) to Social Security Administration mortality records
- ACS is large survey (4 to 4.5 million respondents per year) and has information on household income, eligibility for other programs, and other information relevant to determine who is most likely to gain eligibility
- We focus on individuals age 55-64, low income or disadvantaged (no high school degree), not otherwise Medicaid eligible, citizens.
- A large % of this group gained Medicaid eligibility.
- Follow this group across expansion and non-expansion states for 4 years after the ACA expansions.
How Many Gained Eligibility?
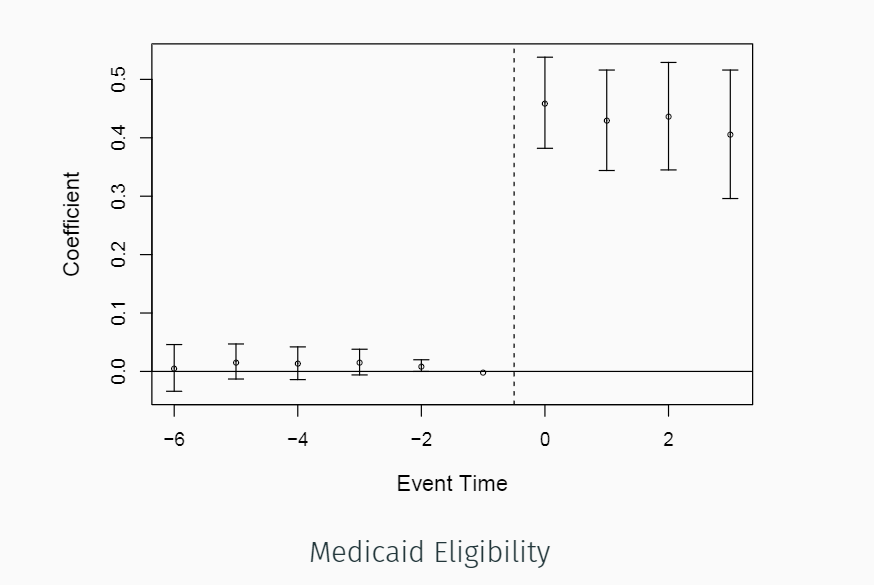
Nearly half of the group gained eligibility
How Many Gained Eligibility?
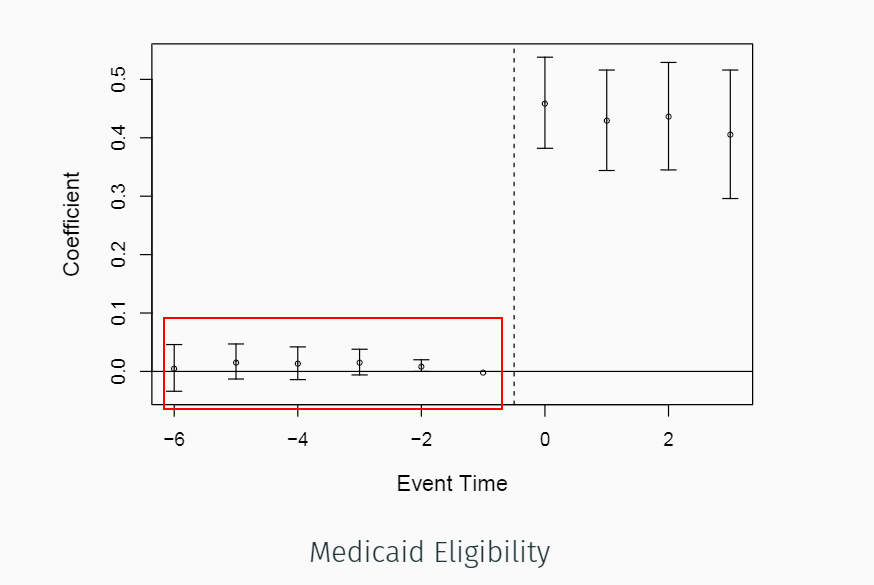
Notice! What does this tell us?
How Many Enrolled?
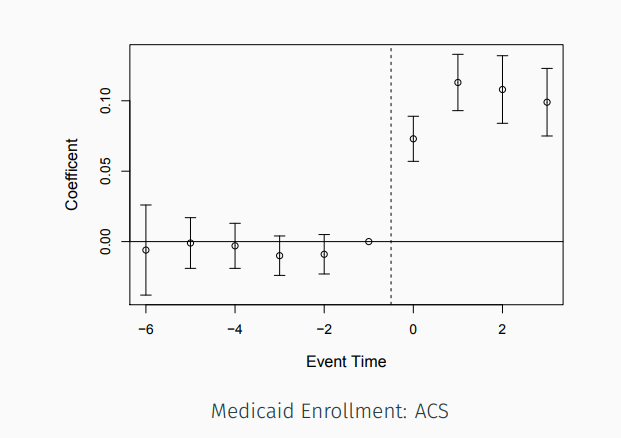
About 10-11percent enrolled, possibly higher due to misreporting in survey
Takeaway?
In the paper, we show this for other measures and other surveys (NHIS) as well.
- Successfully identified a group that was highly impacted by Medicaid expansions.
- ACA policy had meaningful impact on coverage for this group.
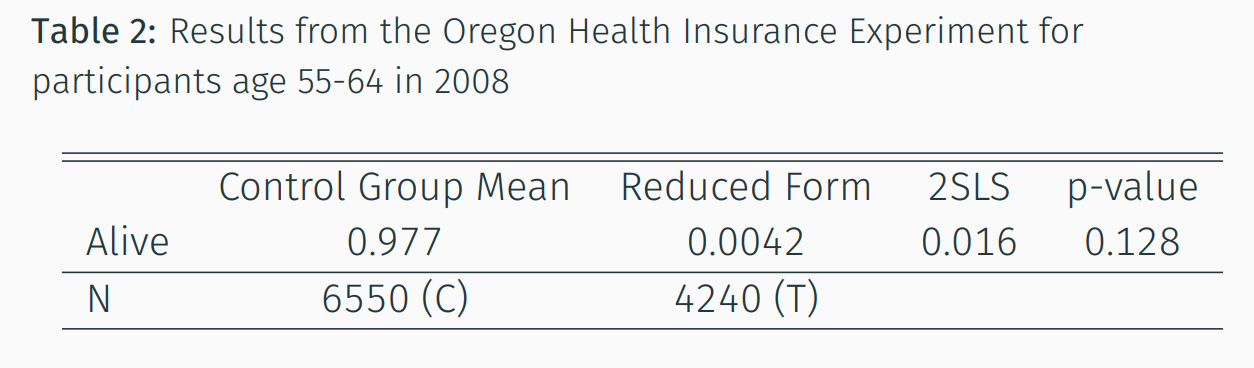
Mortality
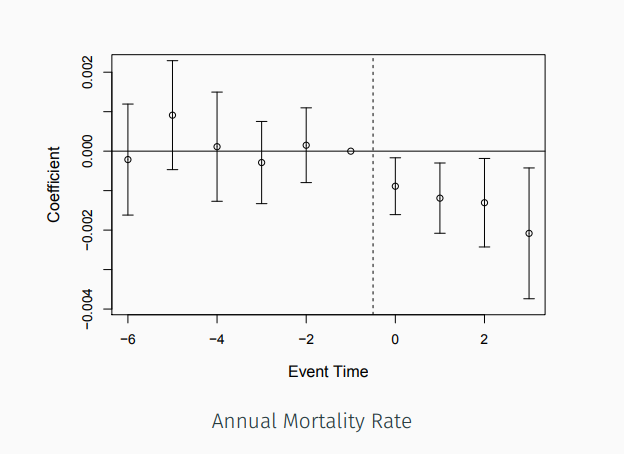
Probability of mortality for all who were alive at the beginning of the year
Mortality
Reduction of 0.09 percentage points first year, increasing to about 0.2 percentage points by year 4
Takeaway
Reduction in mortality rate for near elderly adults who benefited the most from the Medicaid expansions.
Is this obvious????
-Increases coverage
-Increases use of life saving care
-Increases use of valuable prescription drugs


Challenges
Previous studies did not have big enough sample sizes or did not have information on eligibility, which made people less likely to take them seriously.
Just bringing new data to an old question can really benefit our policy knowledge!
Other Results
- Younger ages: Much smaller effect that is not statistically significant
- By cause of death: cardiovascular disease and diabetes are the biggest drivers
- No effect on "external" causes like opioid overdoses, suicides, and murders--seems to be driven by disease related deaths.
Brainstorm
- What other outcomes might the Medicaid expansions affected?
- What businesses might have been affected? How do you think they would respond?