The Importance of Flexion MRI in Hirayama Disease with Special Reference to Laminodural Space Measurements
D.K. Bourah et. al., AJNR May 2018
Background
- First described 1959
- “juvenile muscular atrophy” of distal upper limb extremity
or “monomelic amyotrophy.”
Background
- Insidious onset asymmetric wasting distal upper ext
- sparing brachioradialis
- C8-T1
- 2nd-3rd decades (15-25 years old)
- M > F
- RUE > LUE
Materials and Methods
- January 2014 to July 2017, Northeast India
- Young adults weakness/wasting hand/forearm
- motor axonopathy on nerve-conduction studies
Included subjects
- Other etiologies for weakness
- AS of C-spine
- Prior trauma or fixation
- Inability to adequately flex neck
Excluded subjects
45 subjects
Materials and Methods
- 1.5T Magnetom Avanto (Siemens)
- Imaged c-spine in neutral and flexed position
- Flexion imaging with body coil
- 30-40°
- Post-gad sag and axial in flexed position
MR protocol
Materials and Methods
- Cord flattening, T2 signal, atrophy
- Max forward shift of posterior dura (laminodural space)
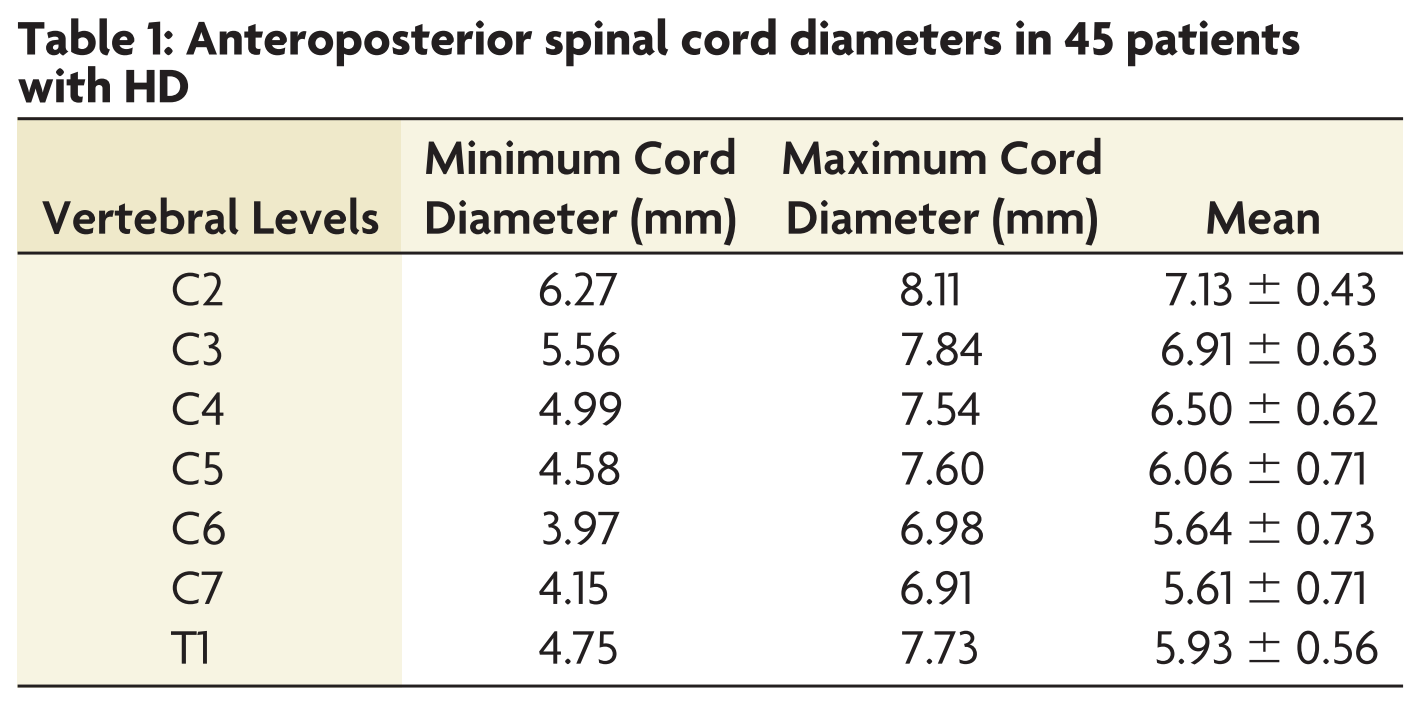
- AP + TV diameter of cord in neutral and flexed
- AP diameter of canal in neutral and flexed
Image analysis
Results
- 44 male, 1 female
- 14 - 42 years at presentation, mean 23 years
- 89% unilateral, 11% bilateral
- 100% hand, 60% forearm, 4% arm muscles
Subjects
Results
- localized lower cervical cord atrophy: 60%
- < 2 vertebral heights in 42%, 2-3 in 11%, > 3 in 7%
- Max mean atrophy at C6-7
- asymmetric flattening in 69%
Imaging findings
Results
- T2 cord signal abnormality: 36%
- Anterior horns: 33%
- Unilateral: 24%
- Bilateral: 9%
- Anterior horns: 33%
Imaging findings
Results
Imaging findings
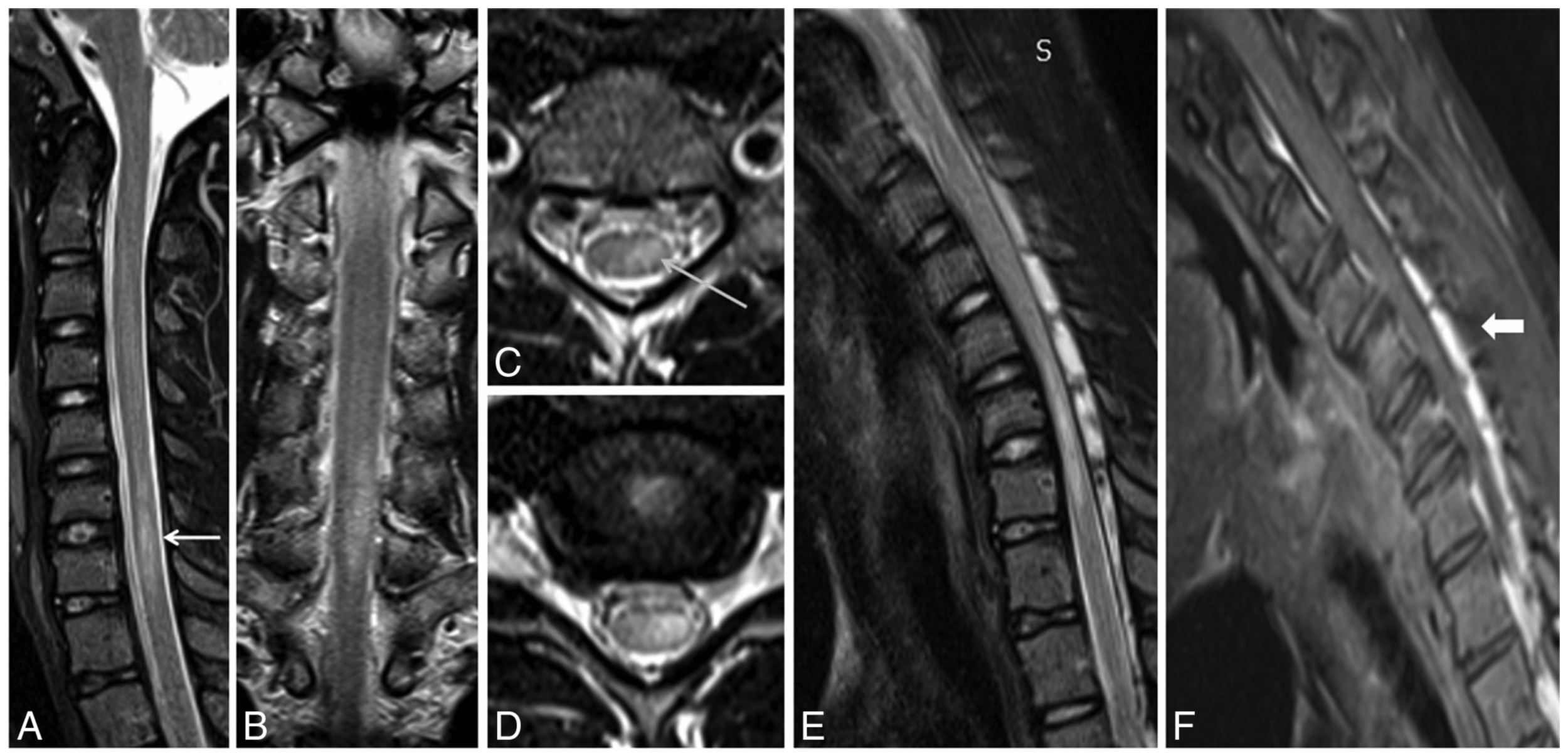
fig. 3
- Loss of dural attachment, forward shifting of posterior dura, enhancing prominent posterior epidural space: 100%
Results
Imaging findings
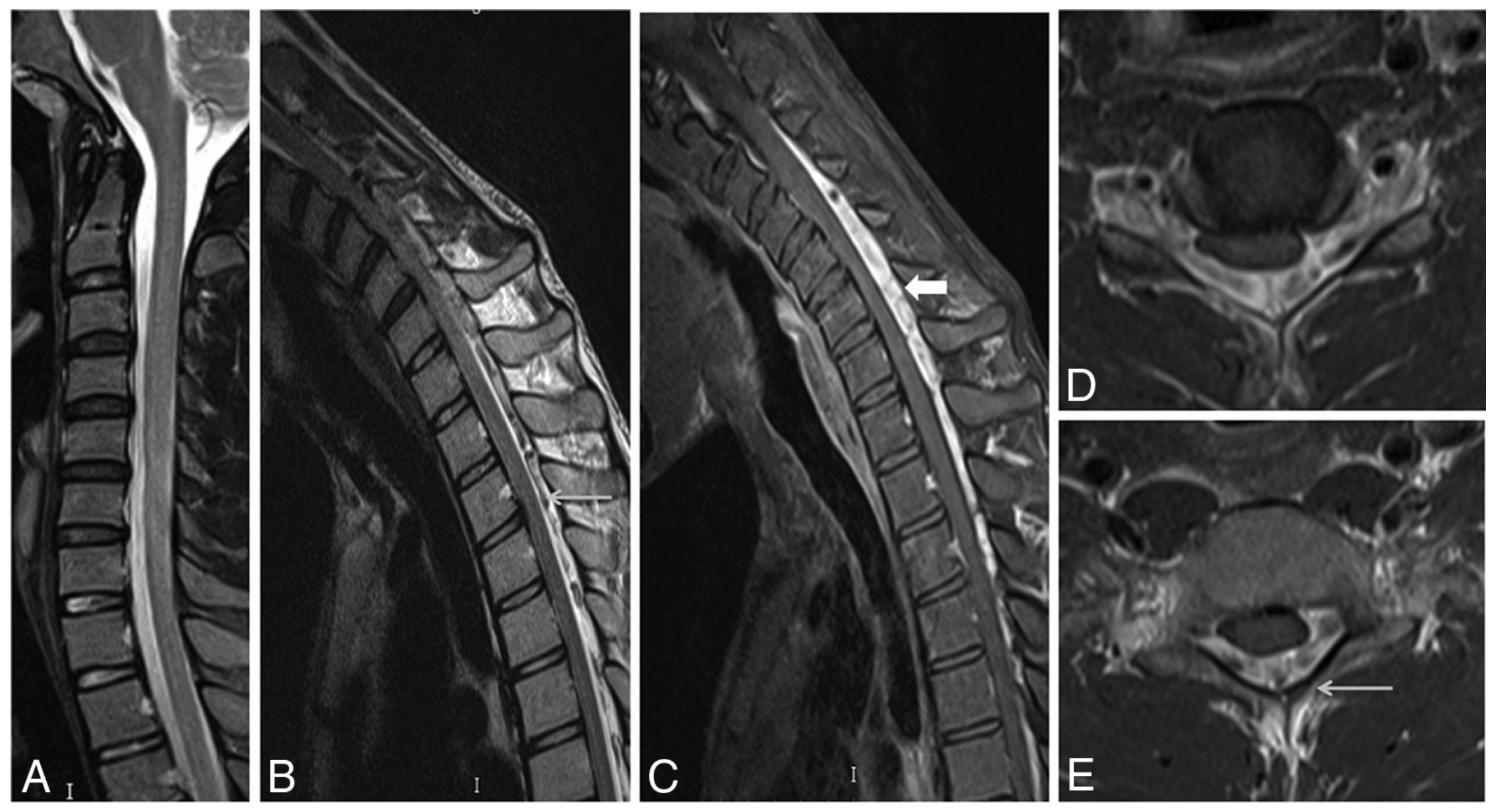
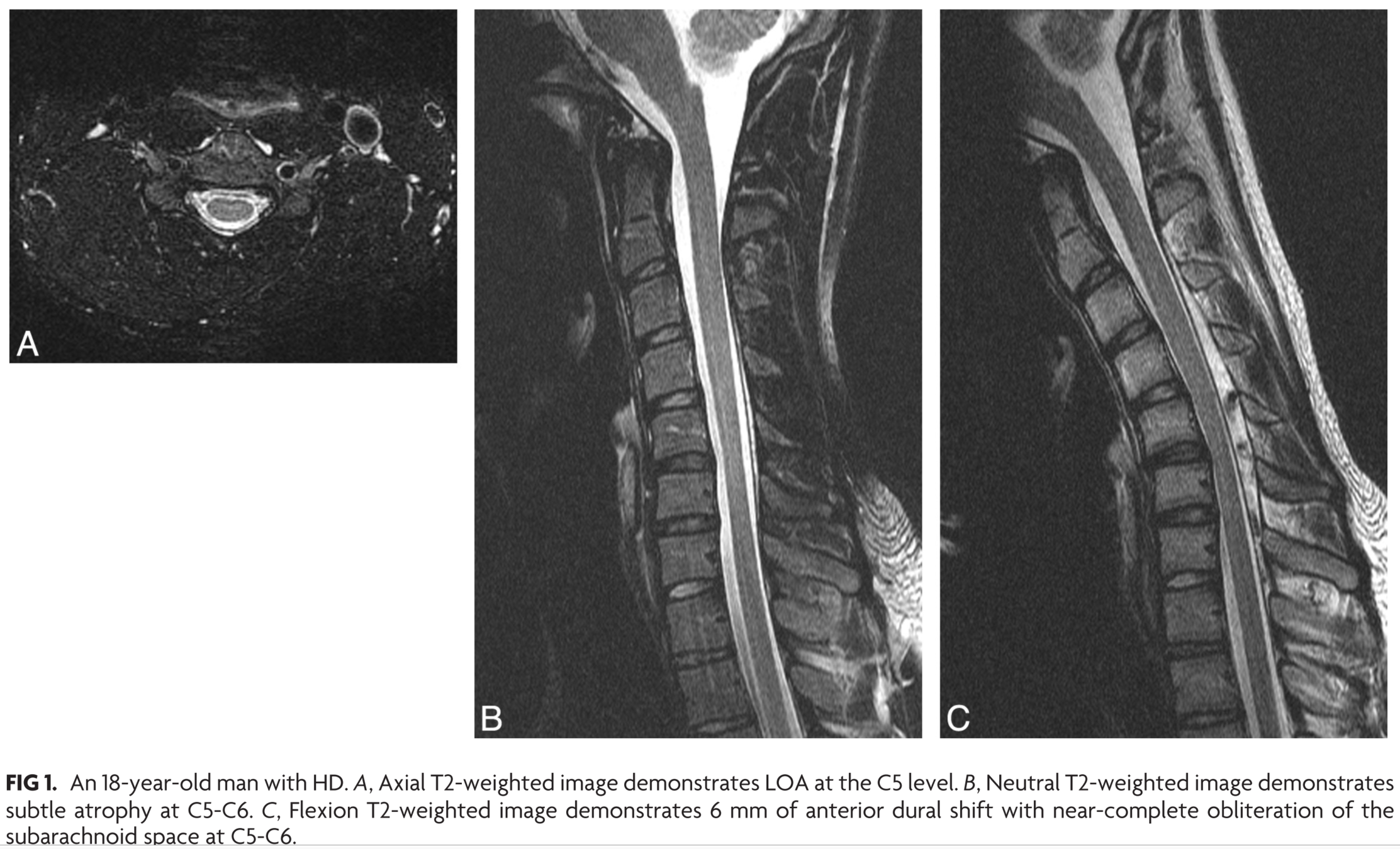
fig 1
Results
Imaging findings
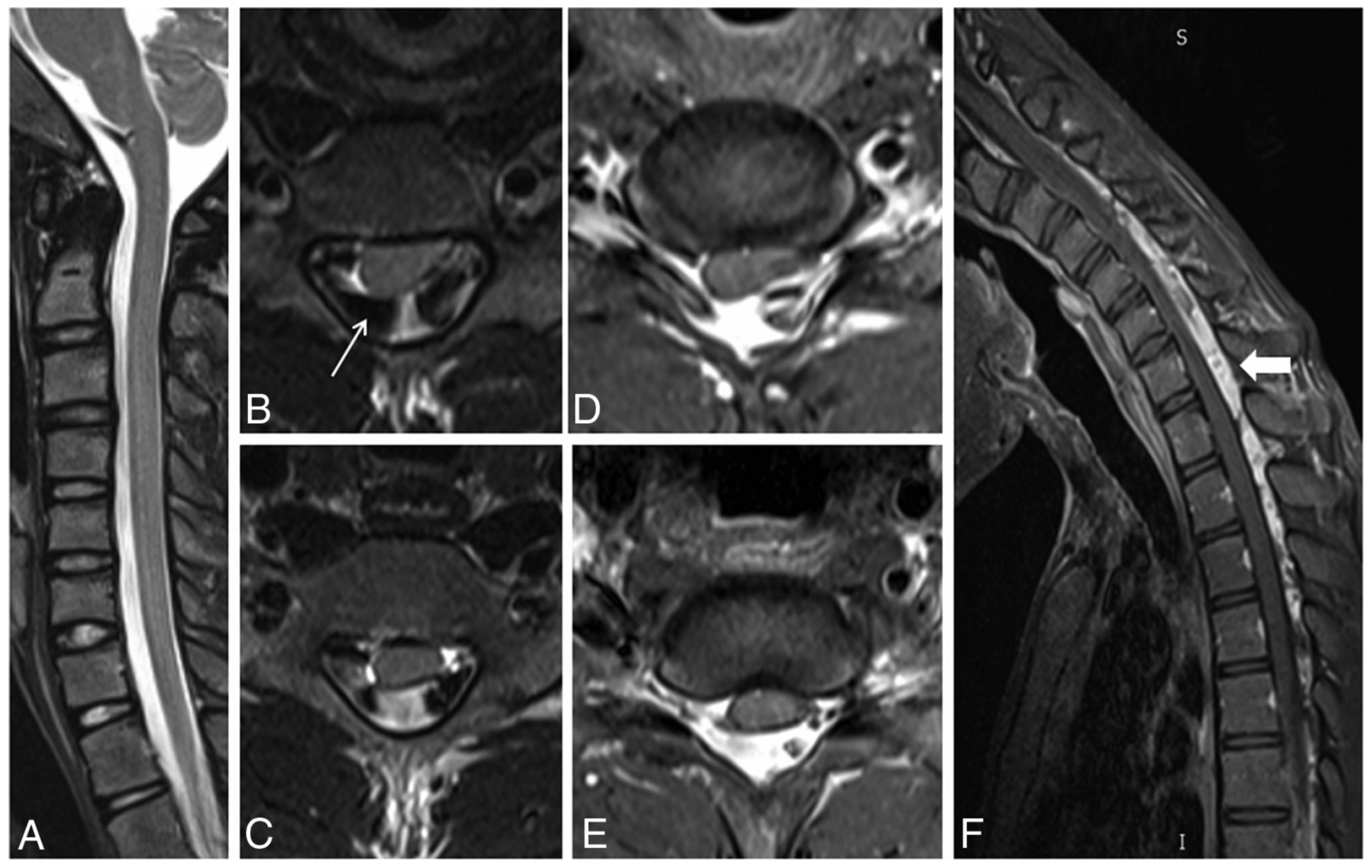
fig 2
Results
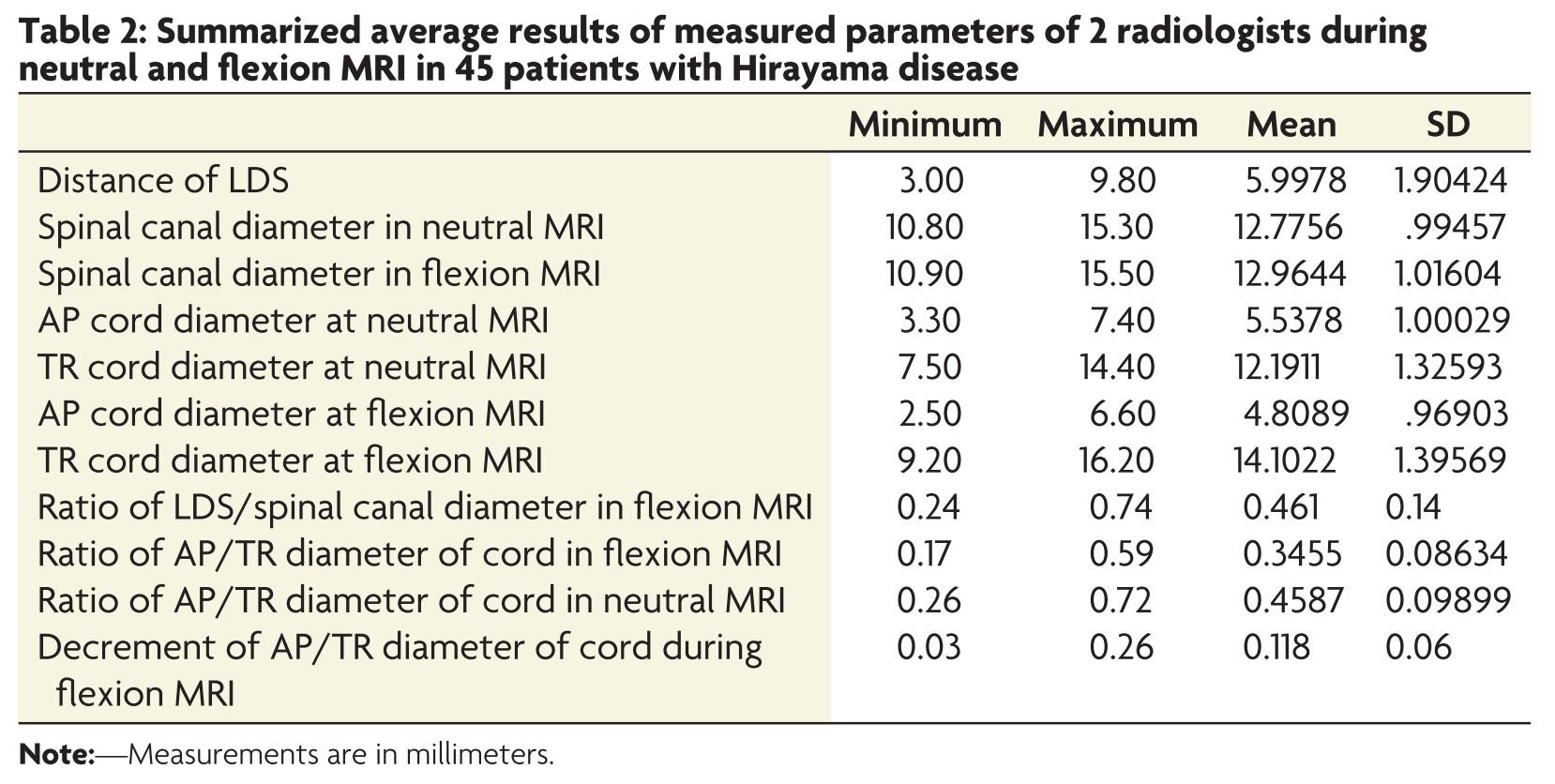
- Max LDS: 3 - 10mm, mean 6mm
- Posterior epidural flow voids: 47%
- Most had increased LDS at both C & T spine
- Diameter of bony canal not sig changed
- At max compression site, cord flattened in AP dimension by avg of 0.7mm
- Mean decrease in AP/TR ratio of 0.12
Imaging findings
Results
Imaging findings
Results
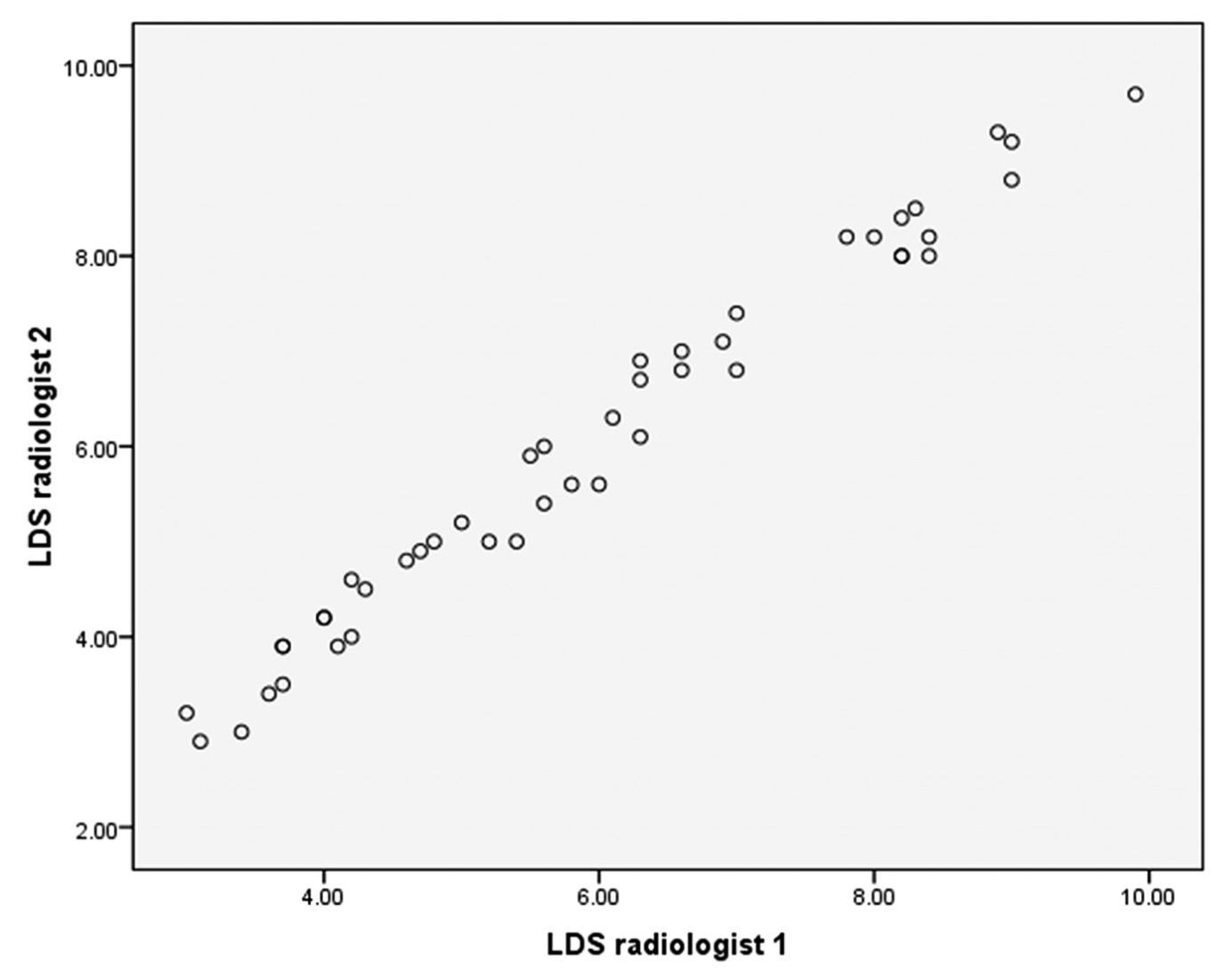
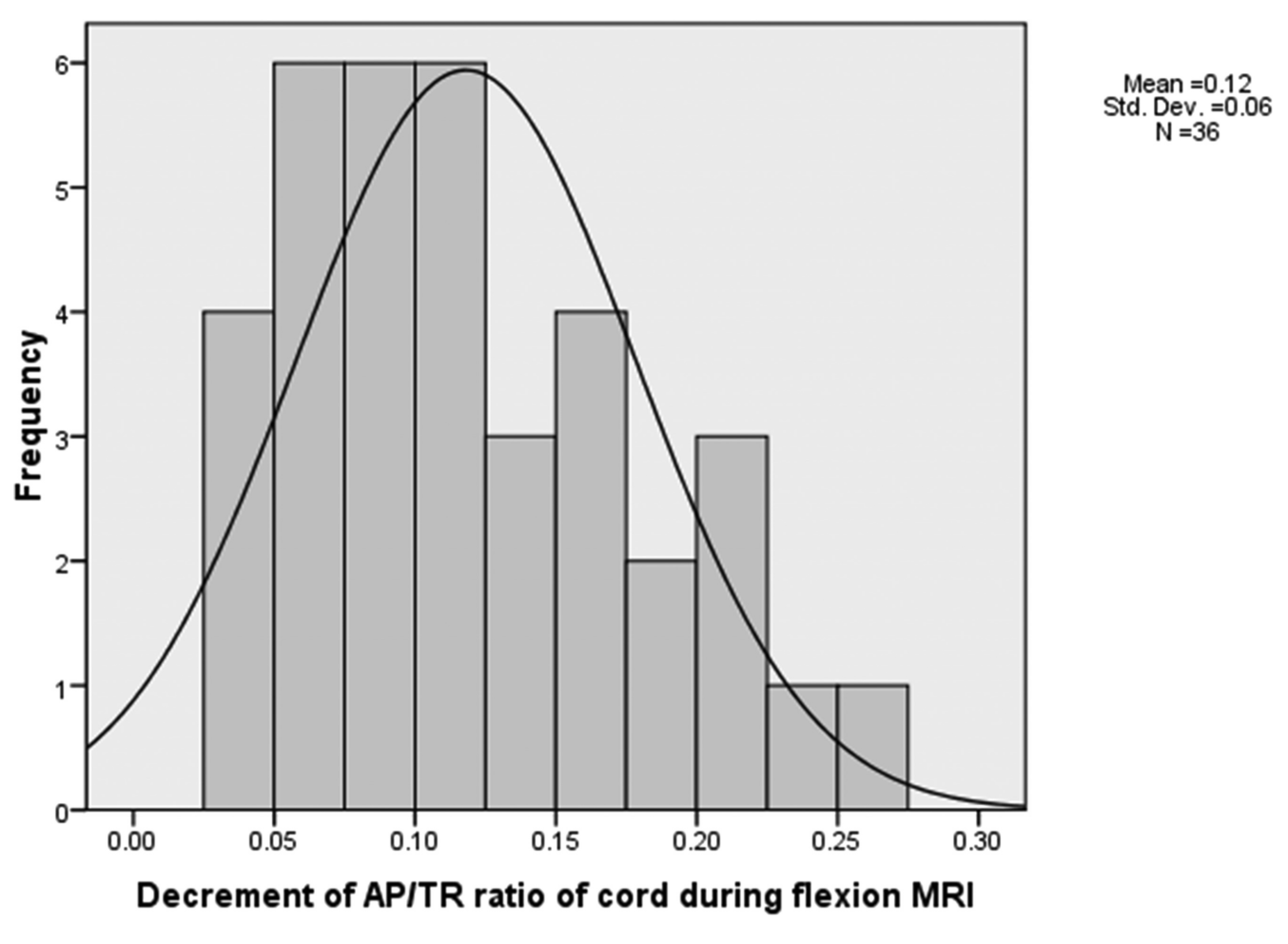
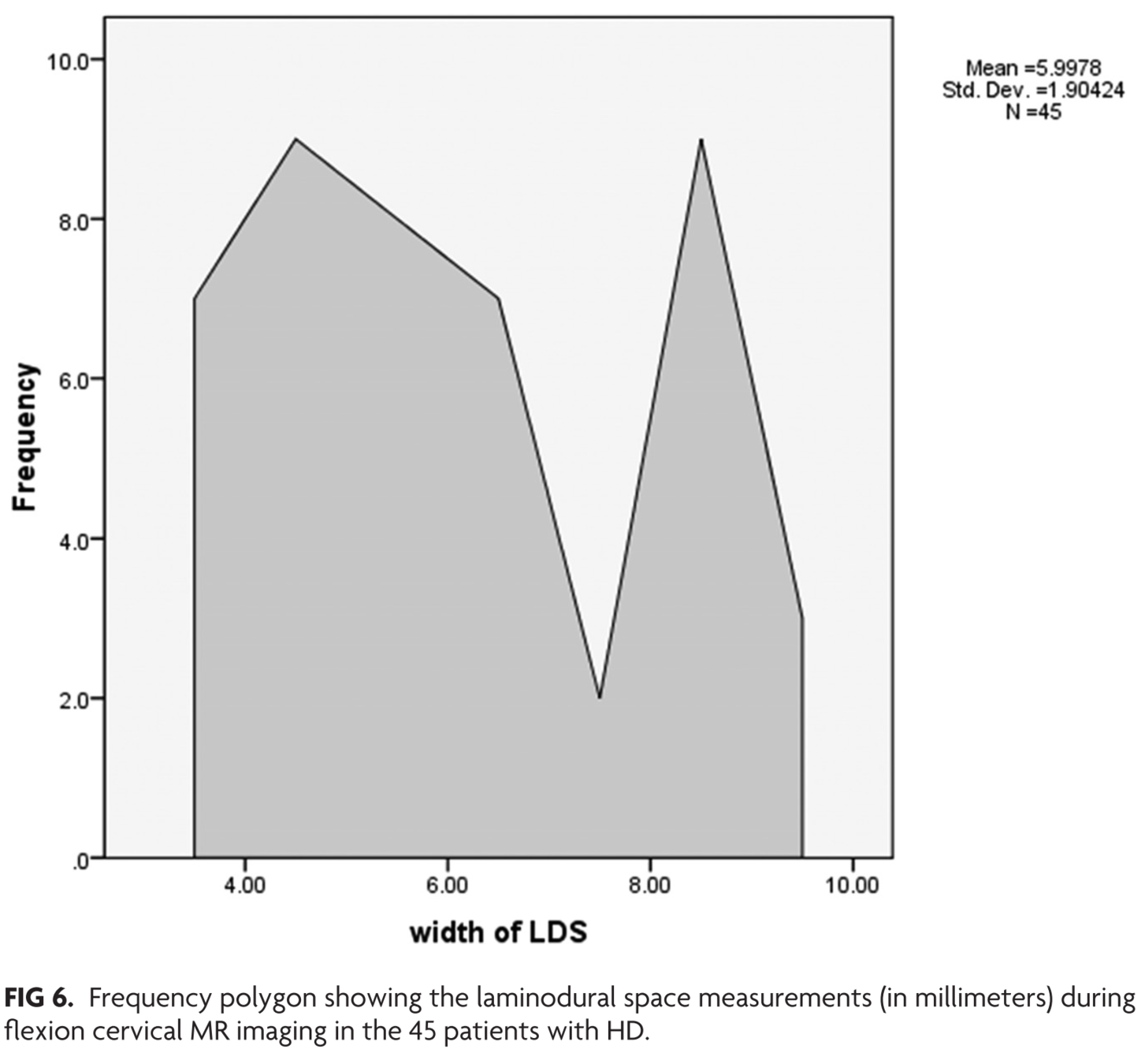
figs. 4, 5, 6
Discussion
Etiology...
- Repeated/sustained flexion leads to necrosis of anterior horn cells 2/2 chronic changes in ASA territory microvasculature
- Differential growth of vert column and cord -> abutment of cord -> ASA ischemia
- ? atopy/immunologic contribution
- Posterior epidural venous engorgement 2/2 impaired venous return from neg pressure in LDS
Discussion
Imaging important in diagnosis
- Neutral MRI may show atrophy, T2 signal, asymmetric flattening
- Flexion MRI shows classic findings
- Posterior dural detachment -> widened LDS
- Enh of engorged posterior epidural venous plexus
- Compression of cord
Discussion
What criteria to use?
- Lehman et al 2013: Sens similar for neutral and flexion (70% vs 71%), but neutral findings subtle
Discussion
What criteria to use
Lehman et al
Discussion
What criteria to use?
- Chen et al 2004: Loss of attachment 93% sensitive
- Lai et al 2011: LDS increase in 46% healthy subjects
- Proposed BOTH:
- increased LDS/canal diameter ratio
- decreased AP/TR cord diameter ratio
- But only 3 patients
- Proposed BOTH:
Discussion
What criteria to use?
- Current study applied these proposed criteria to 45 patients
- Mean LDS/canal ratio increase: 0.46
- Mean AP/TR cord diameter decrease: 0.12
Limitations
- No control group to determine cutoff for diagnosing HD
- Uniform neck flexion angle not achieved in all patients
Thoughts
- Ratios of LDS/canal & AP/TV seems like overkill
- Why not just loss of attachment and decreased AP cord diameter in flexion?
- Flexion images clearly helpful
- Comparison with asymptomatic controls would be helpful
Conclusions
- Important to recognize
- Self-limiting disease if early intervention
- (conservative or surgical)
- High index of suspicion in young person with insidious onset hand/forearm weakness
- Flexion imaging useful for diagnosis as findings can be missed on neutral images
- Self-limiting disease if early intervention