Abdomen : Case 2
History : A 50-year-old female with left flank pain.
Plain abdominal film was performed on admission.
What is the abnormality?
A. Small bowel dilatation
B. Retroperitoneal air
C. Left distal ureteric stone
D. Ascites

Answer : C. Left distal ureteric stone or left distal vesicoureteric junction stone

Phleobolith
Stone
Phleboliths "vein stones"
- Represent calcification within venous structures
- Particularly common in the pelvis where they may mimic ureteric calculi
Radiographic features :
- Focal calcifications, often with radiolucent centers (another helpful sign if present to distinguish them from ureteric calculi).
- This appearance is attributed to calcification peripherally within the vessel, and is frequently seen on abdominal radiographs.
Abdominal CT images
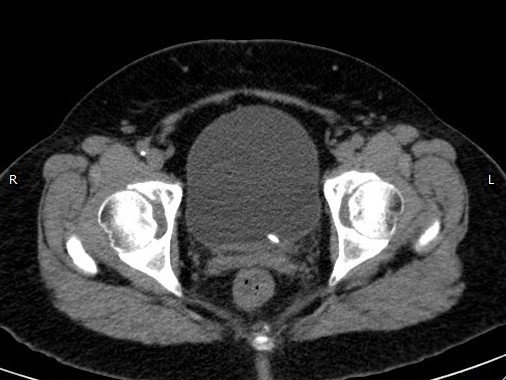
Abdominal CT images

Treatment :
-
Stone size is an important factor in treatment planning
- 90% of stones smaller than 4 mm and 50% of stones 4–7 mm will pass spontaneously
- Currently, the primary method for treatment of symptomatic urolithiasis is extracorporeal shock-wave lithotripsy (ESWL). Both the size and the location of a calculus within a ureter were important predictors of the success of ESWL
Evaluation of the Patient with Flank Pain and Possible Ureteral Calculus
Tamm EP, Silverman PM, Shuman WP. Radiology Aug 2003
- Flank pain due to urolithiasis : Common problem in patients presenting to emergency departments
- Imaging -> Primary role in the work-up
- Traditionally, evaluation consisted of conventional radiography followed by IVP
-
In the past several years, nonenhanced CT has evolved:
- Identify calculi and location
- Determine size
- Guide management
- However, questions remain regarding the optimal use of this technique because of concerns about radiation exposure and cost
Radiographic Examination : Plain KUB
- Often used as an inexpensive first step -> 90% of urinary calculi are radiopaque
- However, while large calculi can easily be seen, confounding factors such as overlying bowel gas or fecal material and osseous structures
- Gallstones may overlie the right renal collecting system, necessitating the use of oblique radiographs to distinguish these two entitie
IVP
- Traditional imaging modality of choice
-
After IV administration of contrast material. The classic signs:
- Delayed opacification of the collecting system
- Persistent delayed nephrogram that increases in intensity with time
-
Secondary signs :
- Formation of a column of contrast material proximal to a point of obstruction
- The rare instances of nonobstructing calculi may be difficult