NEIGHBORHOOD ENVIRONMENT AND HYPERTENSIVE DISORDERS OF PREGNANCY
A Dissertation Defense by
Hui Hu
June 17, 2016
Supervisory Committee:
Linda B. Cottler, PhD, MPH, FACE, Chair
Xiaohui Xu, PhD, MD, MA, Former Chair
Cindy A. Prins, PhD, MPH, CIC, CPH, Member
Barron H. Henderson, PhD, Member
Xiaomin Lu, PhD, Member

Outline
Background
Ozone and HDP in Florida: Identifying Critical Windows of Exposure
Neighborhood Socioeconomic Status and HDP in Florida
Racial Disparities in HDP Mediated by Neighborhood Environmental Factors
Conclusions
Background
Public Health Significance of HDP
Theoretical Framework
Air Pollution and HDP
Neighborhood SES and HDP
Racial Disparities in HDP
Knowledge Gap
Research Objectives
Hypertensive Disorders of Pregnancy (HDP)

A common pregnancy complication (up to 10%)
Classified into four categories:
- Chronic hypertension
- Gestational hypertension
- Preeclampsia-eclampsia
- Preeclampsia superimposed on chronic hypertension
Linked to adverse health outcomes in both mothers and infants
Theoretical Framework
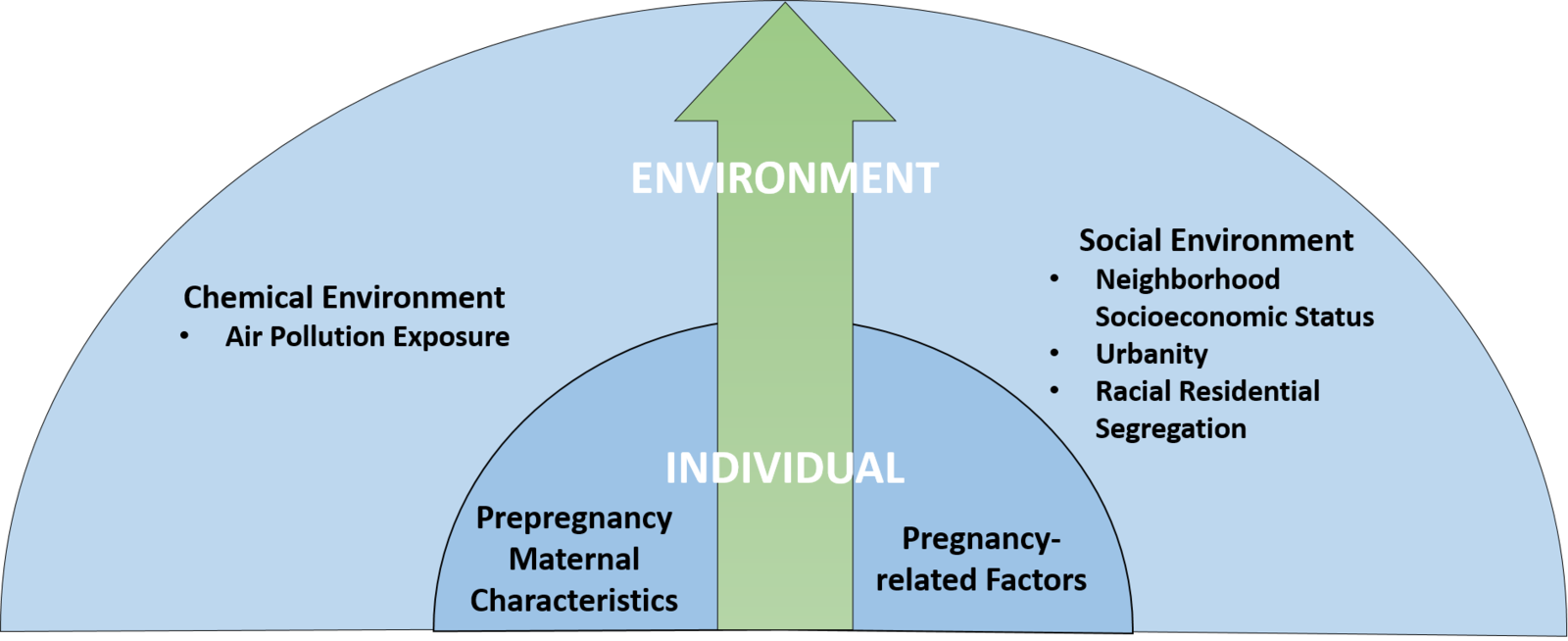
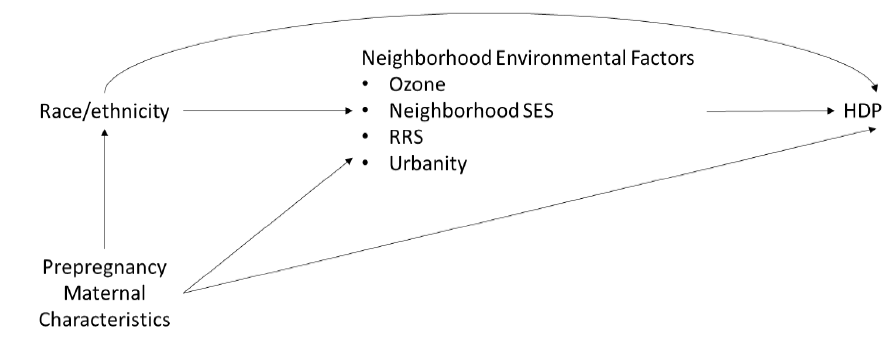
A Socio-Ecological Model (SEM) of Factors Influencing HDP
Air Pollution and HDP
Air pollution and adverse birth outcomes
Air pollution and hypertension in the general population
Potential biological mechanisms:
- Increased oxidative stress
- Lipid peroxidation
- Inflammation
- Endothelial dysfunction
- Autonomic imbalance
- Altered blood rheology
Existing literature:
- Inconsistent results
- Sparsely located stationary air monitors
- Critical window of exposure is unknown
Chemical Environment
Neighborhood SES and HDP
Neighborhood SES and adverse birth outcomes
Neighborhood SES and hypertension in the general population
Existing literature:
- Inconsistent results
Social differences
Different SES categories examined
- Neighborhood SES is multifaceted
A variety of indices used in previous studies
Hard to interpret the results and to guide interventions
Social Environment
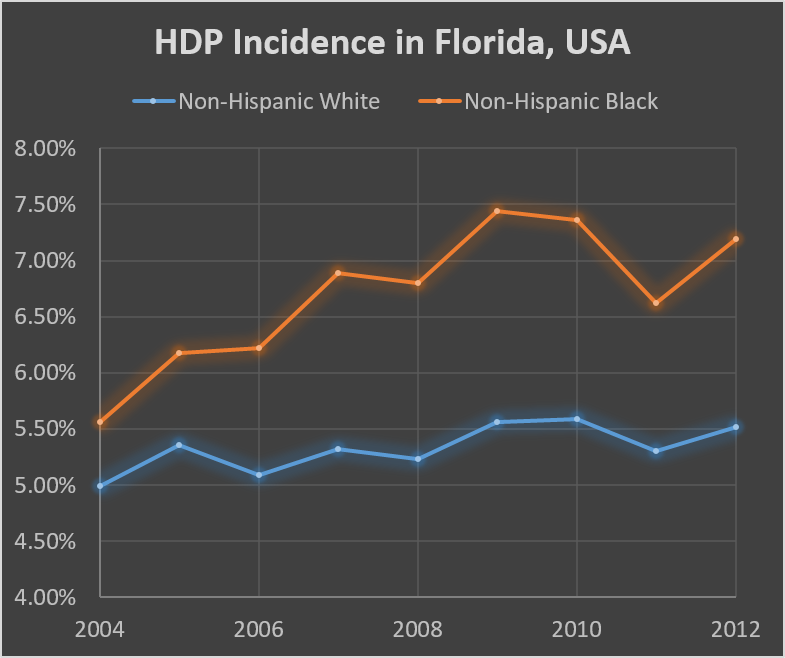
Racial Disparities in HDP
Increasingly large racial disparities in HDP
Racial residential segregation
- The fundamental cause of racial disparities
- Linked to adverse birth outcomes
Little is known about the factors contributing to racial disparities in HDP
Knowledge Gaps
Very few studies and inconsistent results
Critical window of exposure to air pollution during pregnancy is unknown
Individual neighborhood SES characteristic predictive of HDP is unknown
How neighborhood environment contributes to racial disparities in HDP is unknown
Ozone and HDP in Florida: Identifying Critical Windows of Exposure
Introduction
O3 is the air pollutant of the greatest concern to the state of Florida
Recent meta-analyses suggest an overall positive association between ozone and HDP
Limitations in existing literature:
- Sparsely located stationary air monitors
- Critical window of exposure to O3 is unknown
Research Objectives
- To investigate the association between O3 exposure during pregnancy and hypertensive disorders of pregnancy.
Hypothesis 1.1: Exposure to O3 during the first two trimesters of pregnancy is associated with hypertensive disorders of pregnancy.
Hypothesis 1.2: Early pregnancy is the most critical window of exposure.
Study Sample
Data source: Florida Vital Statistics Birth Record data
All women gave live births in Florida during 2005-2008 (n=917,788)
Residential addresses which could not be geocoded (n=108) or outside Florida (n=4,632) were excluded.
Conception date between January 1, 2005 and December 31, 2007 (n=691,011)
Exclude non-singleton deliveries (n=21,609), pre-pregnancy hypertension (n=10,590), birthweight <500g or >5,000g (n=621), or with a gestational age <26 weeks (n=2,662).
A total of 655,529 women were included.
Outcome Assessment
Diagnoses of prepregnancy hypertension, gestational hypertension or preeclampsia, and eclampsia were collected
The restricted definition of HDP was used in this study, which only includes:
- Gestational hypertension
the development of hypertension after 20 weeks of pregnancy - Preeclampsia
the new onset of hypertension and proteinuria after 20 weeks of pregnancy - Eclampsia
the onset of convulsions
Ozone Exposure Assessment
Data: The hierarchical Bayesian space-time statistical modeled (HBM) data from the National Environmental Public Health Tracking Network (2005-2008)
- Daily
- 12km×12km
Exposure windows:
- Predefined: trimester 1 only (1-13 weeks), trimester 2 only (14-26 weeks), and trimesters 1 and 2 (1-26 weeks)
- Weekly
Covariates
Age: <20, 20-24, 25-29, 30-34, 35-39, or ≥40 years old
Race/ethnicity: non-Hispanic White, non-Hispanic Black, Hispanic, or others
Education: <high school, high school or equivalent, or >high school
Marital status: married or not married
Pregnancy smoking status: yes or no
Pre-pregnancy BMI: underweight, normal, overweight, or obese
Season of conception: warm (June-November) or cool (December-May)
Year of conception: 2005, 2006, or 2007
Statistical Analyses
Predefined windows of exposure:
- Trimester 1 only, trimester 2 only, and both trimesters 1 and 2
- Logistic regression models
- Both an unadjusted model and an adjusted model controlling for covariates
- ORs with 95% CIs for each 5 ppb increase in O3
Identification of critical window of exposure:
- Weekly
-
Constrained distributed lag models
The associations between HDP and each of the 26 weekly O3 exposures was examined controlling for other weekly O3 exposures.
Constrained the 26 weekly specific effect estimates to follow the shape of a natural cubic spline with a knot at lag 13
Results
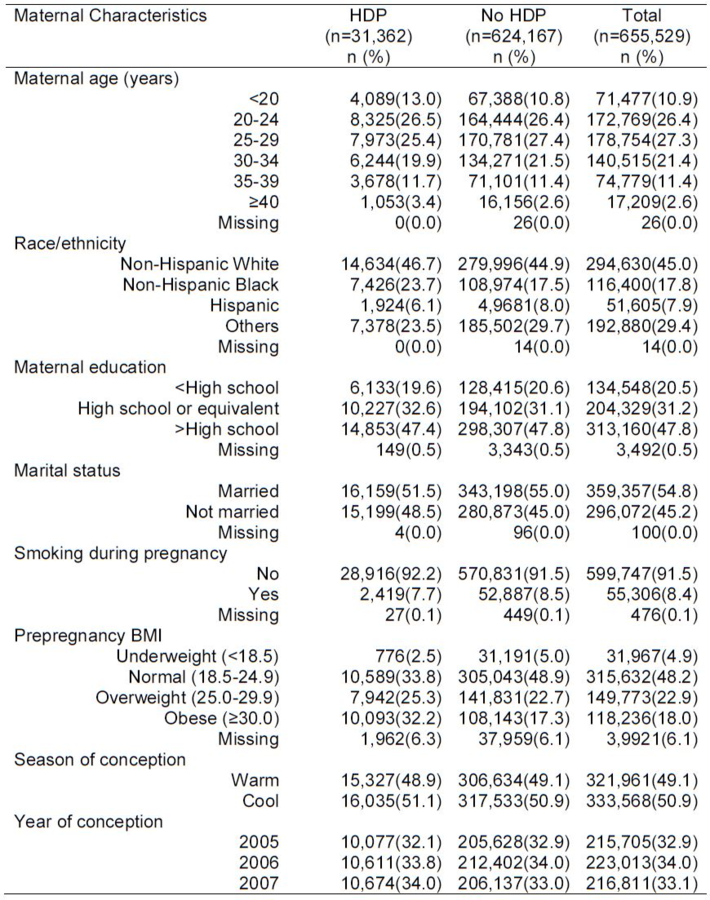
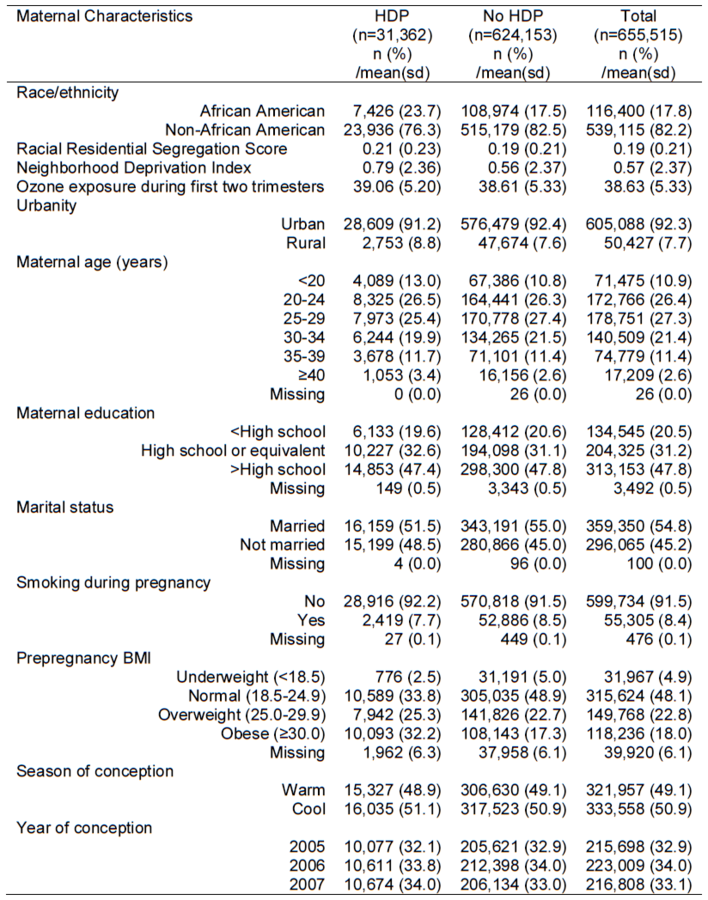
Compared with women without HDP, HDP cases were:
- less likely to be between 25-34 years old, married, or have smoked during pregnancy
- more likely to be non-Hispanic Black
- with higher pre-pregnancy BMI
31,362 (4.8%) women had HDP
Results
Women with HDP had a higher exposure to O3 compared with those without HDP during the three pre-defined exposure windows

Results

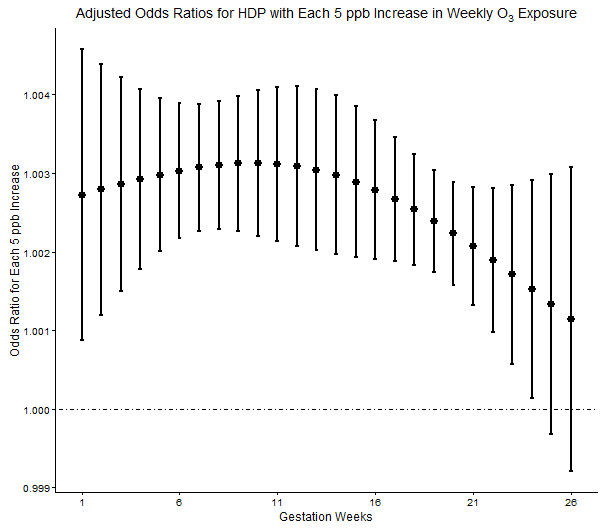
Positive associations between HDP and O3 exposure across the first 24 weeks of gestation, with higher odds of HDP observed in early pregnancy
Discussion
A consistent pattern of elevated odds of HDP with increased exposure to O3 during the first two trimesters.
Early pregnancy was the most critical window for O3 exposure during pregnancy.
Consistent with pooled estimates from meta-analyses
- First trimester exposure: OR=1.05, 95% CI: 1.02, 1.06 for each 5 ppb increase in O3
- No significant association for second trimester exposure
Discussion
Potential biological mechanism:
- Oxidative stress
- Lipid peroxidation
- Inflammation
- Endothelial dysfunction
- Autonomic imbalance
- Altered blood rheology
The elevated odds ratio observed in early pregnancy:
- Differences in blood pressure patterns during pregnancy
- Vasoconstriction
Discussion
Implications for health interventions:
- Almost impossible to avoid air pollution exposure during one's entire pregnancy period
- Identification of critical exposure window can guide future intervention
Strengths:
- Large sample size and high geocoded rate
- High temporal and spatial resolutions of the exposure data
- Assessed critical windows of exposure
Limitations:
- HDP measurements: no diagnosis dates or detailed blood pressure, potential under-diagnoses
- O3 measurements: no data on residential history, daily mobility and behavior patterns
Neighborhood Socioeconomic Status and HDP in Florida
Introduction
Socioeconomic status (SES) is an important determinant of health.
Low neighborhood SES has been linked to increased risks of hypertension in the general population and adverse birth outcomes.
Limitations in existing literature:
- Only a few studies examined neighborhood SES and HDP
- All used composite indices and individual neighborhood SES factor predictive of HDP is unknown
Research Objectives
-
To examine the association between neighborhood socioeconomic status and hypertensive disorders of pregnancy.
Hypothesis 2.1: Neighborhood socioeconomic status assessed by the Standardized Neighborhood Deprivation Index is associated with hypertensive disorders of pregnancy.
Hypothesis 2.2: Individual neighborhood socioeconomic characteristics such as income and poverty are predictive of hypertensive disorders of pregnancy.
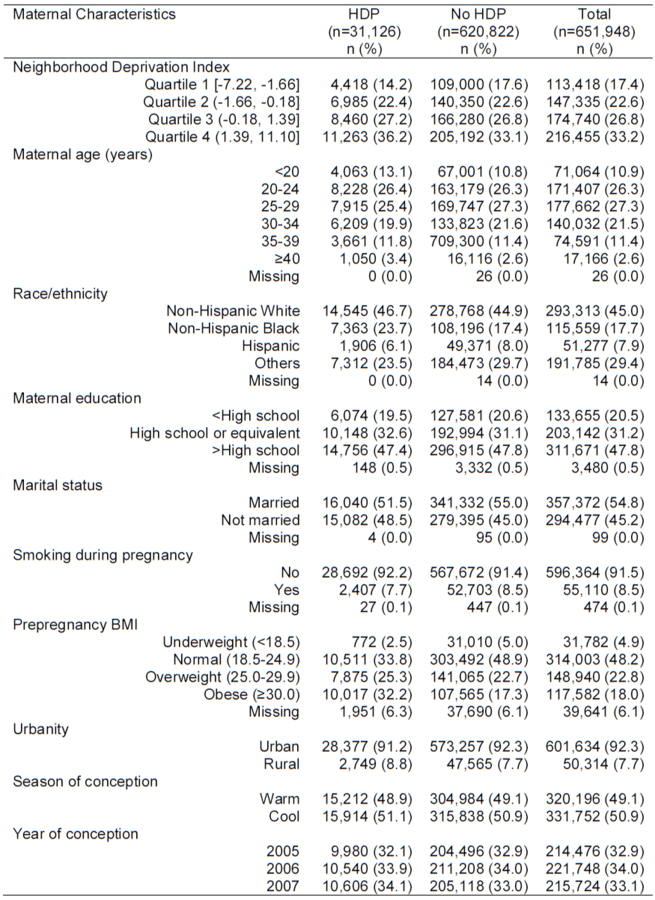
Study Sample
Data source: Florida Vital Statistics Birth Record data
All women gave live births in Florida during 2005-2008 (n=917,788)
Residential addresses which could not be geocoded (n=108) or outside Florida (n=4,632) were excluded.
Conception date between January 1, 2005 and December 31, 2007 (n=691,011)
Exclude non-singleton deliveries (n=21,609), pre-pregnancy hypertension (n=10,590), birthweight <500g or >5,000g (n=621), with a gestational age <26 weeks (n=2,662), or missing NDI (n=3,581).
A total of 651,948 women were included.
Outcome Assessment
Diagnoses of prepregnancy hypertension, gestational hypertension or preeclampsia, and eclampsia were collected
The restricted definition of HDP was used in this study, which only includes:
- Gestational hypertension
the development of hypertension after 20 weeks of pregnancy - Preeclampsia
the new onset of hypertension and proteinuria after 20 weeks of gestation - Eclampsia
the onset of convulsions
Neighborhood SES Assessment
Data: The 2006-2010 American Community Survey
- 17 census-tract level SES characteristics
-
Covering 7 different domains:
Poverty: % HHs in poverty, % HHs earning <$30,000/year, % HHs with no vehicle
Occupation: % males(females) in management or professional occupations
Housing: % rented housing, % vacant housing, % renter/owner costs>50% income, median household value
Employment: % unemployed, % males no longer in work force
Education: % <high school education
Racial composition: % non-Hispanic blacks
Residential stability: % in same residence in the last year, % residents ≥65 years old
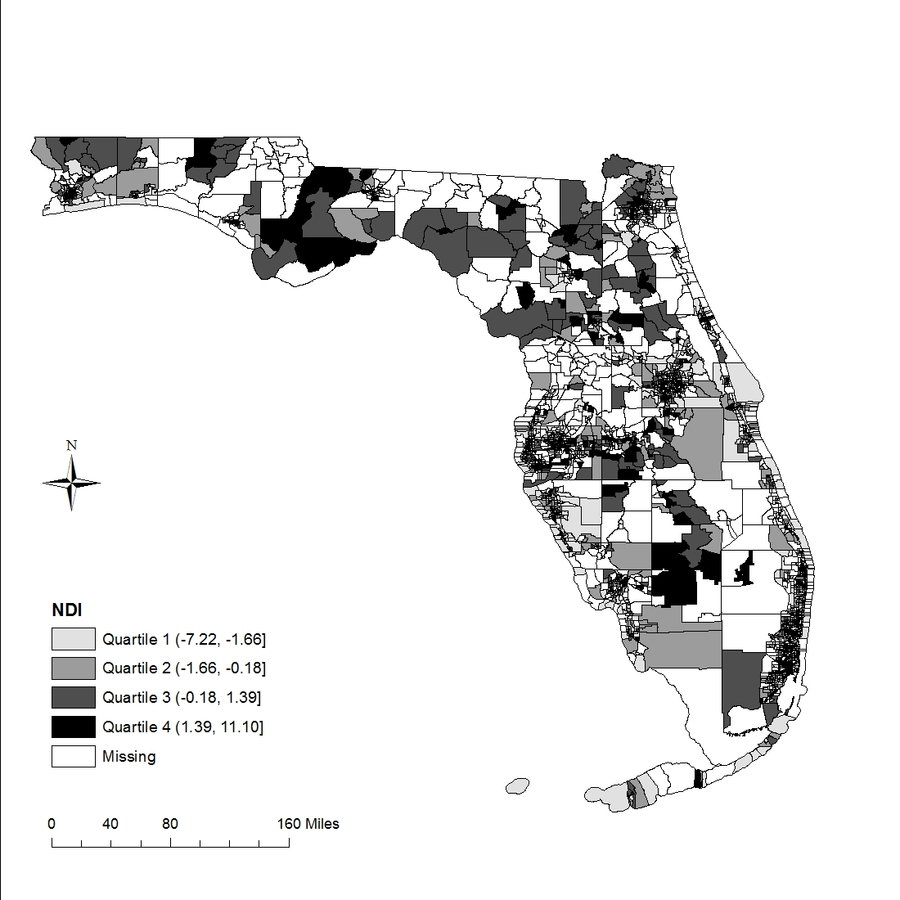
Neighborhood Deprivation Index (NDI):
- Created using the first factor loadings from PCA
- Categorized into quartiles in census-tract level
Covariates
Age: <20, 20-24, 25-29, 30-34, 35-39, or ≥40 years old
Race/ethnicity: non-Hispanic White, non-Hispanic Black, Hispanic, or others
Education: <high school, high school or equivalent, or >high school
Marital status: married or not married
Pregnancy smoking status: yes or no
Pre-pregnancy BMI: underweight, normal, overweight, or obese
Season of conception: warm (June-November) or cool (December-May)
Year of conception: 2005, 2006, or 2007
Urbanity: urban or rural
Statistical Analyses
NDI:
- Logistic regression models
- Both an unadjusted model and an adjusted model controlling for covariates
- ORs with 95% CIs
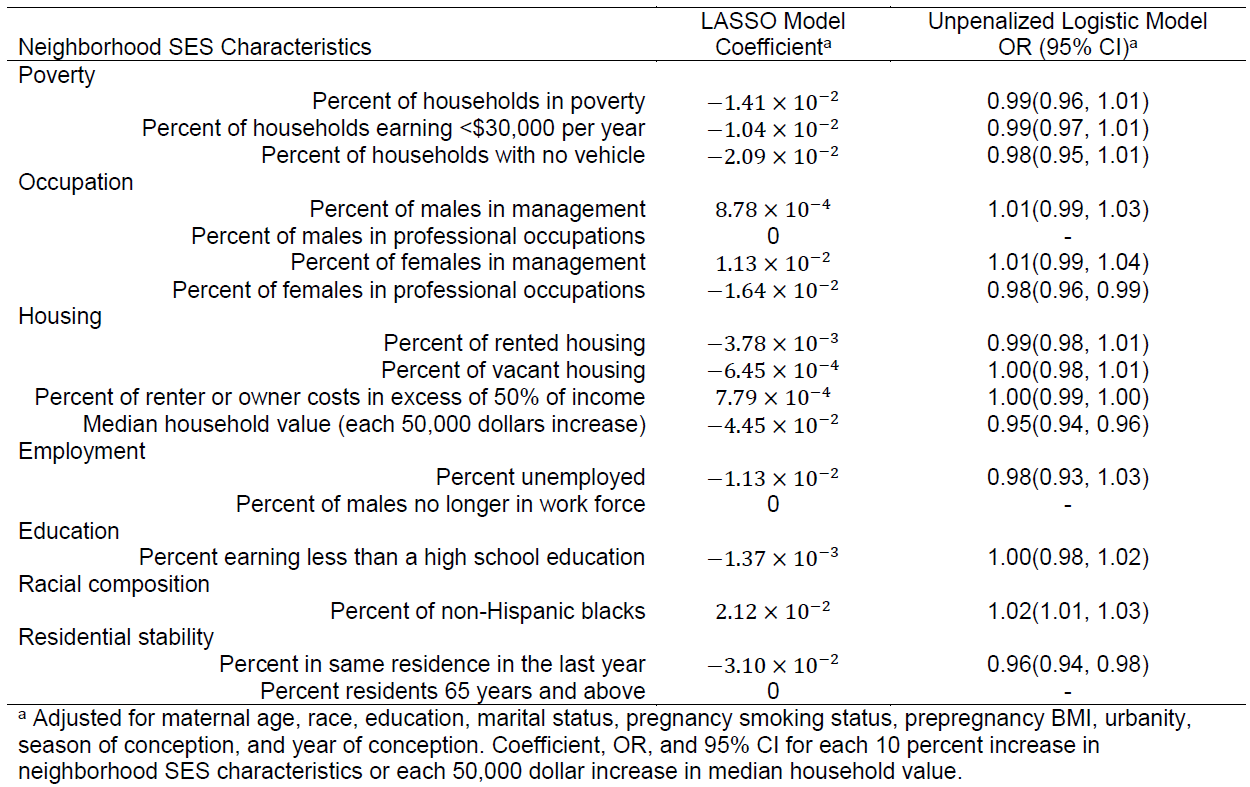
Determination of predictive neighborhood SES characteristics:
-
Regularized Logistic regression with l1-penalty (LASSO)
The parameter λ was tuned by a 10-fold cross-validation based on AUC - Variables with nonzero coefficients were refitted using the unpenalized Logistic regression model
Results
Results

Results
Discussion
Women living in neighborhoods with lower SES had higher odds of HDP.
The following neighborhood characteristics are predictive of HDP:
- Percentage of women in professional occupations
- Percentage of non-Hispanic blacks
- Median household value
-
Residential stability
Consistent with previous studies:
- Clausen et al. 2006 found that women living in low-income areas had higher rates of preeclampsia than women living in high-income areas.
- Vinikoor-Imler et al. (2012) reported a positive association between neighborhood deprivation and HDP in the US.
Discussion
Implications for health interventions:
- Provides insights into the important characteristics of SES that may inform targeted intervention.
- Identifications of vulnerable population subgroups such as pregnant women living in a low SES neighborhood with a residential instability.
Strengths:
- Large sample size and minimal selection bias
- Assessed neighborhood SES using both a composite index and individual characteristics.
Limitations:
- HDP measurements: no diagnosis dates or detailed blood pressure, potential under-diagnoses.
- Neighborhood SES measurements: low temporal resolution in the exposure data.
- Other potential confounders such as diet.
Racial Disparities in HDP Mediated by Neighborhood Environmental Factors
Introduction
The burden of HDP falls disproportionately on African Americans.
There is an increasing trend of racial disparities in HDP.
Neighborhood environmental factors such as racial residential segregation, urbanity, neighborhood SES, and O3 exposure are potential mediators for racial disparities in HDP.
Few studies has directly addressed how neighborhood environmental factors contribute to the racial disparities in HDP.
Research Objectives
-
To examine the racial disparities in hypertensive disorders of pregnancy and how neighborhood environmental factors mediate the pathways.
Hypothesis 3.1: African American women have higher risks of hypertensive disorders of pregnancy compared with non-African Americans.
Hypothesis 3.2: The association between race and hypertensive disorders of pregnancy is mediated by neighborhood environmental factors including O3 exposure during pregnancy, neighborhood socioeconomic status, urbanity, and racial residential segregation.
Study Sample
Data source: Florida Vital Statistics Birth Record data
All women gave live births in Florida during 2005-2008 (n=917,788)
Residential addresses which could not be geocoded (n=108) or outside Florida (n=4,632) were excluded.
Conception date between January 1, 2005 and December 31, 2007 (n=691,011)
Exclude non-singleton deliveries (n=21,609), pre-pregnancy hypertension (n=10,590), birthweight <500g or >5,000g (n=621), with a gestational age <26 weeks (n=2,662), or missing race/ethnicity (n=14).
A total of 655,515 women were included.
Outcome Assessment
Diagnoses of prepregnancy hypertension, gestational hypertension or preeclampsia, and eclampsia were collected
The restricted definition of HDP was used in this study, which only includes:
- Gestational hypertension
the development of hypertension after 20 weeks of pregnancy - Preeclampsia
the new onset of hypertension and proteinuria after 20 weeks of gestation - Eclampsia
the onset of convulsions
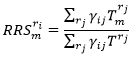
Racial Residential Segregation Assessment
The spatial measure of neighborhood level racial isolation developed by Anthopolos et al. 2011.
-
Census block-group level population count data by race from the 2006-2010 American Community Survey.
-
- It can be interpreted as the average percentage of group m in the local environment of r i as defined by the adjacency matrix.
- Bordering block groups located outside the State of Florida were also included to correct for the edge effects.
Assessments of Other Mediators and Covariates
Ozone: exposure during the first two trimesters using the HBM data
NDI: the first factor loadings from the PCA on 17 variables
Urbanity: 2010 Census
Age: <20, 20-24, 25-29, 30-34, 35-39, or ≥40 years old
Race/ethnicity: non-Hispanic White, non-Hispanic Black, Hispanic, or others
Education: <high school, high school or equivalent, or >high school
Marital status: married or not married
Pregnancy smoking status: yes or no
Pre-pregnancy BMI: underweight, normal, overweight, or obese
Season of conception: warm (June-November) or cool (December-May)
Year of conception: 2005, 2006, or 2007
Statistical Analyses
Determination of racial disparities in HDP:
- Logistic regression models
- Both an unadjusted model and an adjusted model controlling for covariates
- ORs with 95% CIs
Mediation analyses to determine how neighborhood environmental factors contribute to racial disparities in HDP:
- The Inverse Odds Ratio Weighting (IORW) developed by Nguyen et al. 2015
Mediation Analyses
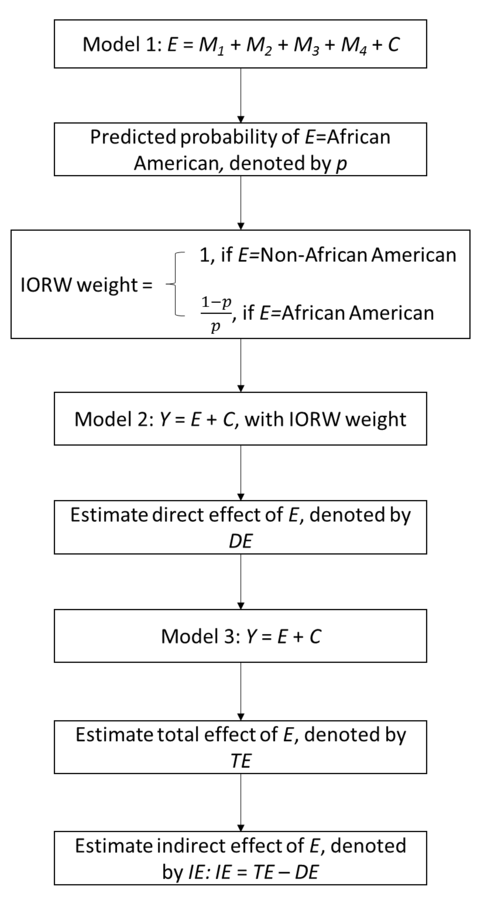
The IORW avoids the difficulties of specifying a model for the joint conditional density of multiple mediators by using weights to indicate the relationship between exposure and multiple mediators.
Standard errors for the estimated direct and indirect effects were derived by using 1,000 bootstrap replications.
Results
Discussion
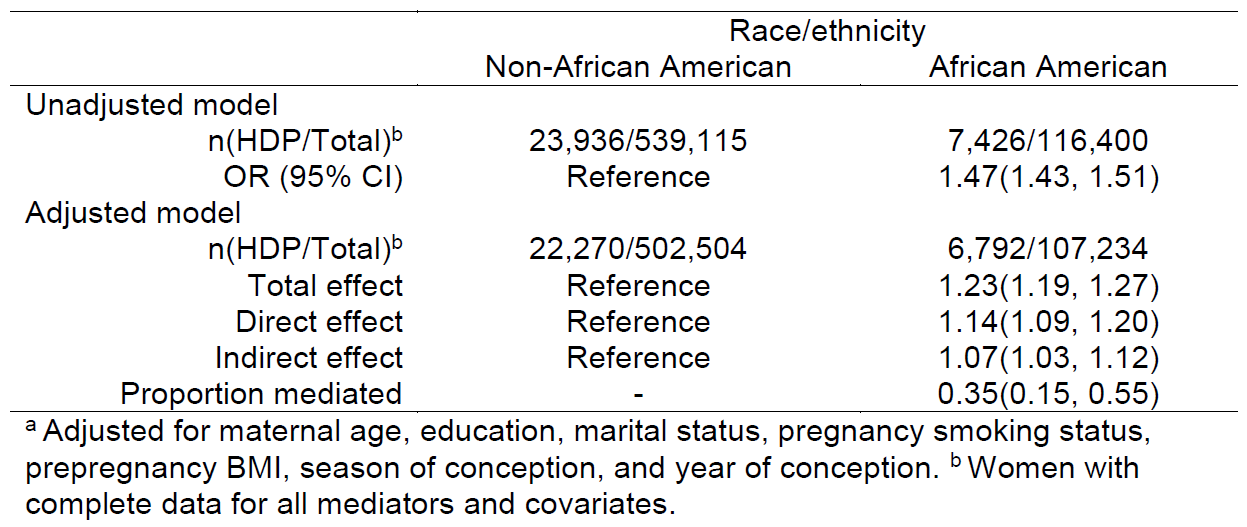
African American women had significantly higher odds to have HDP compared with non-African American women.
35% of racial disparities in HDP can be explained by the differential exposure to neighborhood environmental factors, including ozone exposure, urbanity, neighborhood SES, and racial residential segregation, between African American women and non-African American women.
Discussion
Consistent with existing literature:
-
Racial residential segregation has been regarded as the fundamental cause of racial disparities in health.
-
Urbanity, ozone exposure, and neighborhood SES have been linked to HDP.
- Studies suggested that the average residential context of African American communities is worse than the worst residential context for Whites.
Discussion
Implications for health interventions:
- Our findings suggest that the improvement on neighborhood environmental factors can greatly reduce the racial disparities in HDP.
-
More efforts should be given on neighborhood-level interventions such as:
The smart growth by The American Planning Association
The community revitalization initiatives
“Environmental justice” interventions
Strengths:
- Large sample size and minimal selection bias
- Assessed how neighborhood environment may contribute to racial disparities in HDP
Limitations:
- HDP measurements
- Exposure assessments
- Other potential confounders
Conclusions
-
Determination of Association between O3 Exposure during the Three Pre-defined Exposure Windows of Pregnancy and HDP
-
Identification of Critical Windows of O3 Exposure during Pregnancy for HDP
-
Determination of Association between Neighborhood SES and HDP
-
Identification of Individual Neighborhood Socioeconomic Characteristics Predictive of HDP
-
Identification of Racial Disparities in HDP between African Americans and Non-African Americans
-
Determination of the Proportions of Racial Disparities in HDP Contributed by Neighborhood Environmental Factors Including O3 Exposure, Neighborhood SES, urbanity, and Racial Residential Segregation
Limitations and Future Directions
Limitations:
- Measurement errors in the outcome, exposure, and covariates.
- Trade-off between measurement errors and selection biases.
- Lack of individual-level interventions to reduce environmental risk factors of HDP.
Future directions:
- Innovative data sources such as remote sensing and satellite imaging
- mHealth
Acknowledgements
Supervisory Committee:
- Linda B. Cottler, PhD, MPH, FACE, Chair, Department of Epidemiology, UF
- Cindy A. Prins, PhD, MPH, CIC, CPH, Member, Department of Epidemiology, UF
- Barron H. Henderson, PhD, Member, Department of Environmental Engineering Sciences, UF
- Xiaomin Lu, PhD, Member, Department of Biostatistics, UF
Former Research Mentor: Xiaohui Xu, PhD, MD, Department of Epidemiology & Biostatistics, TAMU
Academic Advisors:
- Volker Mai, PhD, MPH, Current Advisor, Department of Epidemiology, UF
- Maria R. Khan, PhD, MPH, Former Advisor, Department of Population Health, NYU
Florida Department of Health
All faculty, staff, and fellow students in the Department of Epidemiology