











Ishanu Chattopadhyay PRO
ML | Data Science Biomedical Informatics | Social Science | Assistant Professor
Ishanu Chattopadhyay, PhD
ishanu_ch@uky.edu
CKD
PF
ZeBRA
ICD
Enable early diagnosis
Seamless background integration with EHR workflows
Primary care
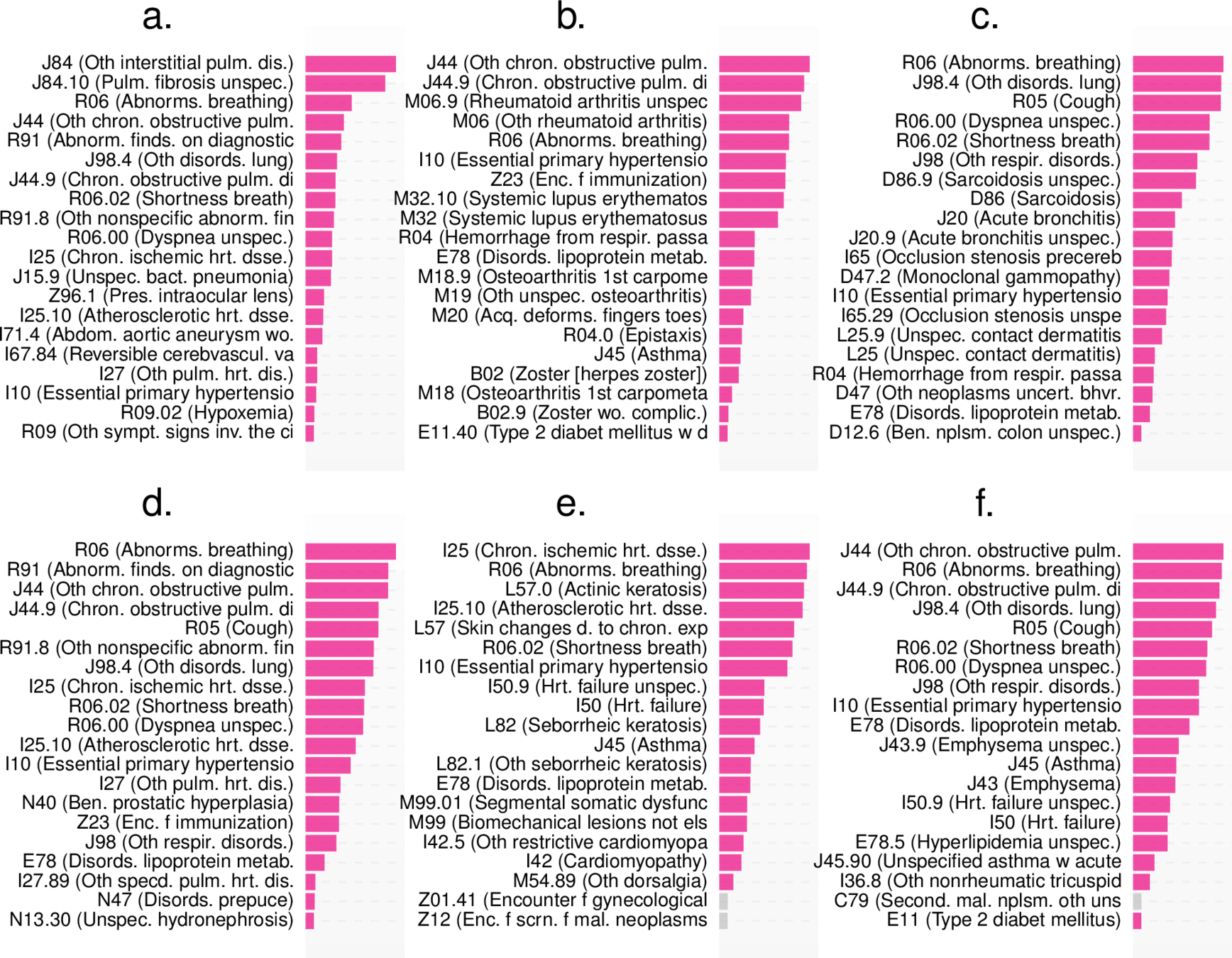
*Onishchenko, Dmytro, Robert J. Marlowe, Che G. Ngufor, Louis J. Faust, Andrew H. Limper, Gary M. Hunninghake, Fernando J. Martinez, and Ishanu Chattopadhyay. "Screening for idiopathic pulmonary fibrosis using comorbidity signatures in electronic health records." Nature Medicine 28, no. 10 (2022): 2107-2116.
Raising Flags before patient or their doctor notice symptoms
downstream care modulation
widely published, retrospectively validated*
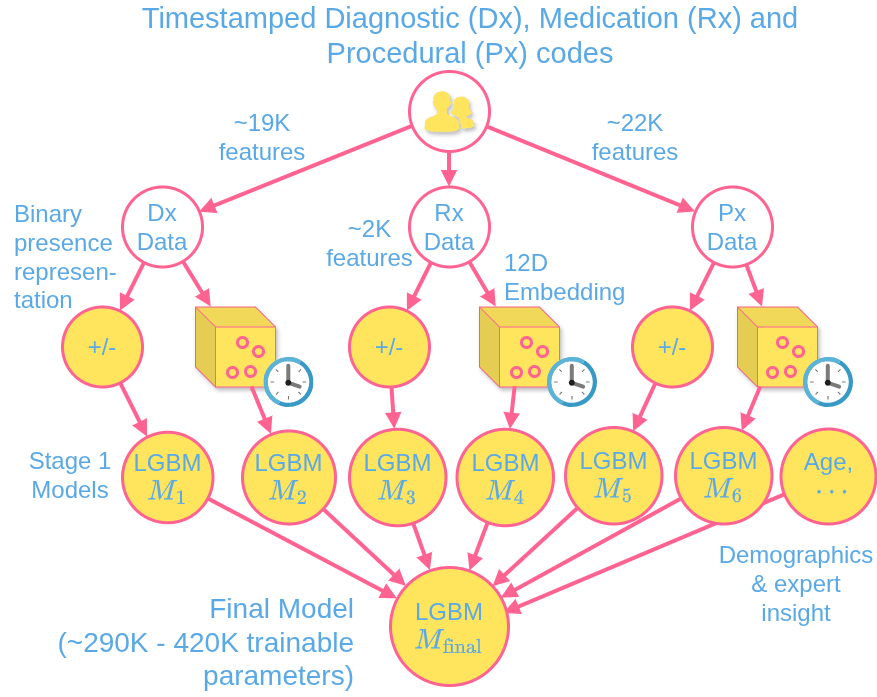
TimestampedDiagnostic procedural codes & prescriptions
MASH
Rx
Px
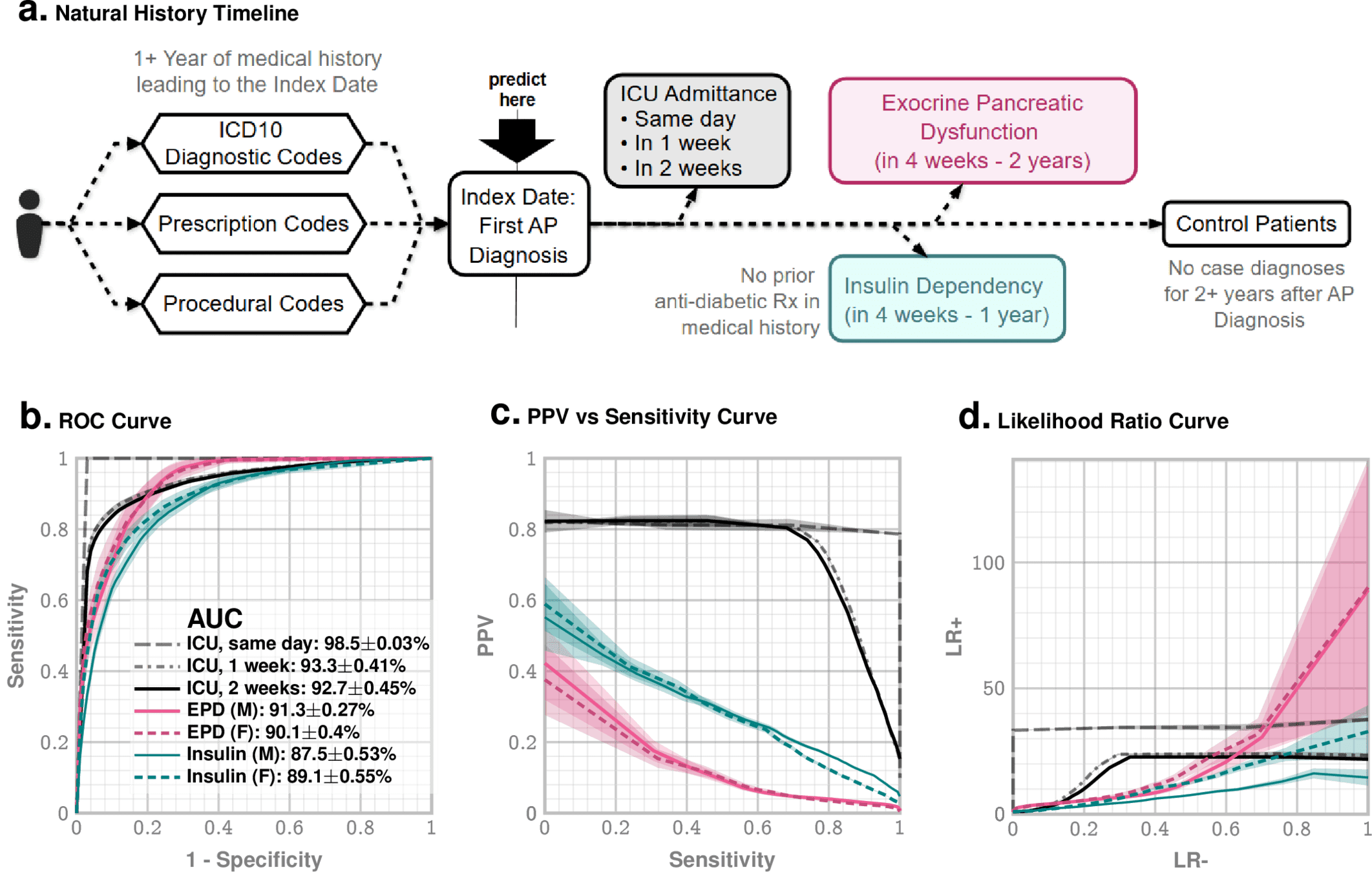
AI-driven Test-Free Prediction of ICU Admission, Insulin Dependence, and Exocrine Dysfunction after Acute Pancreatitis
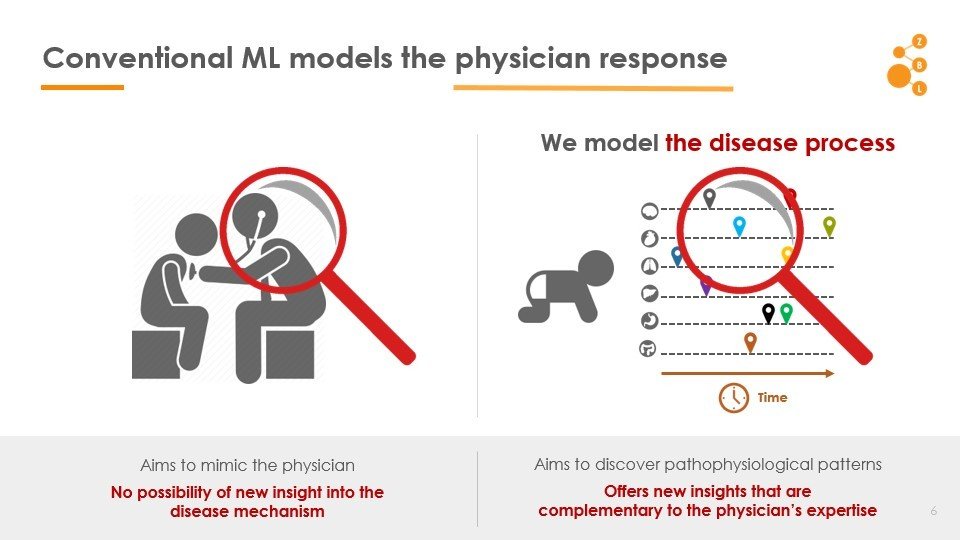
2. Conventional AI attempts to model the physician
Current State of Art
1. Use of AI in point-of-care diagnostic workflow is limited
ZeBRA
*Chattopadhyay, Ishanu, and Hod Lipson. "Abductive learning of quantized stochastic processes with probabilistic finite automata." Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences 371, no. 1984 (2013): 20110543.
Curated Disease-agnostic Features | Odds ratio dictionaries combined with multi-stage LGBMs | Specialized HMM based Longitudinal Tracking*
Standard AI
Non-specific Symptoms
Pulmonary Fibrosis
Rare disease
~5 in 10,000
Post-Dx
Survival
~4 years
At least one misdiagnosis
~55%
Two or more misdiagnosis
38%
Initially attributed to age related symptoms:
72%
shortness of breath
dry cough
doctor can hear velcro crackles
Cannot always be seen on CXR
PCP workflow demands
Problem
Highlights:
*Onishchenko, D., Marlowe, R.J., Ngufor, C.G. et al. Screening for idiopathic pulmonary fibrosis using comorbidity signatures in electronic health records. Nat Med 28, 2107–2116 (2022). https://doi.org/10.1038/s41591-022-02010-y
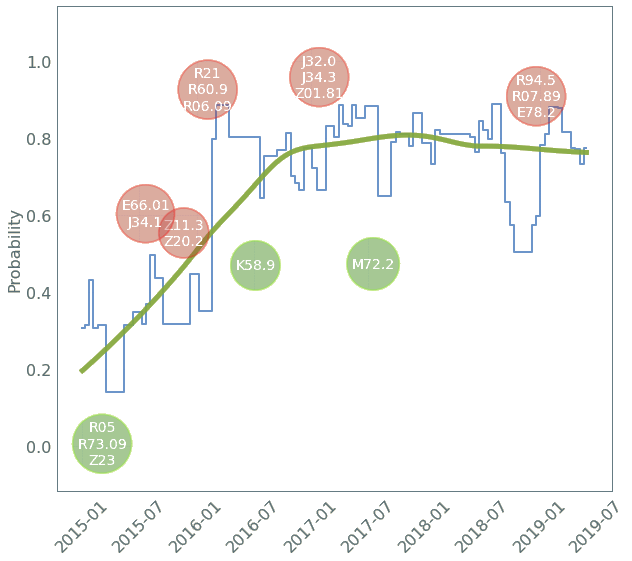
Model
time
Patient A
Patient B
Personalized Risk Factors
& Patient Journeys
ZeBRA score
IPF prevalence: 10-25% of ILD
IPF prevalence: 10-25% of ILD
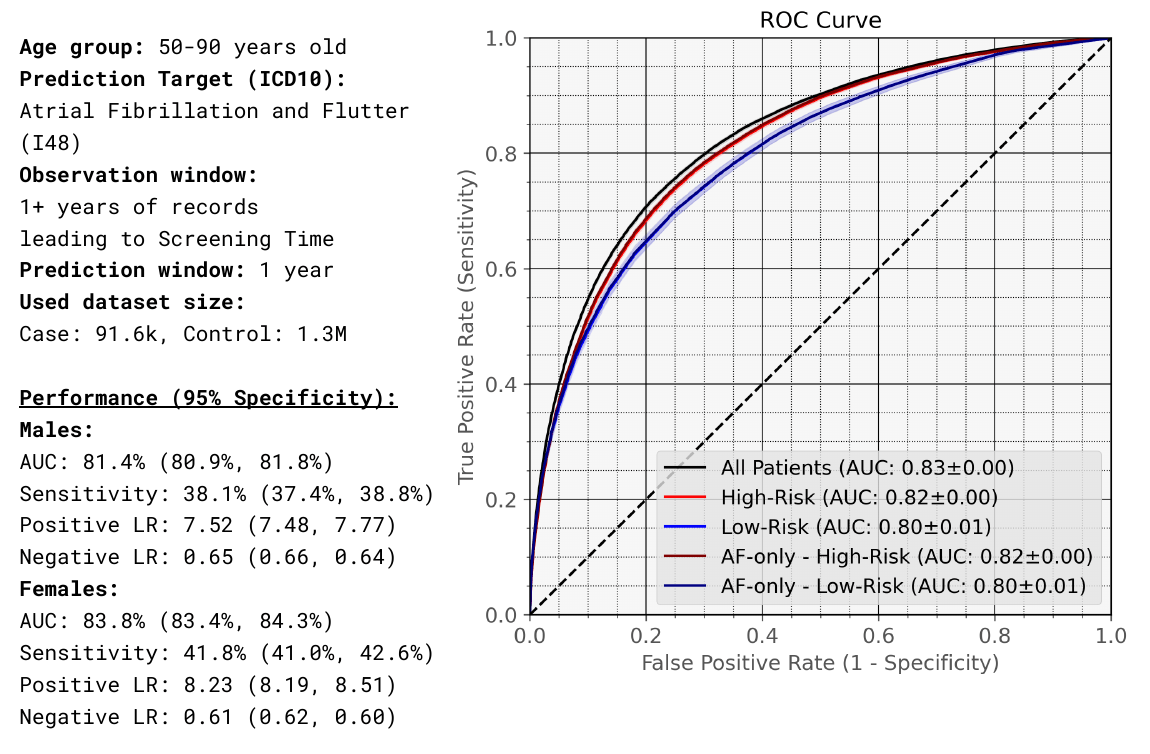
Age group: 50-85 years old
Observation window:
1+ years of records
Prediction window: 1 year
Used dataset size:
Case: 25.4k, Control: 15.1M
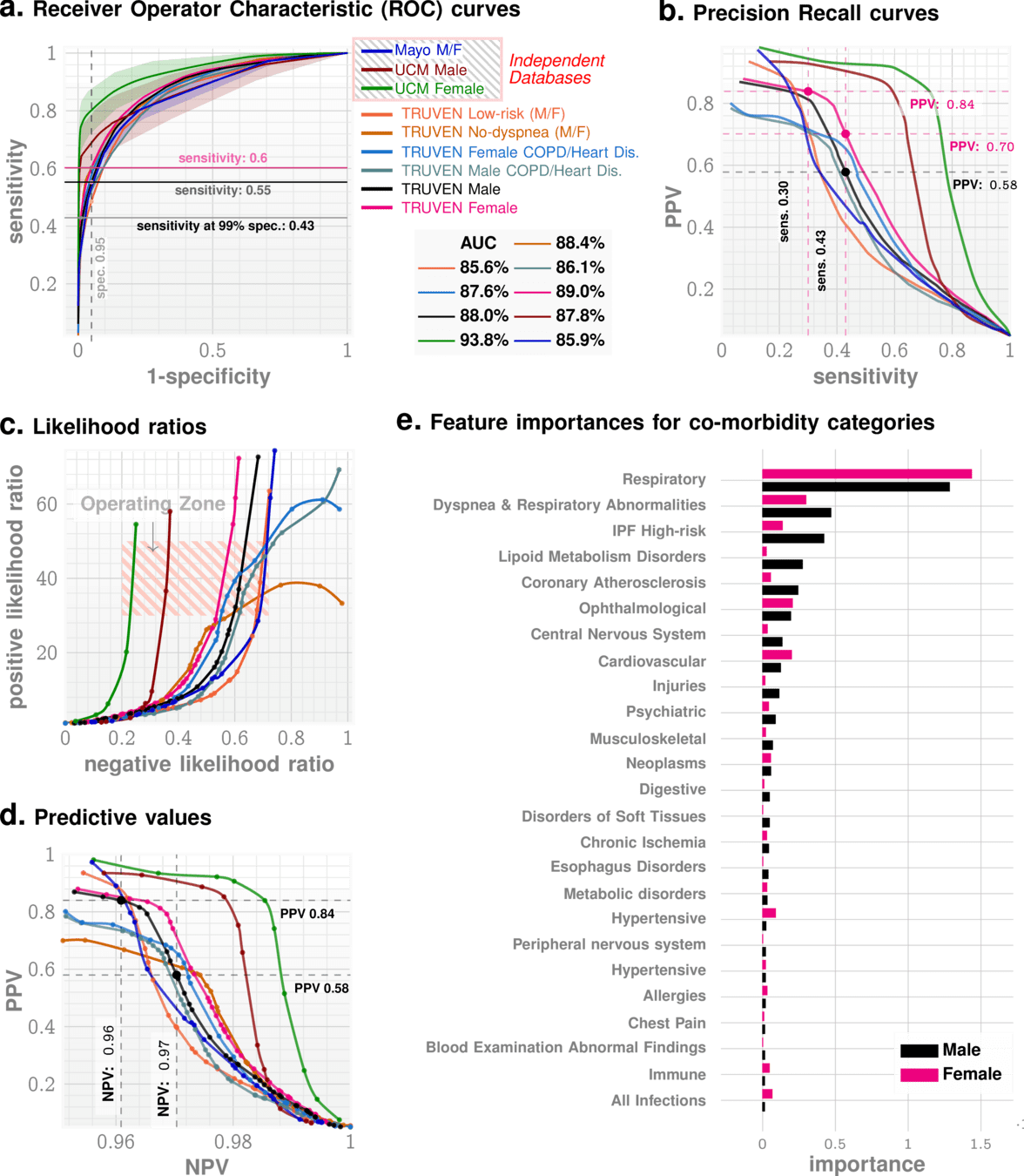
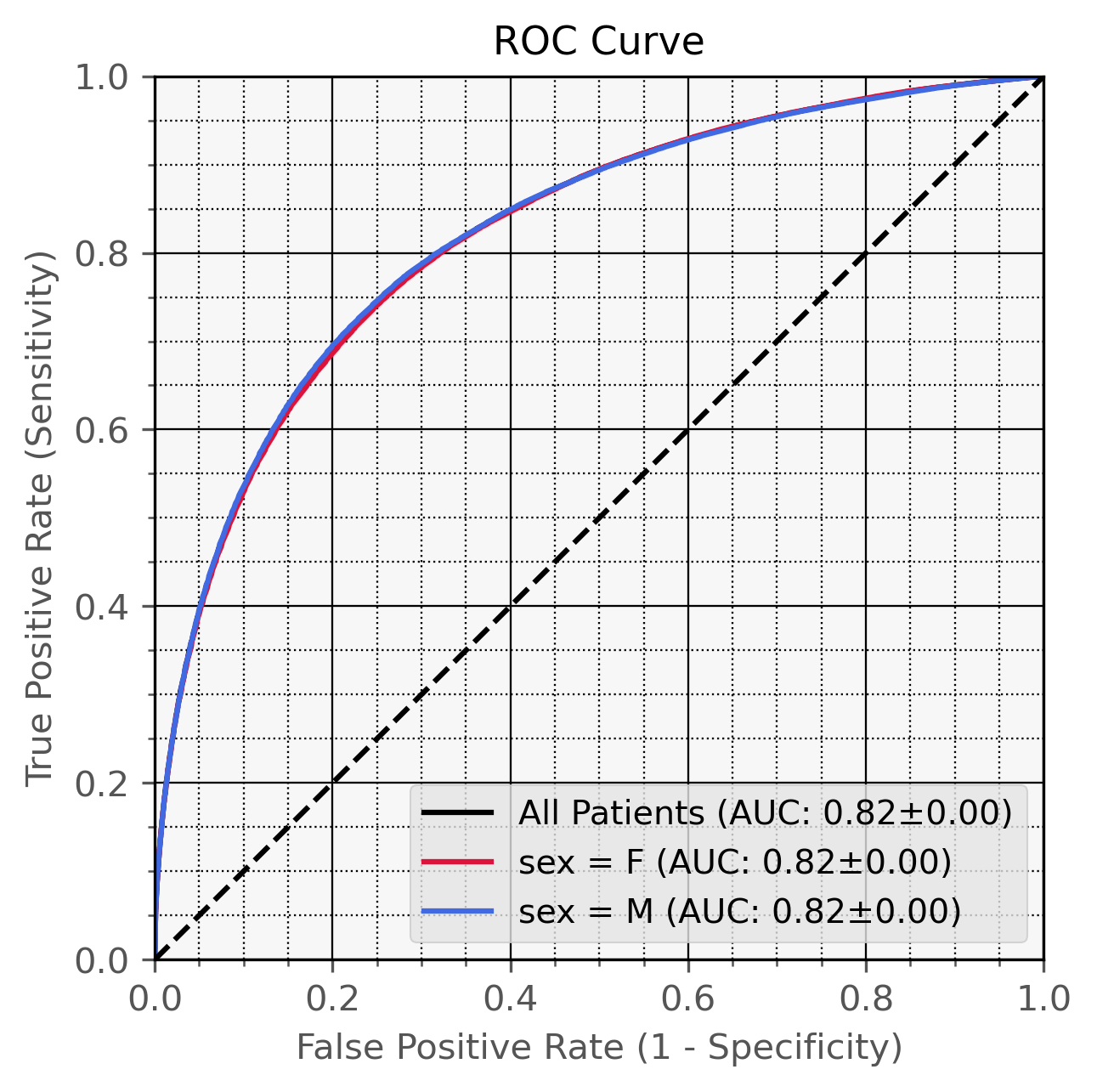
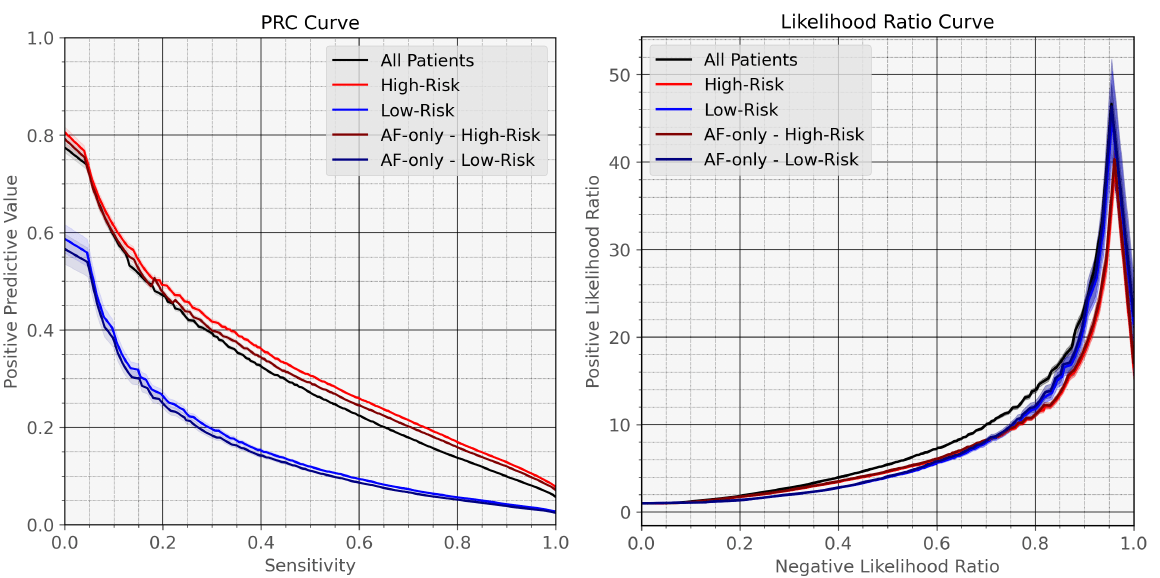
Performance (95% Specificity):
Males:
AUC 82.2% (82.0%, 82.5%)
Sensitivity 39.7% (39.3%, 40.1%)
Positive LR: 7.81 (7.85, 8.01)
Negative LR: 0.64 (0.64, 0.63)
Females:
AUC 82.1% (81.8%, 82.3%)
Sensitivity 39.1% (38.7%, 39.5%)
Positive LR: 7.77 (7.74, 7.90)
Negative LR: 0.64 (0.65, 0.64)
| 95% specificity/39% sensitivity | 99% specificity/17% sensitivity | 99.5% specificity/12.5% sensitivity | |
|---|---|---|---|
| Additional ILD diagnoses from ZeBRA | 546 | 238 | 175 |
| Total ILD diagnoses per year with ZeBRA | 746 | 438 | 375 |
| Additional transplant-eligible patients with ZeBRA | 164 | 71 | 53 |
| Expected False Positives | 29,930 | 5,986 | 2,993 |
| Net annual contribution margin* | $46,613,500 | $12,706,700 | $7,703,350 |
|---|
Patient population: 600K unique patients per year Current ILD diagnoses: 200 per year
* diagnostic workup margin (CT+PFT): $950, lunng transplant contribution margin: $120,000, incremental program operating cost: -$1.5M
Current diagnosis: based on cognitive assessments, often delayed or missed
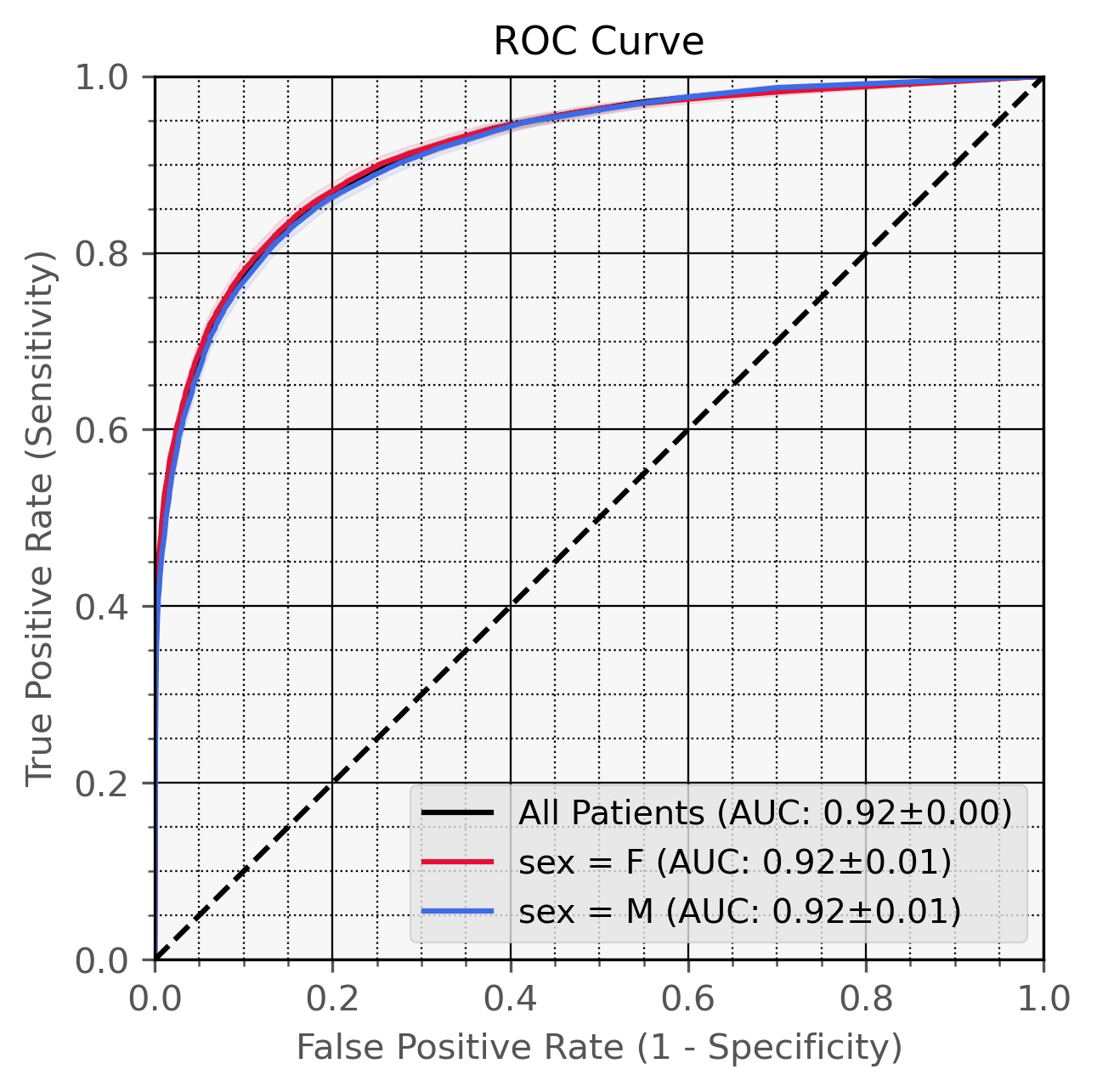
| Target | AUC |
|---|---|
| Frailty / Physical Debility | 96.2% |
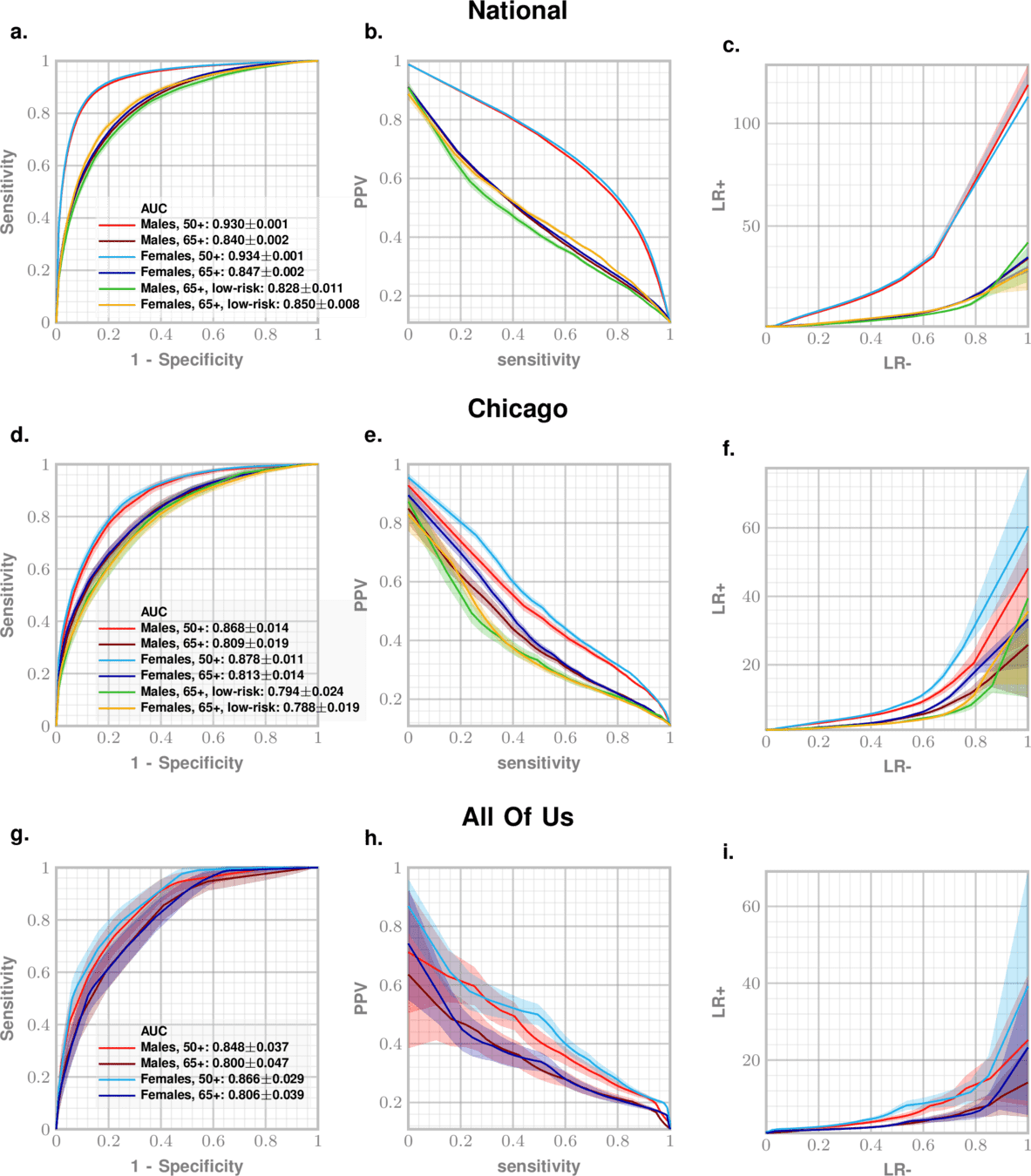
| Alzheimer's Disease and Related Dementia (ADRD) | 93.4% |
| Chronic Fatigue Syndrome / ME | 93.2% |
| Acute Pancreatitis: ICU Visit | 92.3% |
| Chronic Pancreatitis: Exocrine Pancreatic Insufficiency | 92.1% |
| Idiopathic Pulmonary Fibrosis (IPF) | 91.6% |
| Sarcopenia | 91.0% |
| Parkinson's Disease | 87.9% |
| Dementia / Degenerative Neurologic Disease | 87.8% |
| Acute Pancreatitis: Insulin Dependence | 87.2% |
| Suicide Attempts / Suicidal Ideations (Males 50--75) | 86.0% |
| Chronic Inflammation | 85.9% |
| Heart Failure with Preserved Ejection Fraction (HFpEF) | 84.9% |
| Suicide Attempts / Suicidal Ideations (Males 25--50) | 84.0% |
| Interstitial Lung Diseases (ILD) | 82.2% |
| Age-related Macular Degeneration | 82.1% |
| Autism Spectrum Disorder (ASD) | 81.8% |
| Chronic Kidney Disease (CKD) | 81.8% |
| Cerebral Infarction | 81.1% |
| Chronic Obstructive Pulmonary Disease (COPD) | 81.0% |
| Major Depressive Disorder | 80.5% |
| Myocardial Infarction / Cardiac Arrest post-arthroplasty | 80.1% |
| CKD Progression to Stage 4+ | 80.1% |
| Prostate Cancer | 80.0% |
| Osteoporosis | 79.5% |
| Post-Traumatic Stress Disorder (PTSD) | 78.1% |
| Hearing Loss | 72.7% |
| Osteoarthritis | 72.5% |
| Systemic Connective Tissue Disorders | 72.0% |
[
{
"patient_id": "P000038",
"sex": "F",
"birth_date": "01-01-2006",
"DX_record": [
{"date": "07-31-2006", "code": "Z38.00"},
{"date": "08-07-2006", "code": "P59.9"},
{"date": "08-29-2016", "code": "J01.90"},
{"date": "09-10-2016", "code": "J01.90"},
{"date": "11-14-2016", "code": "J01.91"}
],
"RX_record": [
{"date": "10-29-2011", "code": "rxLDA017"},
{"date": "05-16-2015", "code": "rxIDG004"},
{"date": "08-08-2015", "code": "rxIDG004"},
{"date": "06-04-2016", "code": "rxIDD013"}
],
"PROC_record": [
{"date": "02-05-2007", "code": "90723"},
{"date": "11-05-2007", "code": "J1100"}
]
}
]{
"predictions": [
{
"error_code": "",
"patient_id": "P000012",
"predicted_risk": 0.005794344620009157,
"probability": 0.8253881317184486
}
],
"target": "TARGET"
}Data Out
Data In
*Documentation: https://github.com/zeroknowledgediscovery/paraknowledgedoc
Model ready to deploy behind UK firewall
By Ishanu Chattopadhyay
Brief talk on the ZeBRA Platform



