BOTULINUM TOXIN INJECTIONS IN FACIAL SPASM-PITFALLS
BLEPHAROSPASM
-
Bilateral forceful contraction of orbicularis oculi
-
Occurs 5-10/100,000
- Associated with frequent blinking and closure of eyes which can lead to functional blindness
BLEPHAROSPASM
May present as:
- Focal dystonia
BLEPHAROSPASM
Cranial dystonia (Mieges syndrome)
BLEPHAROSPASM
- May be primary (essential blepharospasm) or secondary
- Causes
- Tardive syndromes
- Parkinsonian syndromes PD,PSP,MSA
- Brainstem pathology
APRAXIA OF EYELID OPENING
- Mechanism not clear
- Levator inhibition
- Pretarsal blepharospasm
- Frontalis is used to try to elevate
- Occurs in PSP and other
- Parkinsonian states but can occur in isolation
- EMG of pretarsal muscles shows activity suggesting this inhibits contraction of LPS
HEMIFACIAL SPASM
BOTULINUM TOXIN IN THE TREATMENT OF BLEPHAROSPASM
- Small number of double-blind studies and a considerable number of open case-control studies suggesting up to 90% benefit.
- Only 3 class one studies- total number of patients 22 for blepharospasm.(Fahn et al, 1985 (5 patients), Jankovic and Orman, 1987 (11 patients) Girlanda et al, 1996) 6 patients.
- A recent Cochrane review found no randomized controlled trials with sufficient numbers of patients to fit the inclusion criteria but the considerable effect size made placebo-controlled trials of blepharospasm treatment with BoNT type A impractical and perhaps unethical (Costa et al, 2005).
- Roggenkamper etal 2006- 256 patients with blepharospasm compared Xeomin with Botox
- Even fewer studies comparing techniques – no class one studies. Wide variation in the position of injection sites – orbital, preseptal, pretarsal or mixtures of all sites.
BLEPHAROSPASM TREATMENT WITH BOTULINUM TOXIN
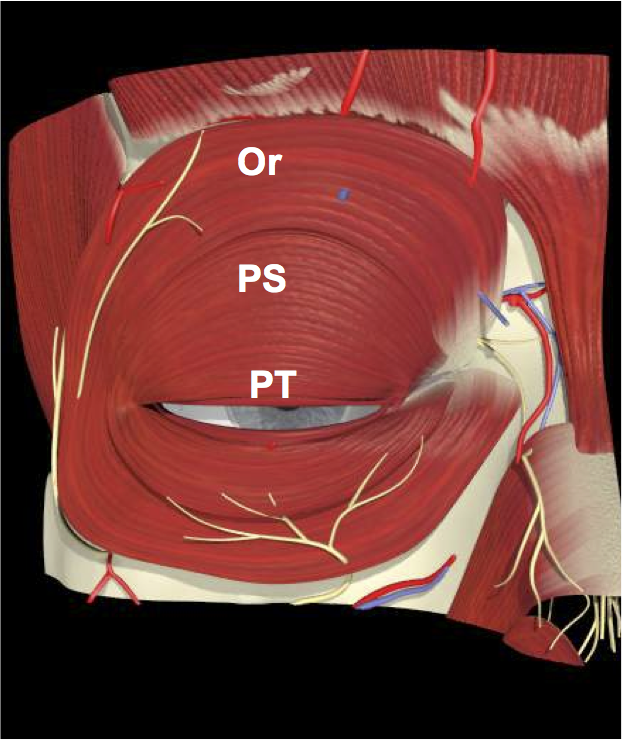
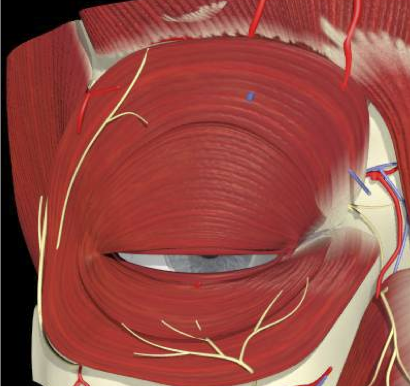
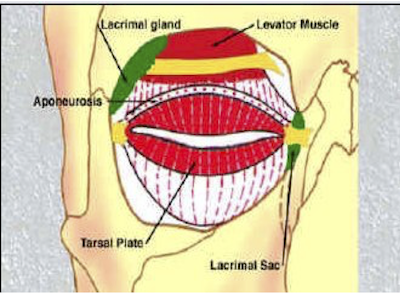
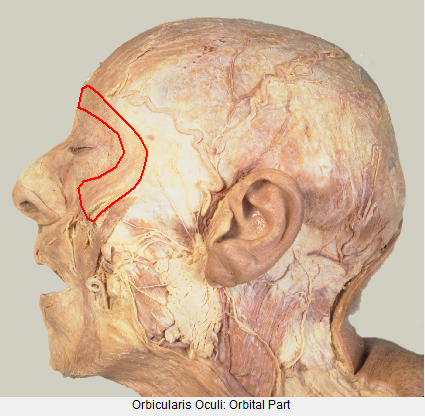
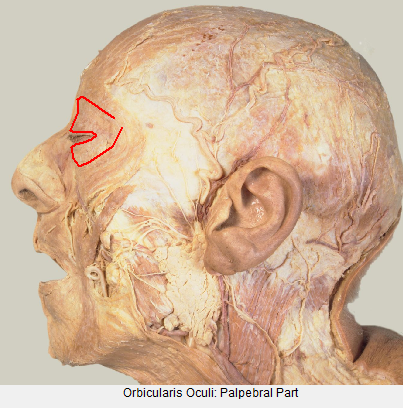
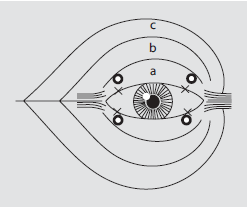
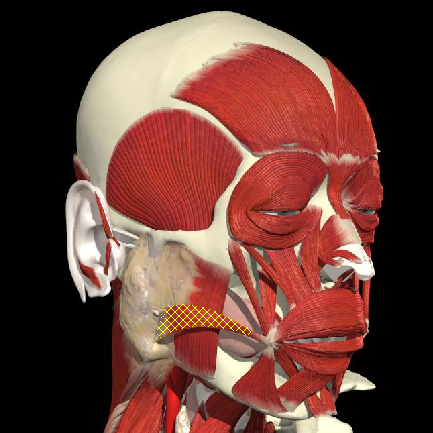
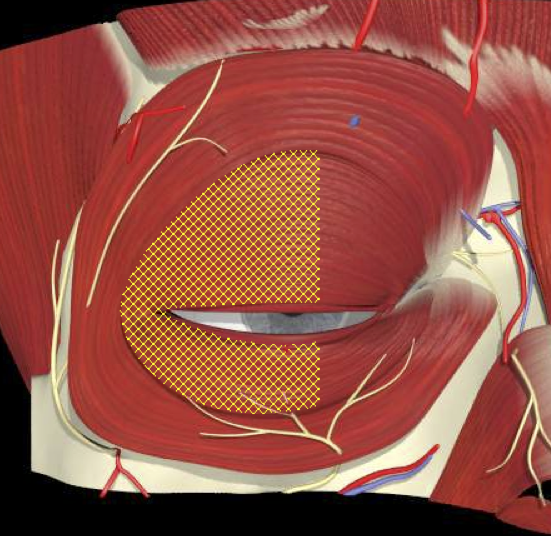
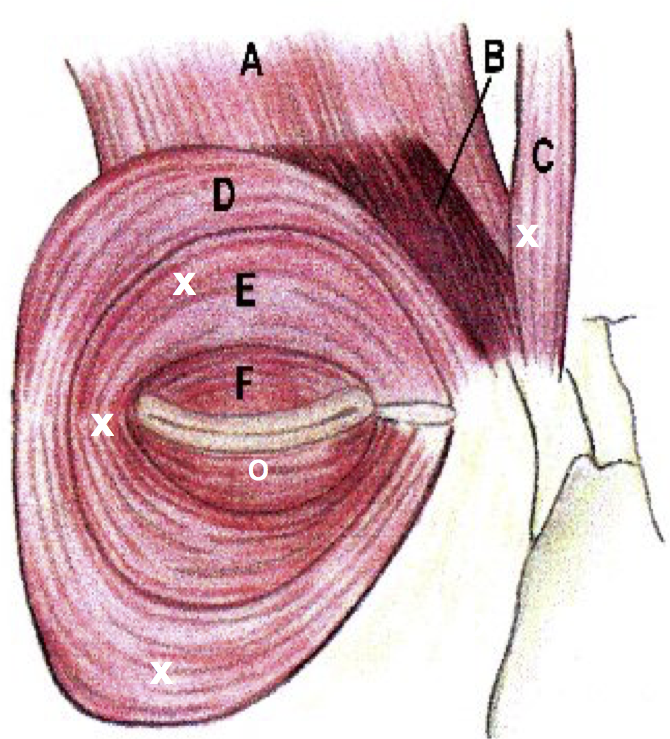
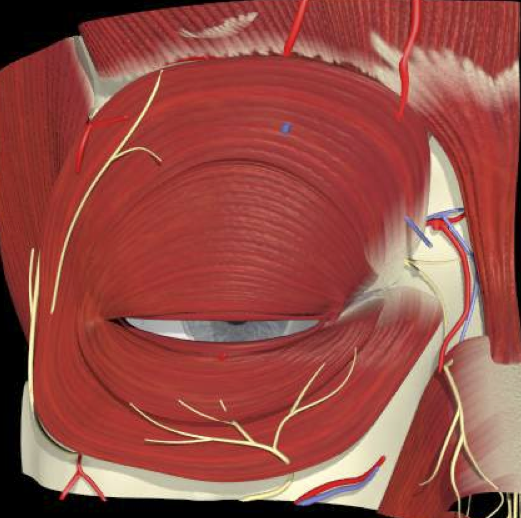
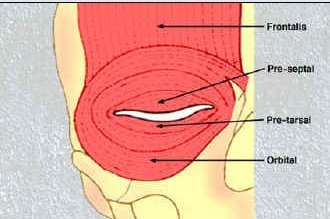
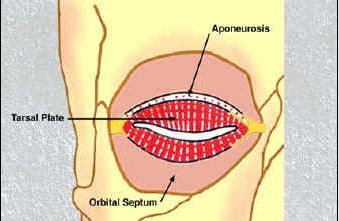
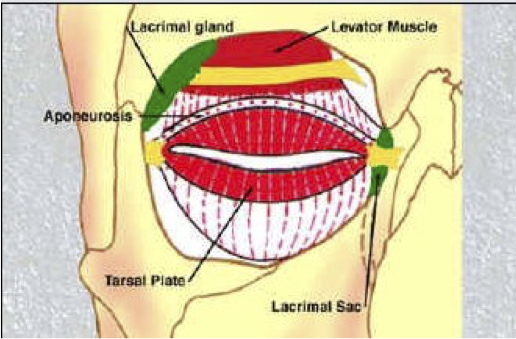
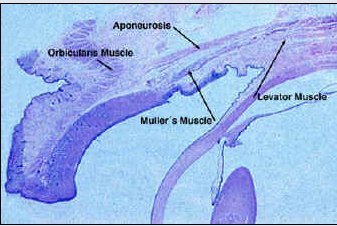
ORBICULARIS OCULI ANATOMY
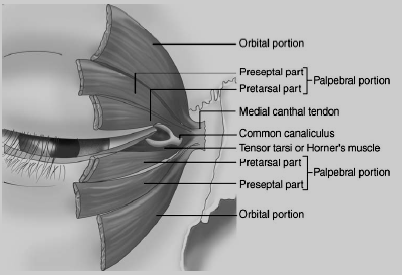
ORBICULARIS OCULI FUNCTION
- Orbital portion closes the lids, drawing the skin of the forehead, temple and cheek medially.
- The palpebral portion of orbicularis closes the lids grossly, but incompletely, for long periods of time.
- Located next to the lid margin the pretarsal and Riolan’s muscle, provides closure for brief periods oftime, as in reflex or involuntary blinking.
- (Horner’s tensor tarsi) encircles canaliculi to facilitate tear drainage.
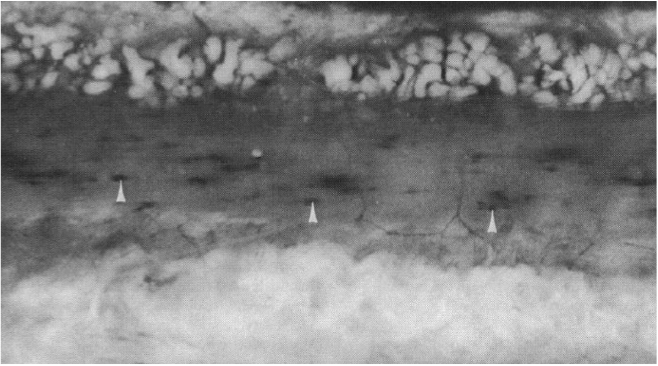
FUNCTIONAL ANATOMY
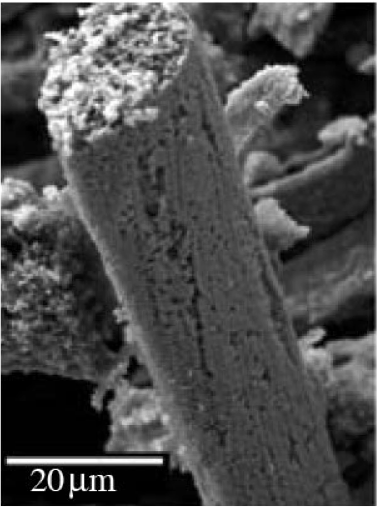
Differences in fibre cross-sectional areas and in fibre type
- At increasing distances from the eyelid margin there is a gradual increase in fiber cross-sectional area and in the proportion of type I fibres (slow-twitch).
- The pretarsal region including Riolans muscle is almost 100%type 2 fibers (fast twitch). Fibres have an average cross sectional area of 400 um2 and contain only 3% to 4% type I fibers.
- Fibres in the preseptal region have an average cross-sectional area of 550 um2 and contain between 8% and 15% type I fibers
FUNCTIONAL ANATOMY
-
The differences may reflect the activity and function of the orbicularis oculi during eye blink and forceful eyelid contraction i.e fast twitch and slow twitch
- Experimental work on rat calf muscles showed that the recovery of type I muscle fibres from botulinum toxin is much faster than that of type II fibres (Hassan SM et al Muscle and Nerve 1994)
FUNCTIONAL ANATOMY
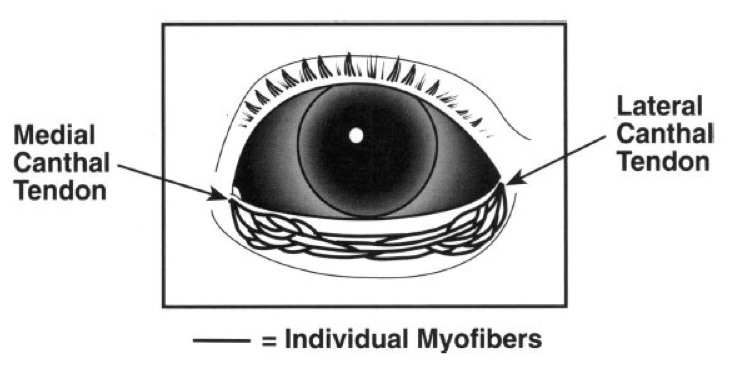
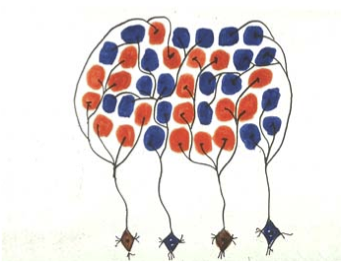
Pretarsal-Riolans muscle organized with short myofibres within longer muscle
Creates possibility of patterned, sequential, wave of recruitment of short myofibers
within a longer muscle, a possibility that may be applicable to functioning of lacrimal pump
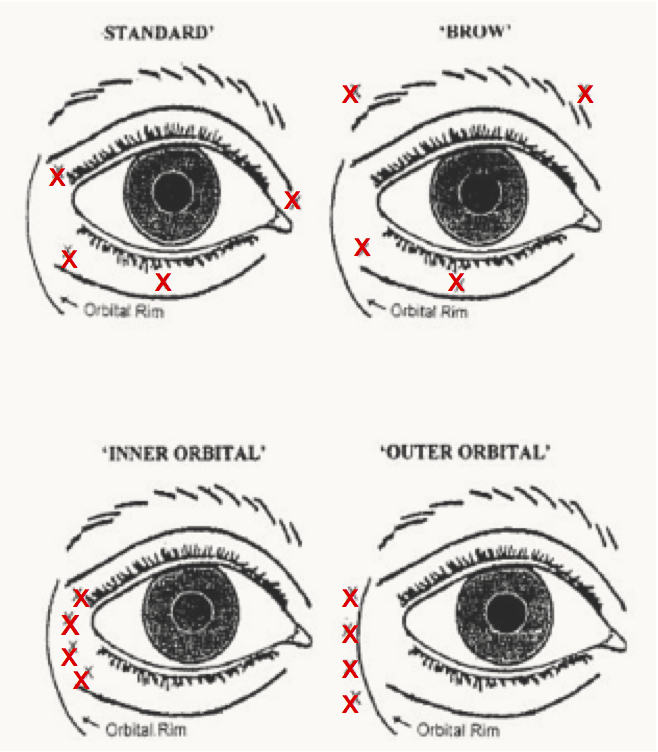
INJECTION TECHNIQUES
Price et al 1997 (Ophthalmology)
- 50 patients blepharospasm, 42 patients with hemifacial spasm
- 2.5 units per site
- Randomized into 4 groups
- Standard technique “had greater duration of action and “outer orbital” least. Brow equally effective in hemifacial spasm.
- ST more Epiphoria
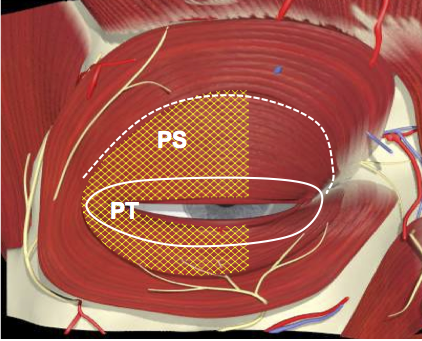
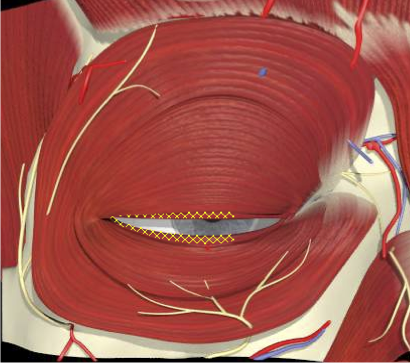
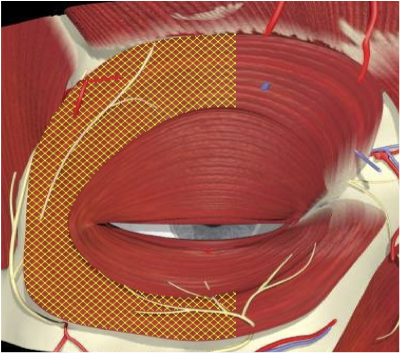
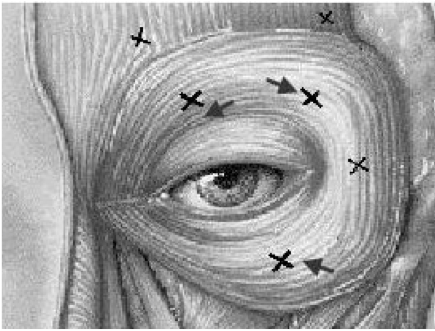
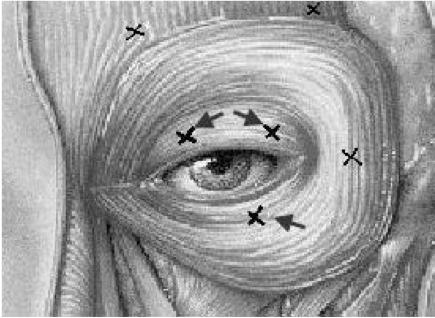
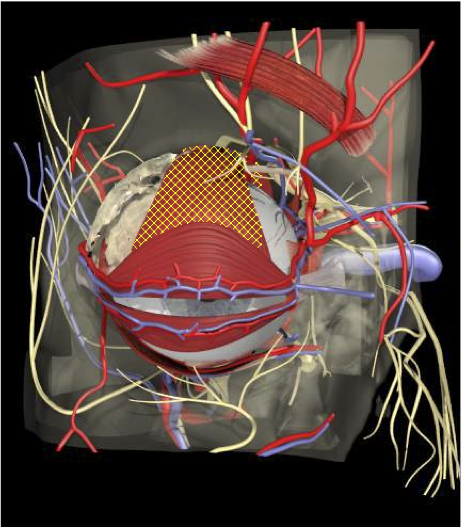
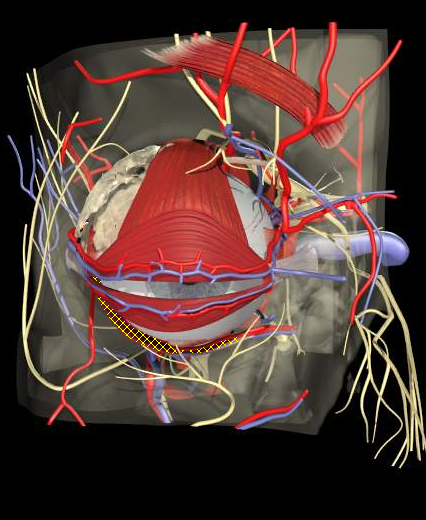
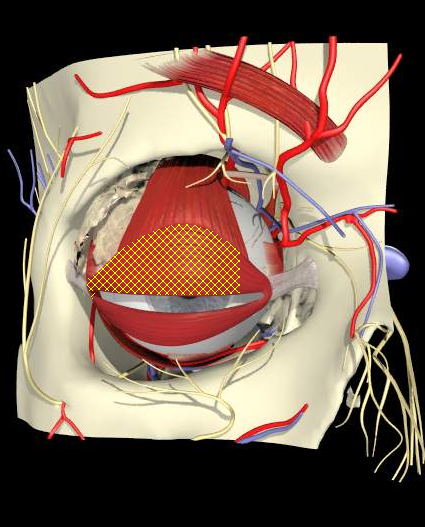
INJECTION TECHNIQUE - PRETARSAL VERSUS PRESEPTAL
Cakmur etal 2002 J Neurol
- 53 patients (25 blepharospasm, 28 hemifacial spasm)
- PT higher response rate and longer duration of action
- PT less ptosis more blurred vision
Other comparative studies Albenese etal 1996, Aramideh et al 1995, Jankovic 1996, Kowal 1997 have found similar results.
Pre Septal
Pre Tarsal
INJECTION TECHNIQUES
Mechanism of superior benefit of pretarsal technique
-
Involuntary blinking, lid closure a function of pretarsal muscles. Pretarsal motor units are probably more susceptible to alterations in spontaneous supranuclear signals and are less under voluntary control
- Pretarsal muscles mainly type II –longer duration effect with Botulinum Toxin
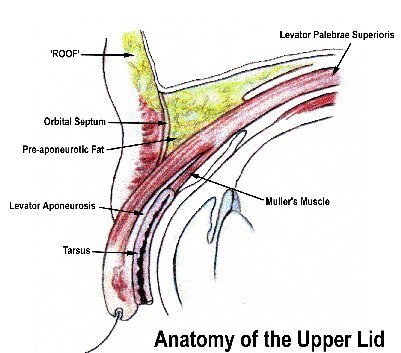
Ptosis
- Levator palpebrae becomes aponeurotic already at the level of the superior transverse ligament 14 to 20 mm above the tarsus. Preseptal injections closer
INJECTION TECHNIQUE - SIDE EFFECT PROFILE

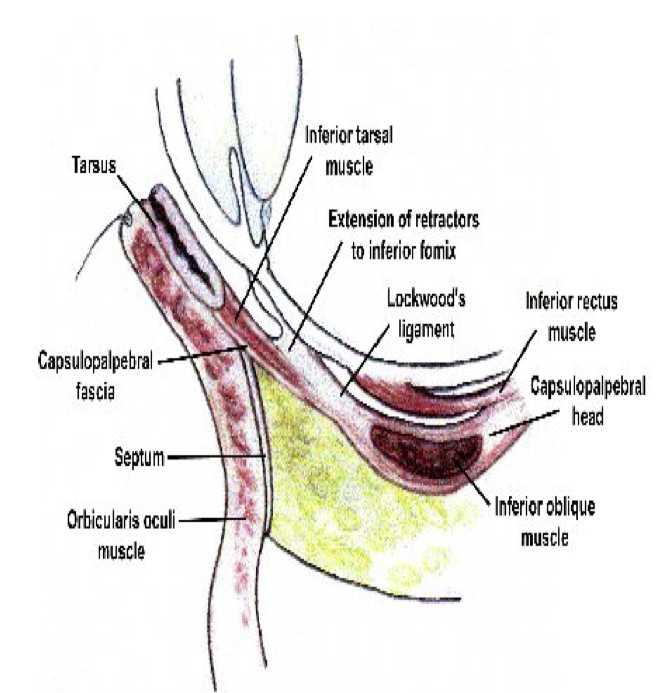
Diplopia
- Inferior Oblique weakness
- Proximity of medial LL PT injections to IO muscle
- Higher incidence in PT injections
INJECTION TECHNIQUE - SIDE EFFECT PROFILE
- Epiphoria, tearing and blurred vision
- Proximity of PT to pretarsal muscles, Riolans muscle and Horners muscle
- Difficulty with opposing lids and lacrimal function
INJECTION TECHNIQUE - SIDE EFFECT PROFILE
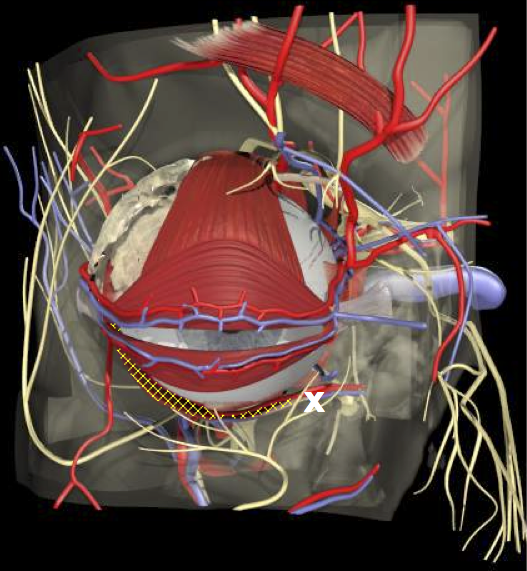
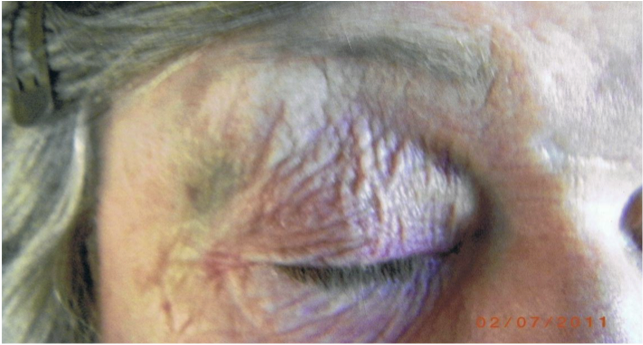
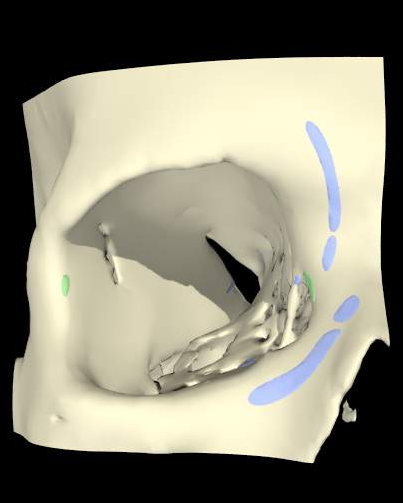
Superficial veins near lid margins
INJECTION TECHNIQUE - SIDE EFFECT PROFILE
Bruising
- Pitfalls with O Oculi injections
INJECTION TECHNIQUE - SIDE EFFECT PROFILE
- Dropping angle of mouth (lower lateral injection)
- Nasolabial fold
- Inability to elevate upper lip. (lower medial injection)
Need VIDEO

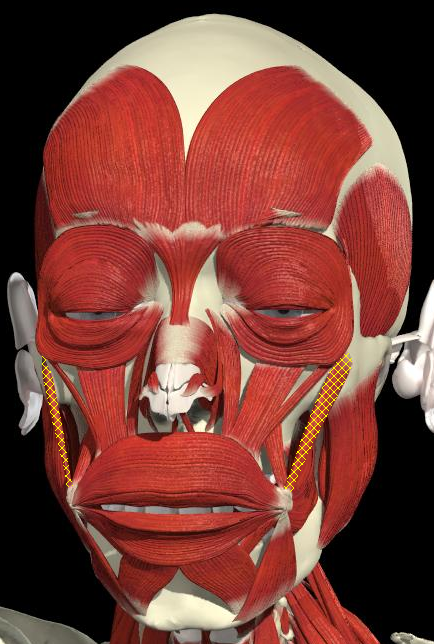
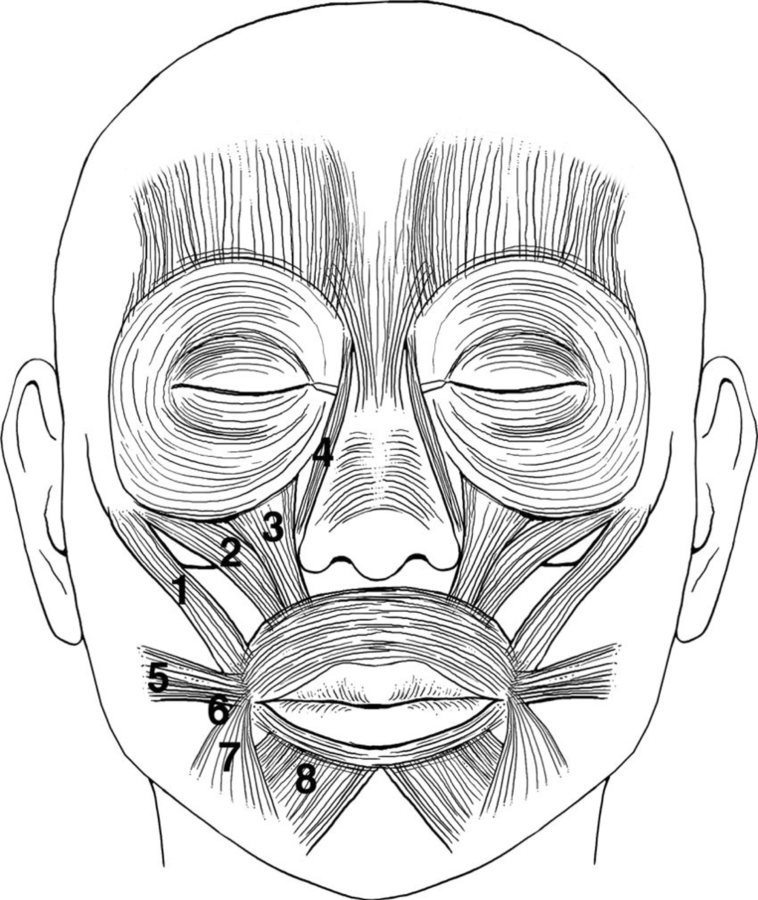
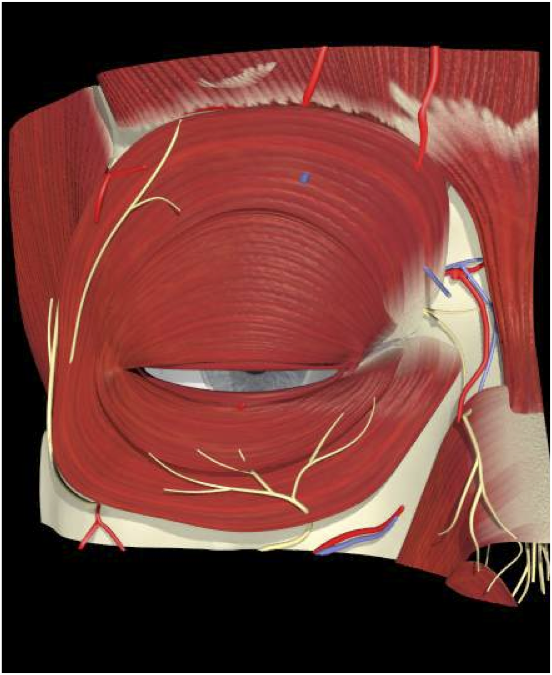
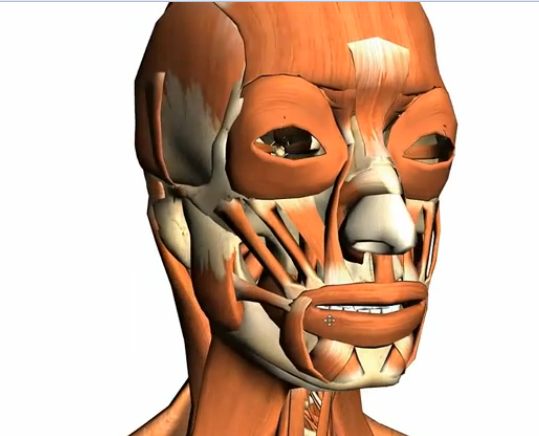
UPPER FACIAL MUSCLE OVERLAP
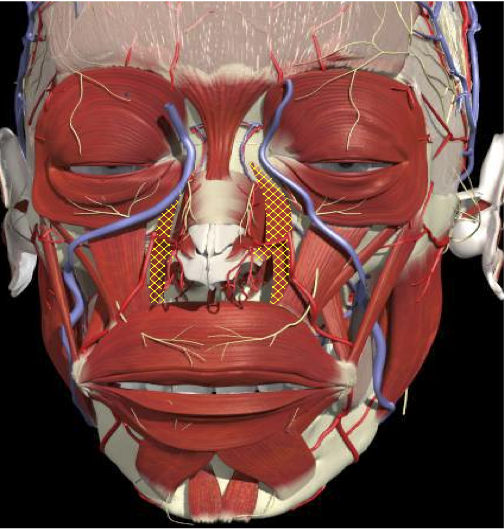
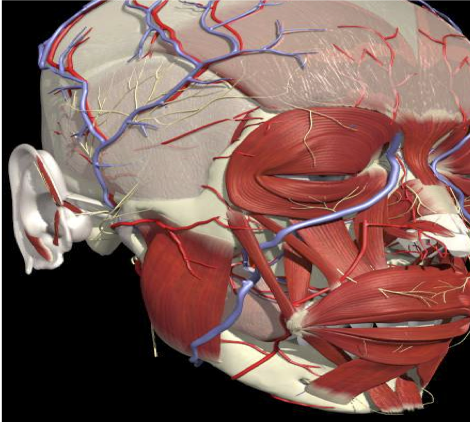
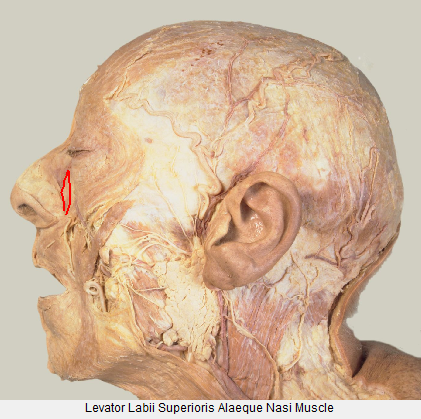
Levator Labii Superioris Alequa Nasi
Levator Labii Superioris
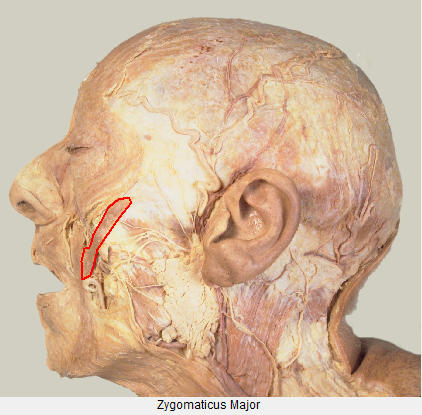
Zygomaticus Major
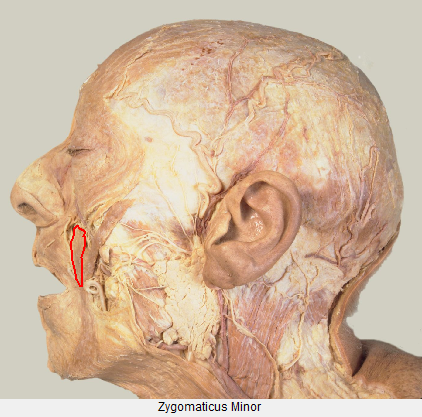
Zygomaticus Minor
Levator Anguli Oris
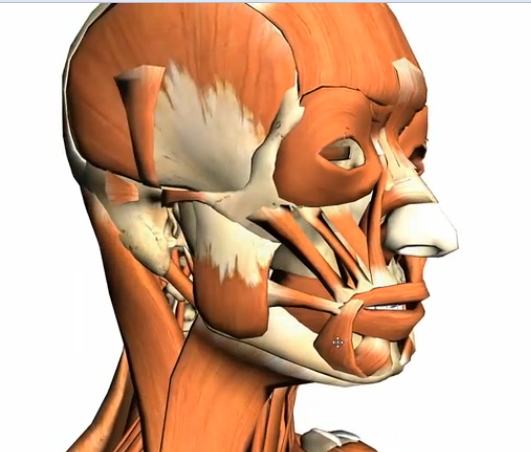
UPPER FACIAL MUSCLE OVERLAP
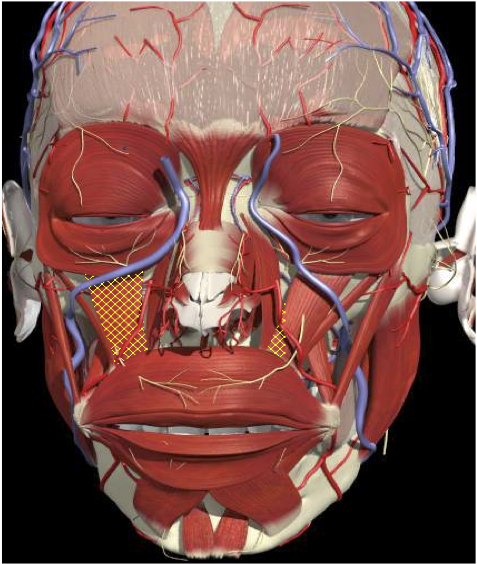
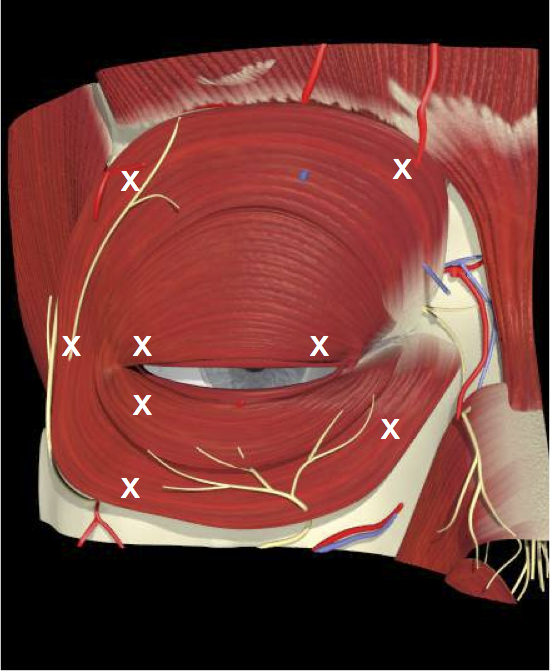
ORBICULARIS OCULI MUSCLE OVERLAP
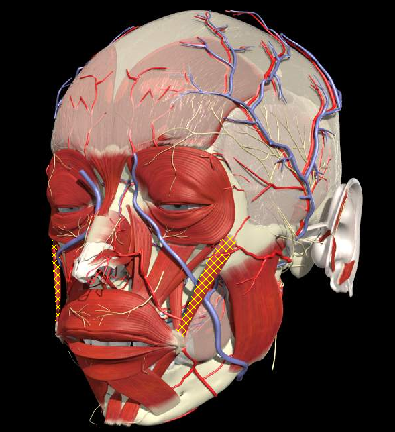
ORBICULARIS OCULI OVERLAP

ORBICULARIS OCULI OVERLAP
Levator Labii Superioris Alaeque Nasi
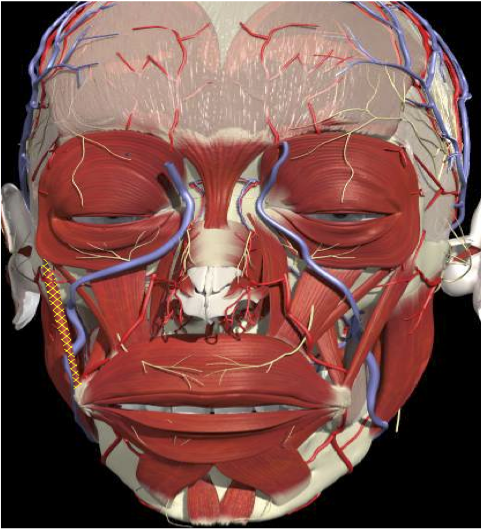
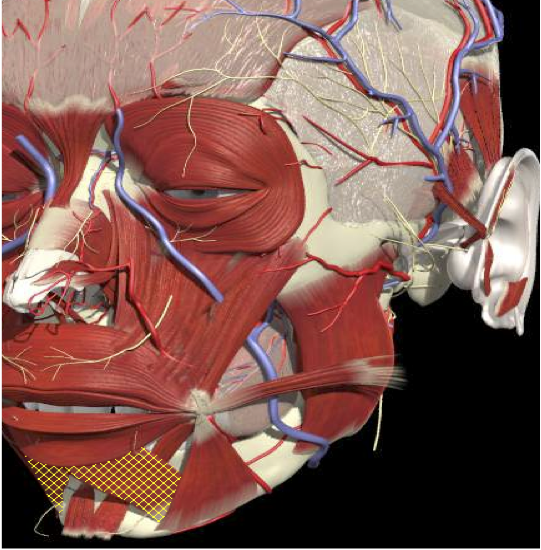
LOWER FACE MUSCLE OVERLAP

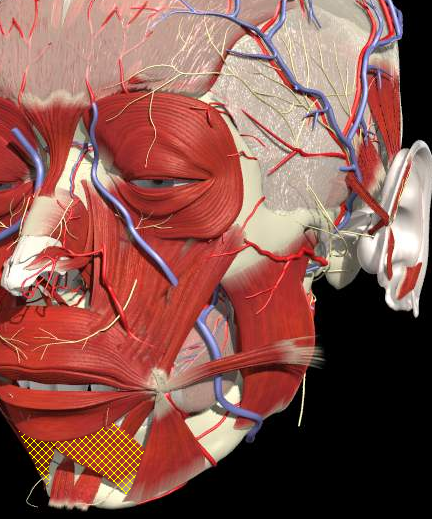
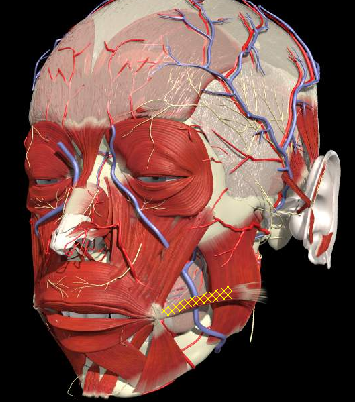
LOWER FACE MUSCLE OVERLAP
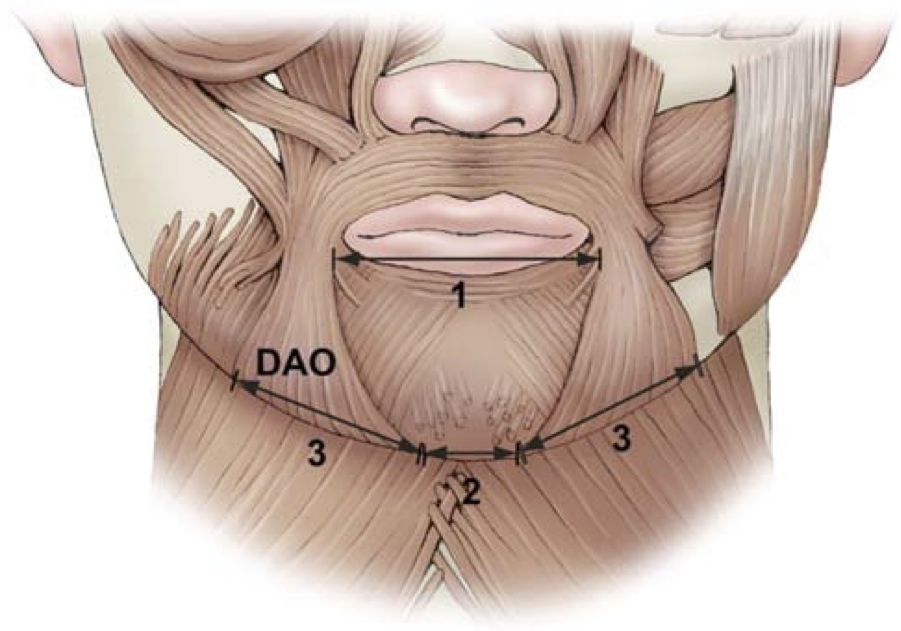
PITFALLS
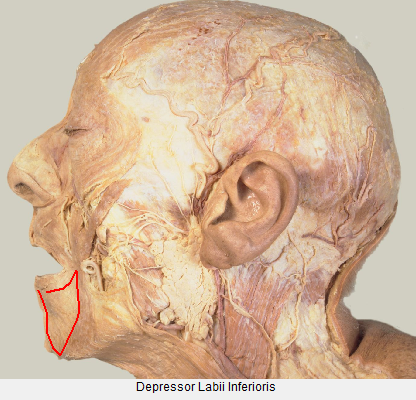
(1) Injections that are too medial can cause an ipsilateral weakness of the depressor labii inferioris muscle and flattening of the lower lip contour when the mouth attempts to form an “O”.
(2) Injections that are too high can interfere with the sphincter function of the orbicularis oris muscle, leading to difficulties with speech and suction.
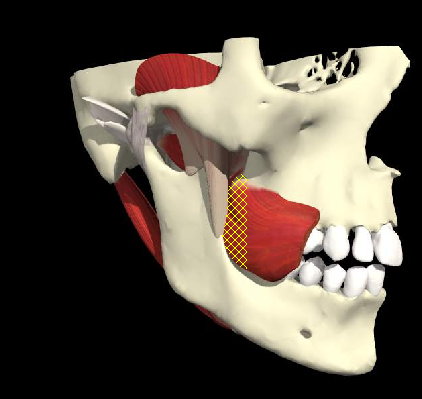
(3) Injections that are too posterior can affect the buccinator so as to result in chewing diffculties.
LOWER FACE MUSCLE OVERLAP
Risorius
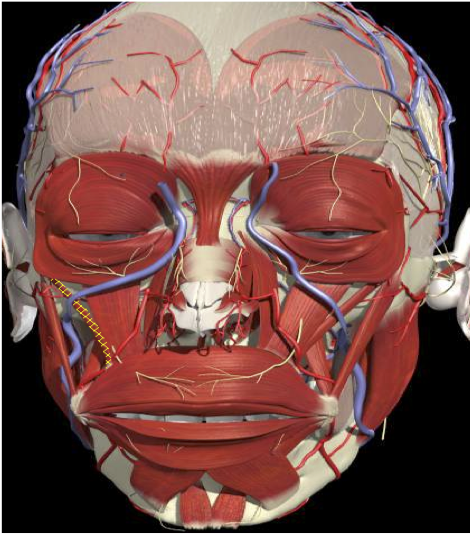
LOWER FACE MUSCLE OVERLAP
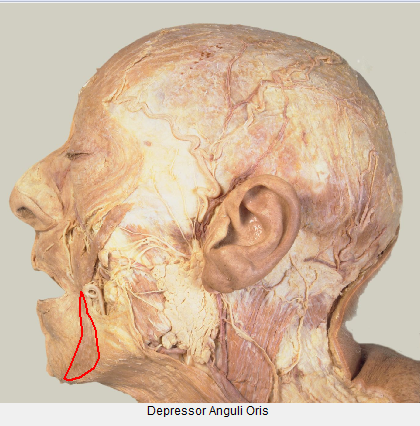
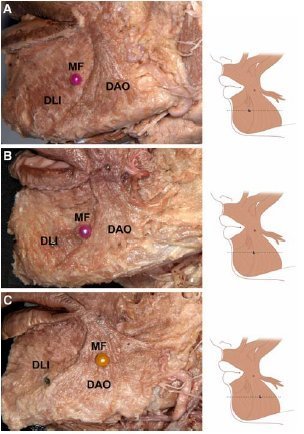
DAO
LOWER FACE MUSCLE OVERLAP
DLI
MEN
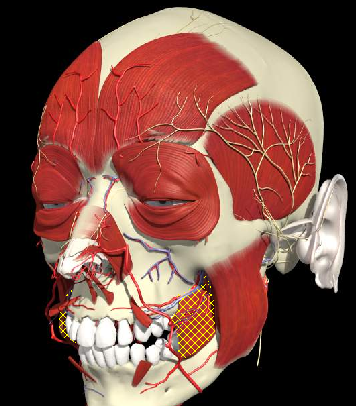
SURFACE ANATOMY LOWER FACIAL MUSCLES
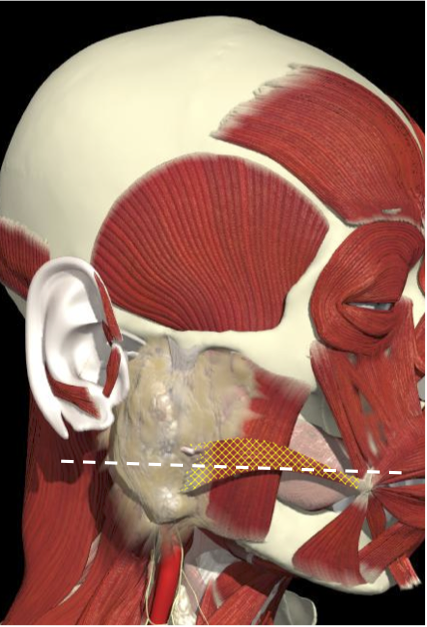
Risorius
Horizontal line from angle of mouth to tragus of ear and in front of border of masseter.
Line from lateral surface of zygomatic (in front of masseter insertion) bone to angle of mouth

ZYGOMATICUS MAJOR
More likely to develop weakness at lower dose therefore dose need to be adjusted
HEMIFACIAL SPASM IN SETTING OF FACIAL PALSY
- Involuntary eyelid closure due to failure of levator palpebrae superioris to contract.
- Occurs in PSP and other Parkinsonian states but can occur in isolation.
- Should be suspected if Blepharospasm is resistant to Botulinum toxin.
- Dystonia- EMG of pretarsal muscles shows activity suggesting this inhibits contraction of LBS.
APRAXIA OF EYELID OPENING
- Dilution
- Dose
INJECTION SITES

FACIAL INJECTIONS
Locations for facial injections
(1) Zygomatic major
(2) Zygomatic minor
(3) Levator labii superioris
(4) Levator labii superioris alaeque nasi
(5) Risorius
(6) Modiolus area
(7) Depressor anguli oris
(8) Depressor labii inferioris
INJECTION TECHNIQUES
LOWER FACE MUSCLE OVERLAP
(1) injections that are too medial can cause an ipsilateral weakness of the depressor labii inferioris muscle and flattening of the lower lip contour when the mouth attempts to form an “O”,
(2) injections that are too high can interfere with the sphincter function of the orbicularis oris muscle, leading to diYculties with speech and suction [3, 4,13]
(3) injections that are too posterior can affect the buccinator so as to result in chewing diffculties
Caution must be exercised when injecting close to the mouth, since;
LOWER FACE MUSCLE OVERLAP
UPPER FACIAL INJECTIONS
Zygomaticus
Need VIDEO
UPPER FACIAL INJECTIONS
Levator Labii Superioris
Need VIDEO
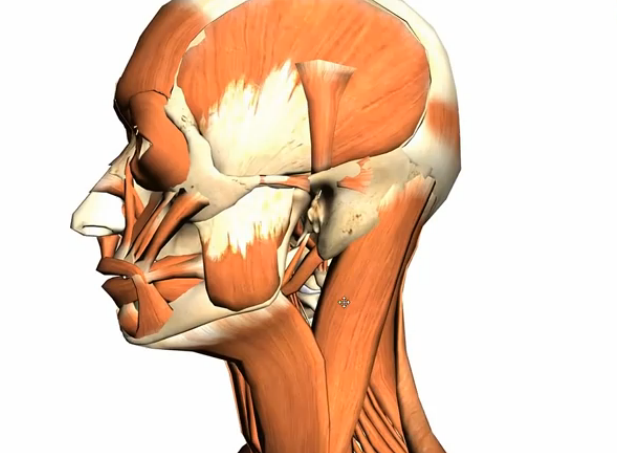
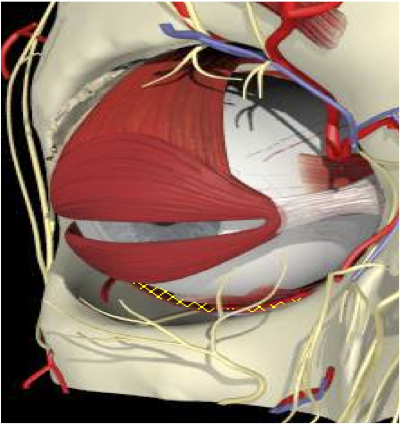
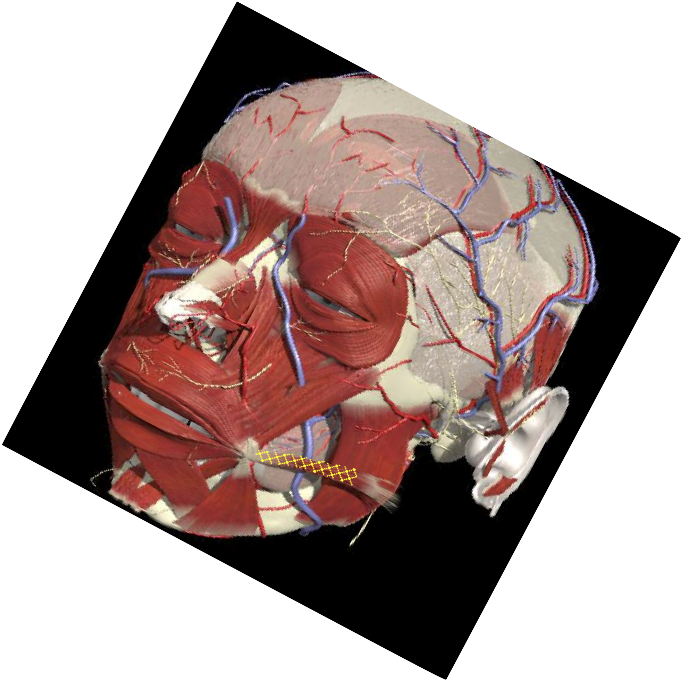
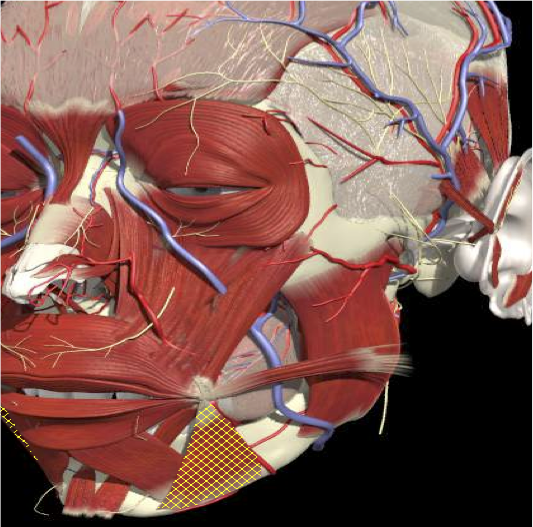
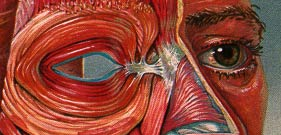
ANATOMICAL RELATIONS
BOTULINUM TOXIN IN THE TREATMENT OF FACIAL SPASMS
- The safety and efficacy of BoNT in the treatment of blepharospasm and hemifacial spasm has been demonstrated by a small number of double-blind studies and a considerable number of open case-control studies suggesting up to 90% benefit
- Only 3 class one studies- total number of patients 22 for blepharospasm.(Fahn et al, 1985 (5 patients), Jankovic and Orman, 1987 (11 patients) Girlanda et al, 1996) 6 patients
- A recent Cochrane review found no randomized controlled trials with sufficient numbers of patients to fit the inclusion criteria but the considerable effect size made placebo-controlled trials of blepharospasm treatment with BoNT type A impractical and perhaps unethical (Costa et al, 2005)
- Even fewer studies comparing techniques – no class one studies. Wide variation in the position of injection sites- orbital, preseptal, pretarsal or mixtures of all sites
ANATOMICAL RELATIONS
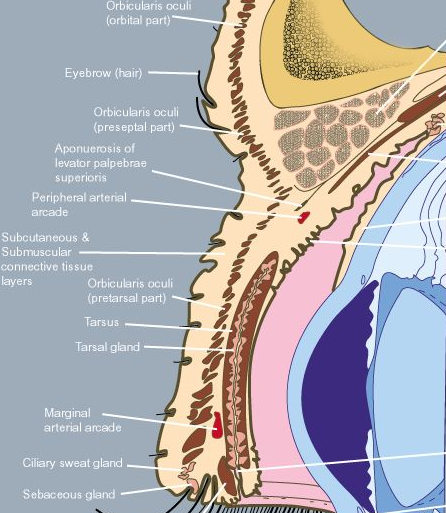
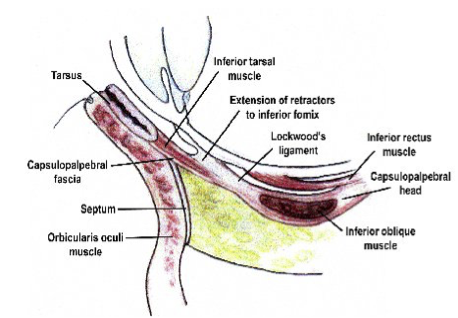
ANATOMICAL RELATIONS – CROSS SECTION
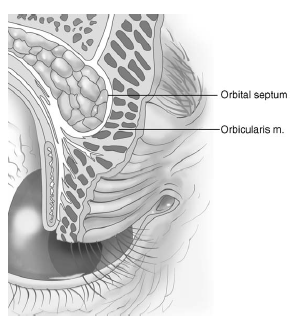
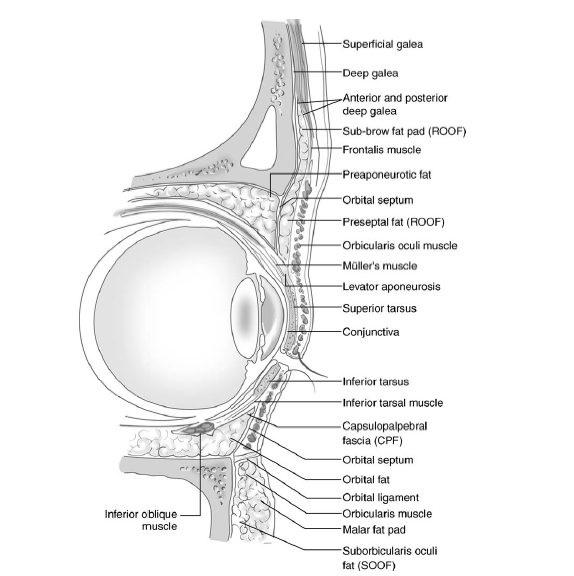
IMPORTANT RELATIONS
INJECTION TECHNIQUES
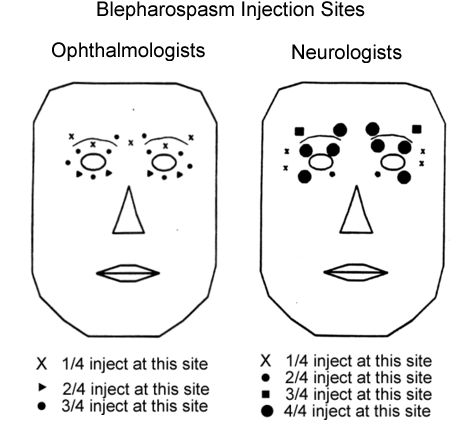
Stacey – Barrow institute
- Large variety of injection sites
- Neurologists most consistent
- Doses 30-60 units, 2.5 units per site
BOTOX Injections in Facial Spasm-Pitfalls
By Integra


