PITFALLS INJECTING CERVICAL DYSTONIA AND FACIAL SPASM
Professor Con Yiannikas
Cervical Dystonia
Cervical Dystonia
Injection Pitfalls
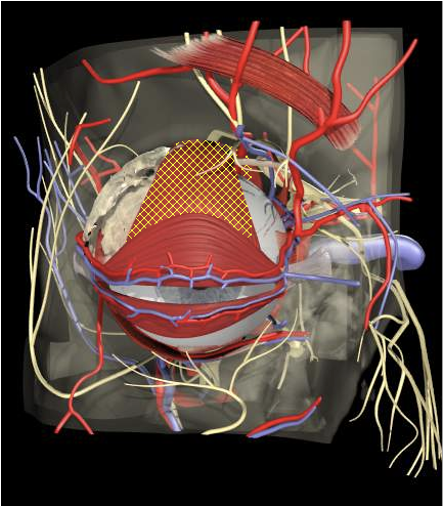
Anatomical Pitfalls
Cervical Dystonia
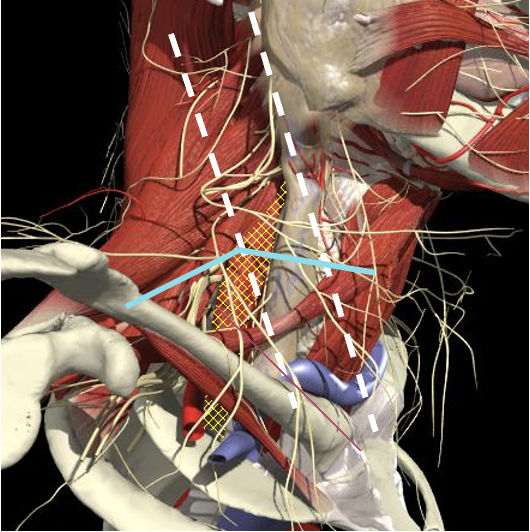
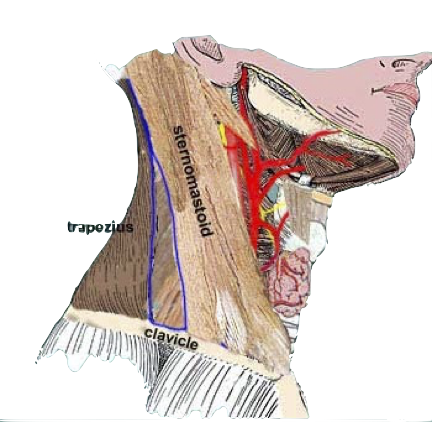
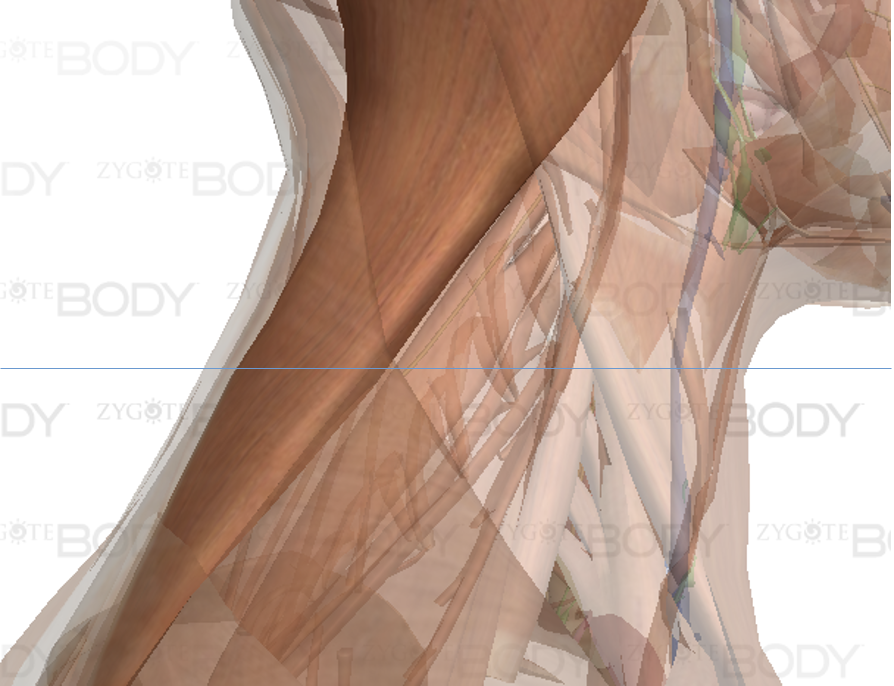
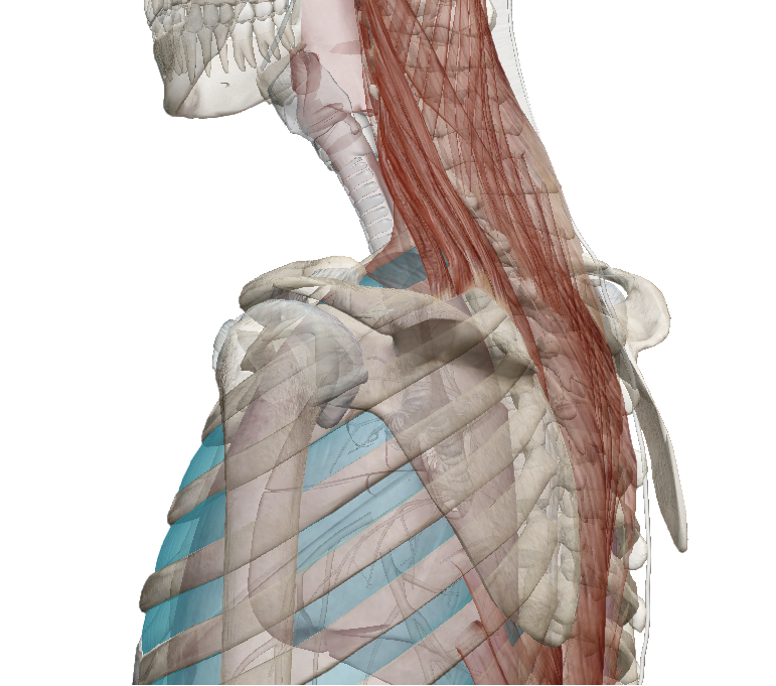
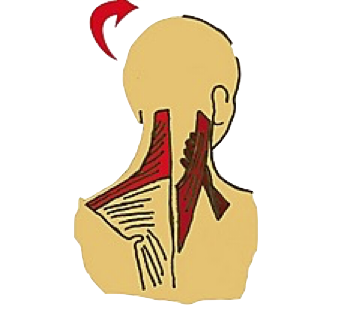
- Posterior Triangle
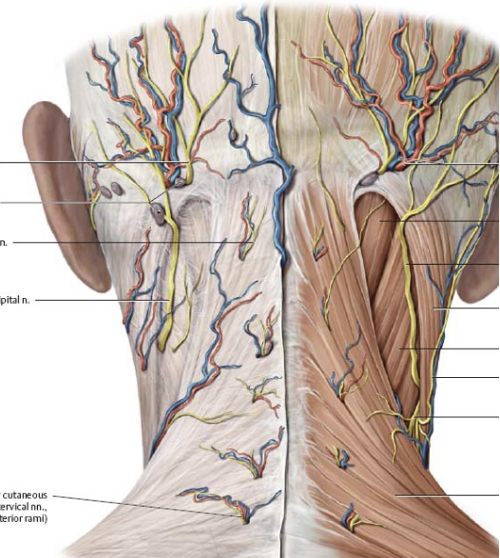
- Nerves
- Brachial plexus
- Accessory nerve
Injection Pitfalls
Brachial Plexus
Cervical Dystonia
The BP lies inferior to a line from the posterior margin of the sternomastoid at the level of the cricoid cartilage to the midpoint of the clavicle

Injection Pitfalls
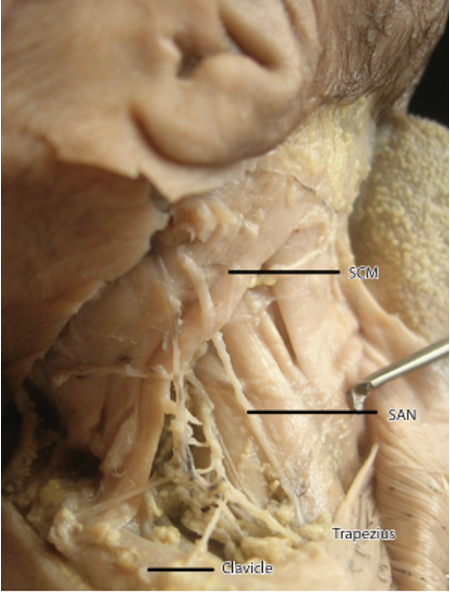
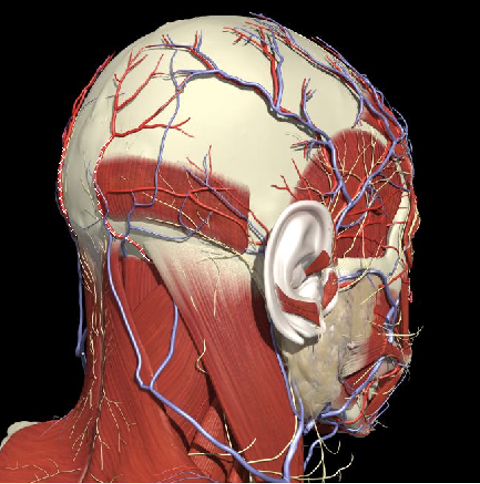
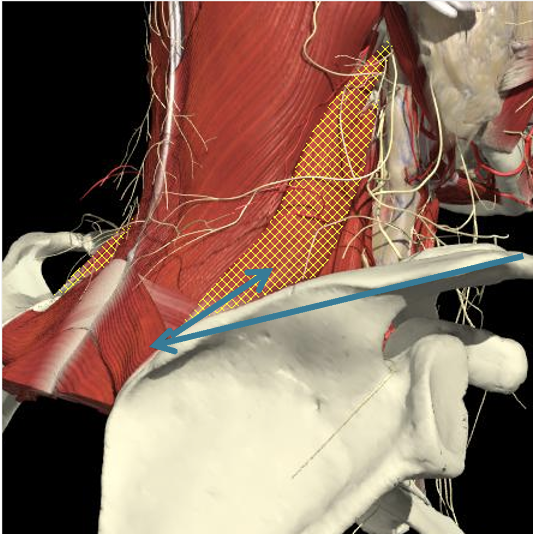
Accessory Nerve
Cervical Dystonia
-
Accessory nerve
-
Lies on LS, enters 1cm cranial to EP posterior border of SCM and runs on line to between middle and lower third of trapezius.
-

-
Should inject splenius and levator over 1cm above EP
Injection Pitfalls
Arteries
Cervical Dystonia
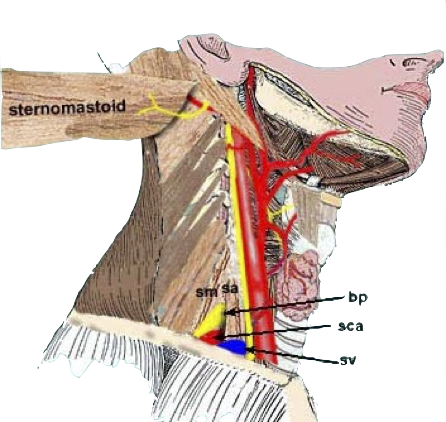
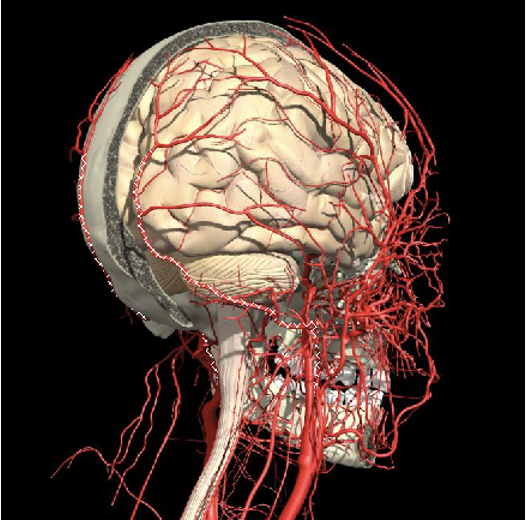
- Carotid artery
-
Midpoint anterior border of SCM
-
-
Occipital artery
-
Avoid apex of posterior triangle
-
Injection Pitfalls
Apex of the Lung
Cervical Dystonia
- Extends 2-3 cms above the clavicle
Injection Pitfalls
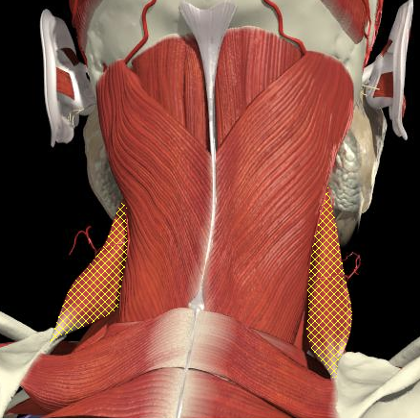
Sternocleidomastoid
Cervical Dystonia
- Stay above the midpoint of the SCM
Injection Pitfalls
Pitfalls Posterior Neck Injections
Cervical Dystonia
-
Injection of lower levator scapulae
-
Apex of lung if too deep

Injection Pitfalls
Pitfalls Posterior Neck Injections
Cervical Dystonia

Injection Pitfalls
Cervical Dystonia
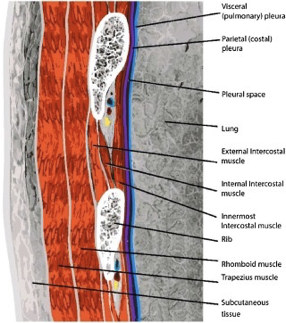
-
Layer – approximately 3cm
- SCM
-
Trapezius
-
Levator Scapulae
-
Intercostal
-
Lung
Pitfalls Posterior Neck Injections
Injection Pitfalls
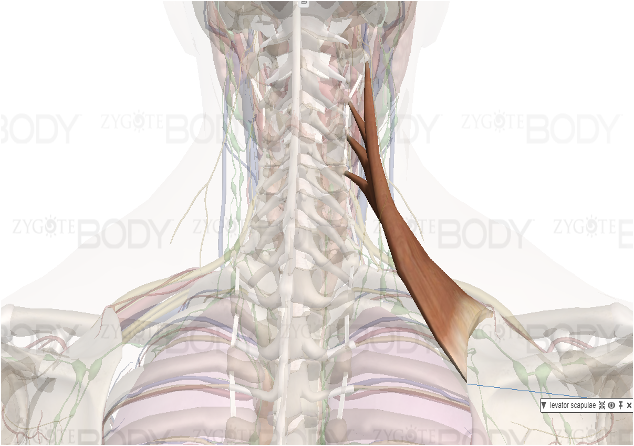
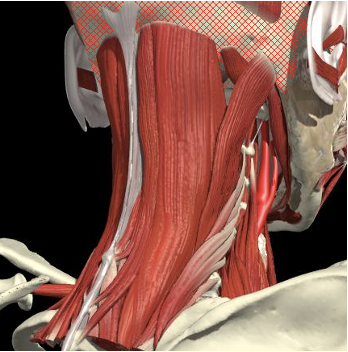
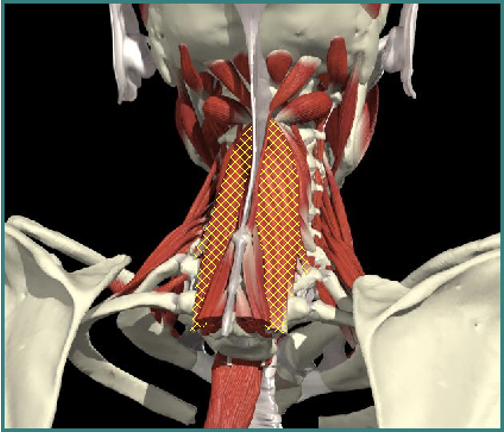
Levator Scapulae
Cervical Dystonia
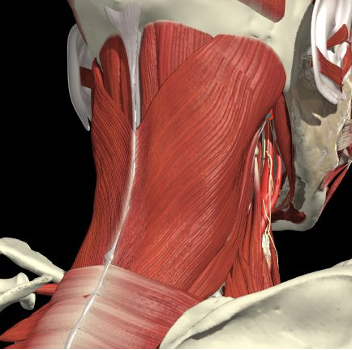
Posterior Surface Anatomy
- Line from acromium to midline and inferior
- Feel the edge of the spine
- Above and below is infra and supraspinatus fossae
- Follow spine to midline (T3 level)
- Above that along the medial border
6. Line obliquely from there to transverse process of C1-4 (below and anterior to splenius capitus)
Injection Pitfalls
Cervical Dystonia
Pitfalls Posterior Neck Injections
Arteries
- Vertebral Artery landmarks
Injection Pitfalls
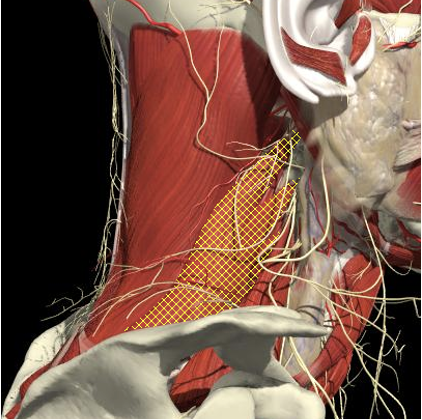
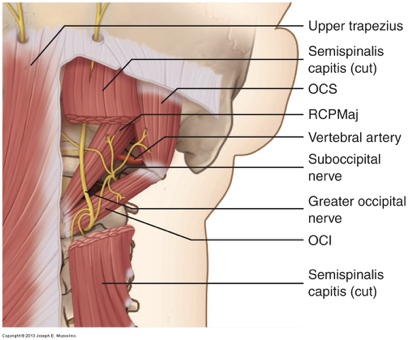
Sub-Occipital Triangle
Cervical Dystonia
Triangle between C1 transverse process (below and behind mastoid), C2 and occiput.
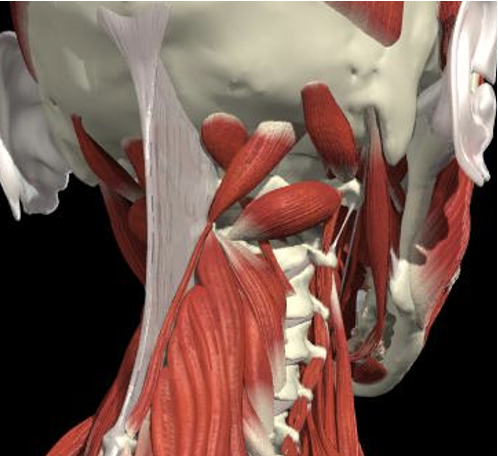
Splenius Capitis
Semispinalis
Rectus Minor Major
Obliquus Superior
Obliquus Inferior
Pass through Trapezius, Splenius capitus (more lateral) and semispinalis capitus (more medial) to reach it.
Injection Pitfalls
Posterior Injections
Cervical Dystonia
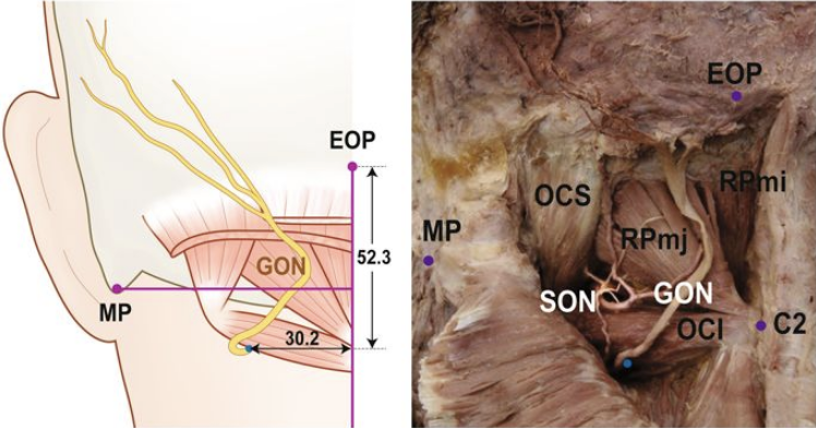
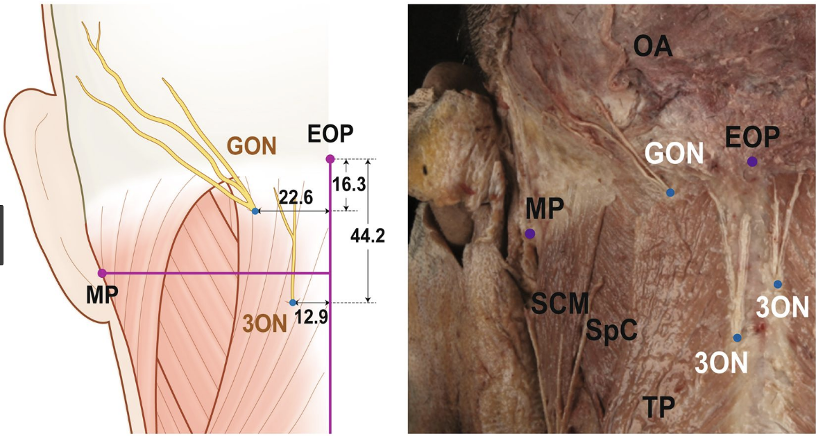
-
Greater Occipital Nerve
-
Avoid nuchal ridge near trapezius
-
Risk near OCI injections
-
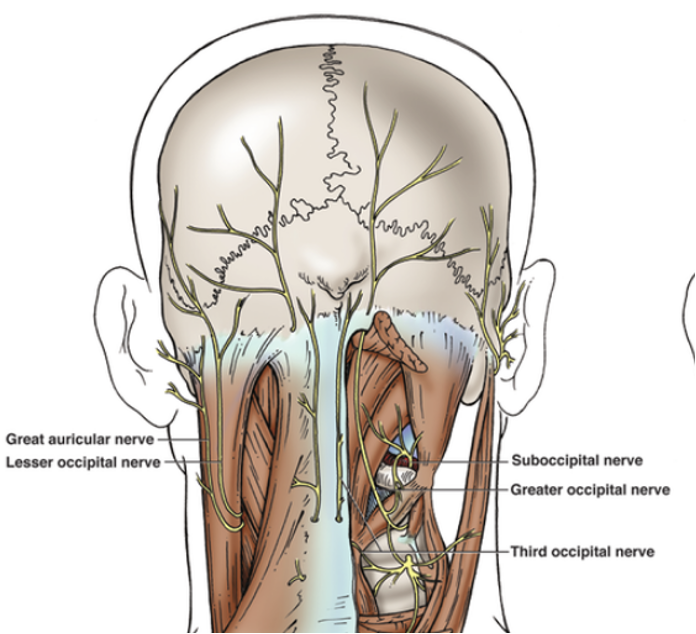
Nerves
Injection Pitfalls
Posterior Injections
Cervical Dystonia
-
Lesser Occipital Nerve
-
Arises near midpoint of SCM and runs along border
-
Avoided if stay in midline of posterior triangle
-
Nerves

Injection Pitfalls
Torticollis
Cervical Dystonia
- Attaching to skull
- Unilateral contraction

Anterolateral muscles contralateral rotation
-
Trapezius
-
SCM
Posterolateral muscles ipsilateral rotation
-
Splenius capitus
-
Longissimus capitus
-
Splenius cervicus
-
Levator Scapulae
-
Obliques Capitus inferior
Posteromedial contralateral rotation
-
Semispinalis capitis
-
Spinalis capitis

Muscles to Inject
Injection Pitfalls
Torticaput
Cervical Dystonia

Muscles attaching to skull
- Ipsilateral rotation
-
Splenius capitis
-
Splenius cervicis
-
Longissimus capitis
-
Obliquis capitis inferior
-
Levator Scapulae
-
-
Contralateral rotation
-
Trapezius
-
Sternomastoid
-
Semispinalis capitis
-
Spinalis capitis
-




Midline
Lateral

Injection Pitfalls
Torticollis
Cervical Dystonia
Muscles attached to spine
- Ipsilateral rotation
-
Longissimus cervicis
-
-
Contralateral rotation
-
Semispinalis cervicis
-
Scalenus anterior
-
Injection Pitfalls
Torticollis
Cervical Dystonia
Muscles attached to spine
-
The relevance of the SCM in some patients questionable.
-
Other muscles such as the levator scapulae and the obliquus capitis inferior muscles have attained key status.
-
Guided by size of muscle and EMG involvement in movement
-
Generally does not require high dose (note risk of dysphagia)
-
NB: Endplate position, fibre type and spindle numbers (more Type 2 – lower dose needed)
Injection Pitfalls
Dressler 2000
Cervical Dystonia

-
10 patients clinical and EMG recordings
-
6 patients had discrepancies between EMG and clinical assessment
-
All were for SCM
Injection Pitfalls
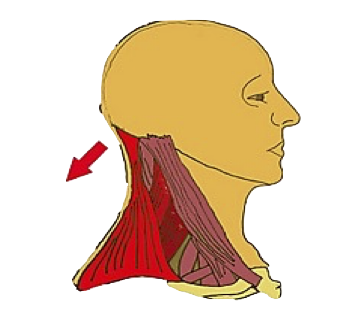
Sternomastoid
Cervical Dystonia
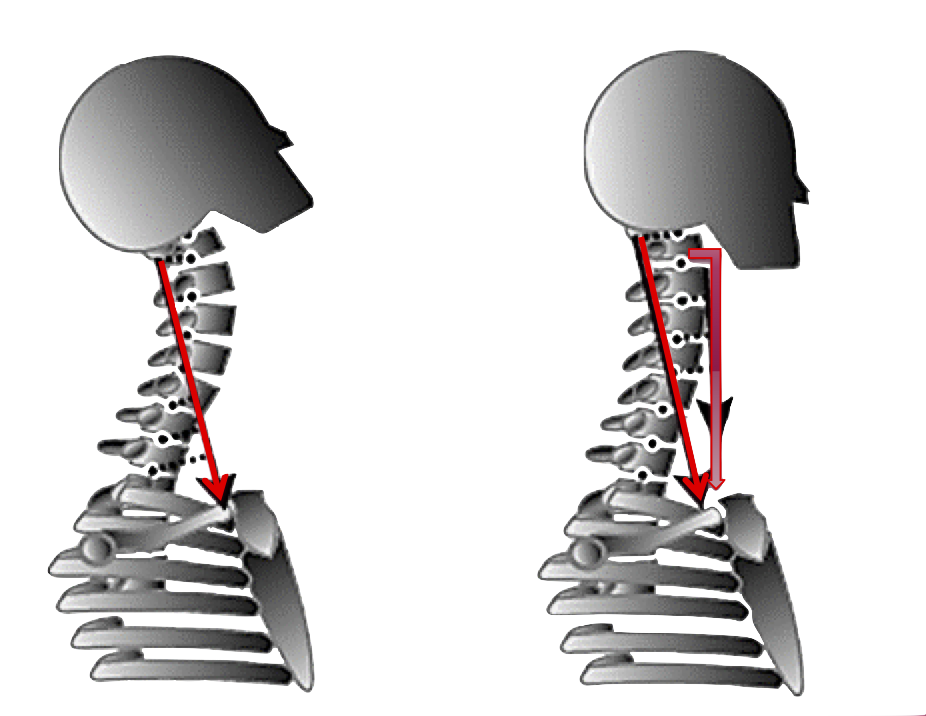
Extends the head and flexes neck when longus colli relaxed
Flexes head and cervical spine if deep flexors [longus colli] are contracted
Unique Action
Injection Pitfalls
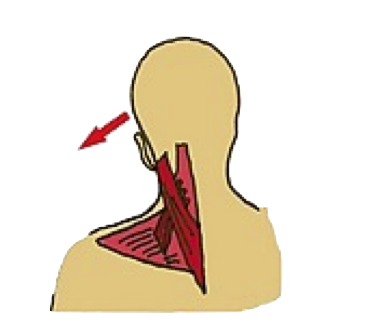
Levator Scapulae & Neck Motion
Cervical Dystonia
Left Lateral Flexion
Left U Trapezius, SCapitus and Levator Scapulae
Left U Trapezius,
Right SCapitus , Levator Scapulae
Bilateral U Trapezius
Scapitus, Levator Scapulae
Right Rotation
Extension
Injection Pitfalls
Cervical Dystonia
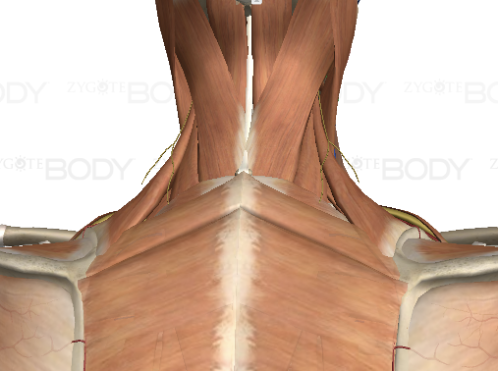
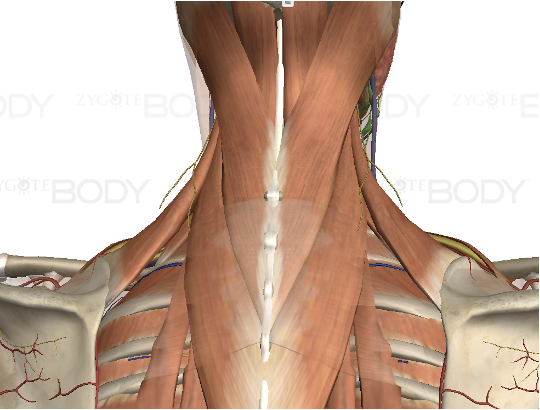
Relationship between SCM,Trapezius, Splenius and Levator Scapulae in Torticollis
Torticollis
-
Synergy between contralateral sternocleidomastoid and contralateral trapezius, and between ipsilateral levator scapulae and ipsilateral splenius for rotation.
-
Shoulder elevation on the side of rotation therefore suggests dystonic levator scapulae
-
Shoulder elevation on the opposite side of rotation suggests dystonic trapezius
-
Injection Pitfalls
Hemifacial Spasm
Injection Pitfalls
Hemifacial Spasm
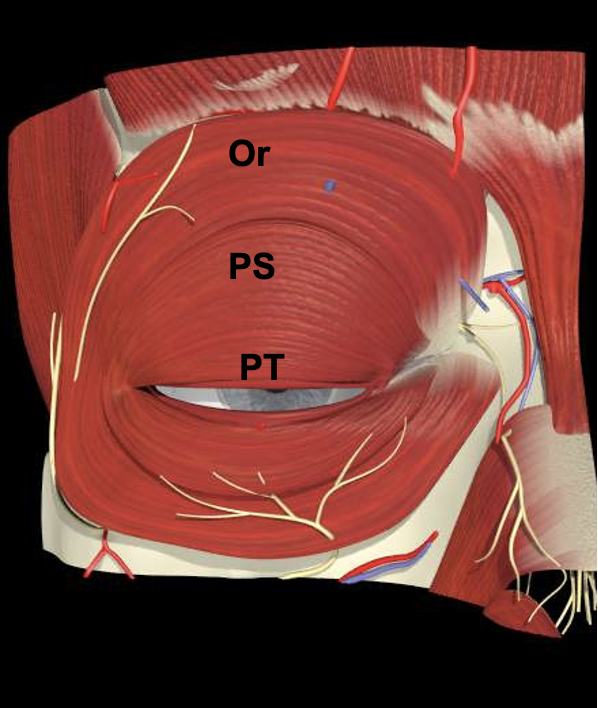
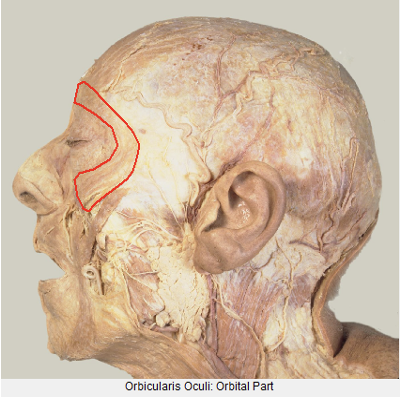
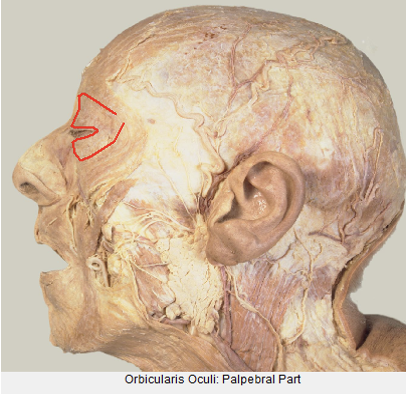
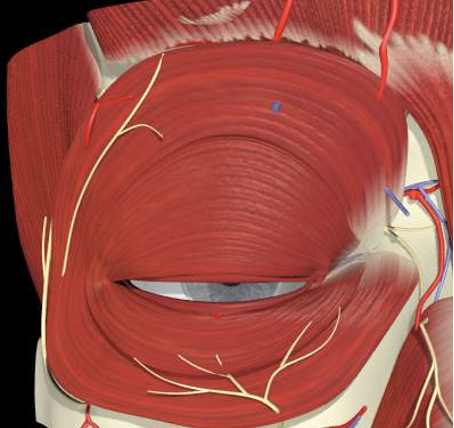
Orbicularis Oculi Function
Role of Pretarsal Injections
-
Orbital portion closes the lids, drawing the skin of the forehead, temple and cheek medially.
-
The palpebral portion of orbicularis closes the lids grossly, but incompletely, for long periods of time.
-
Located next to the lid margin the pretarsal and Riolan’s muscle, provides closure for brief periods of time, as in reflex or involuntary blinking.
-
Horner’s tensor tarsi encircles canaliculi to facilitate tear drainage
Injection Pitfalls
Hemifacial Spasm
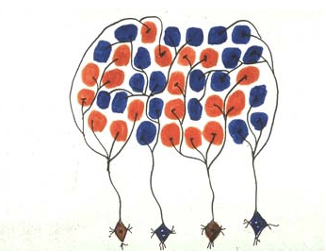
Functional Anatomy
-
Differences in fibre cross-sectional areas and in fibre type.
-
At increasing distances from the eyelid margin there is a gradual increase in fiber cross-sectional area and in the proportion of type I fibres (slow-twitch).
-
-
-
The pretarsal region including Riolans muscle is almost 100% type 2 fibers (fast twitch).
-
-
-
Fibres in the preseptal region contain between 8% and 15% type I fibers
-
Injection Pitfalls
Hemifacial Spasm
Functional Anatomy
-
The differences may reflect the activity and function of the orbicularis oculi during eye blink and forceful eyelid contraction i.e fast twitch and slow twitch.
-
Experimental work on rat calf muscles showed that the recovery of type I muscle fibres from botulinum toxin is much faster than that of type II fibres (Hassan SM et al Muscle and Nerve 1994)
Injection Pitfalls
Hemifacial Spasm
Injection Technique
Role of Pretarsal Injections
-
Cakmur etal 2002 J Neurol
-
53 patients (25 blepharospasm, 28 hemifacial spasm).
-
PT higher response rate and longer duration of action.
-
PT less ptosis more blurred vision.
-
-
Other comparative studies Albenese etal 1996, Aramideh et al 1995, Jankovic 1996, Kowal 1997 have found similar results.
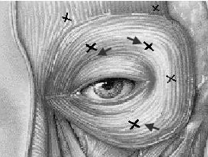
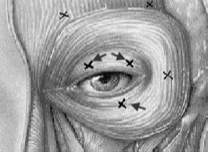
Pre Septal
Pre Tarsal
Injection Pitfalls
Hemifacial Spasm
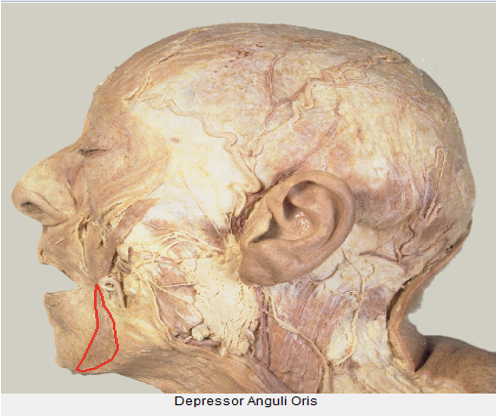
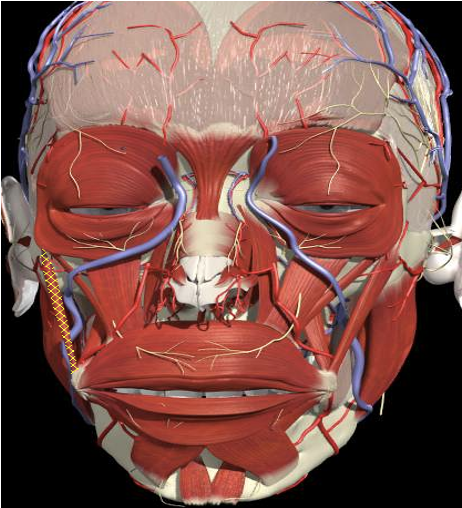
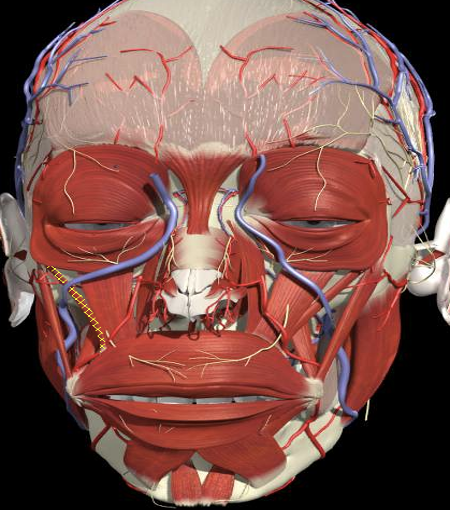
Lower Face Muscle Overlap
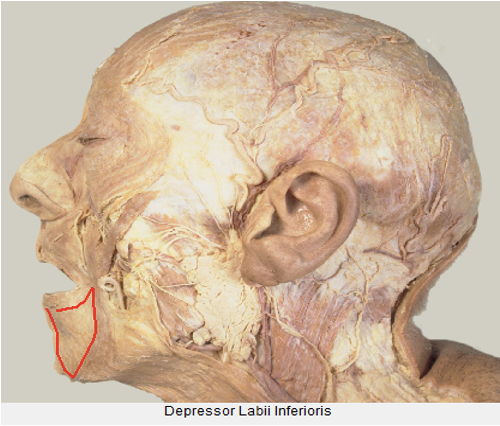
DLI
DAO
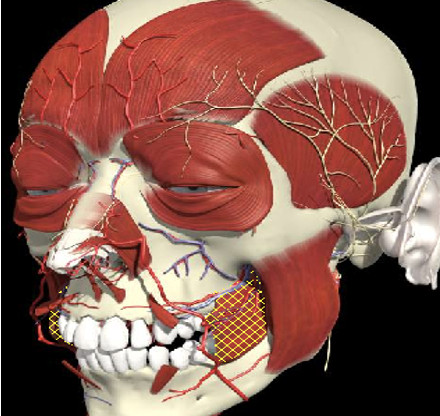
BUC
RIS
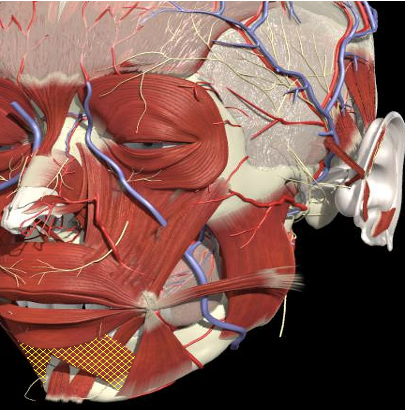
Injection Pitfalls
Hemifacial Spasm
Lower Face Muscle Overlap


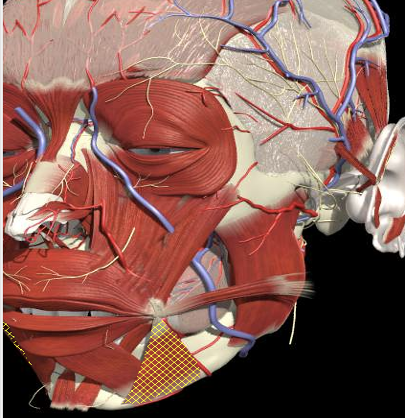
Injection Pitfalls
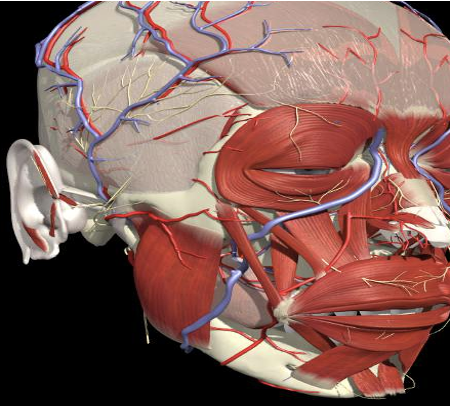
Hemifacial Spasm
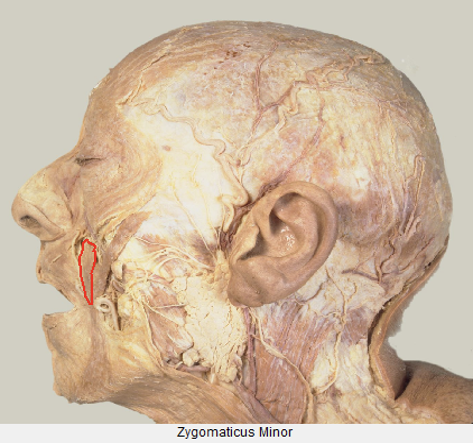
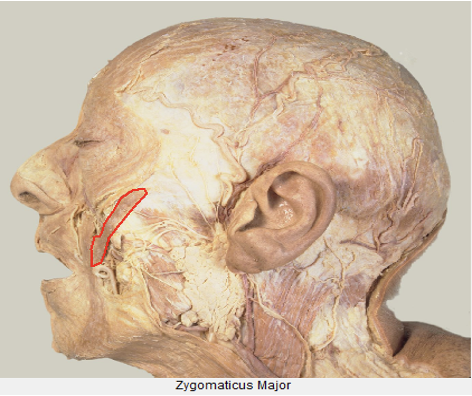
Upper Face Muscle Overlap
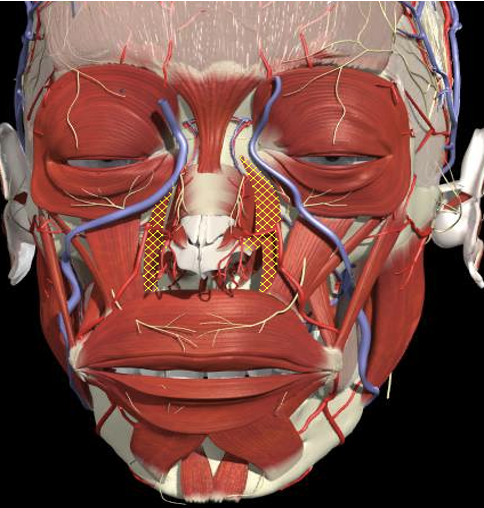
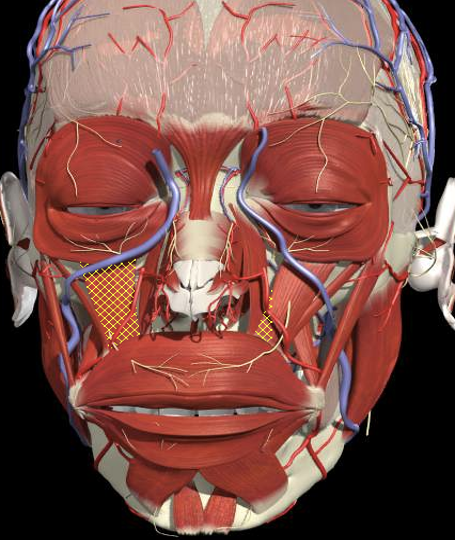
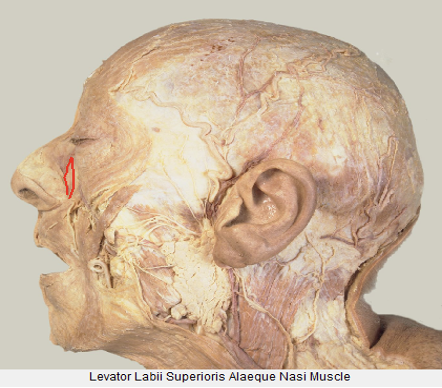
Levator Labii Superioris
Alequa Nasi
Levator Anguli Oris
Zygomaticus Major
Zygomaticus Minor
Levator Labii Superioris
Injection Pitfalls
Hemifacial Spasm
Upper Face Muscle Overlap
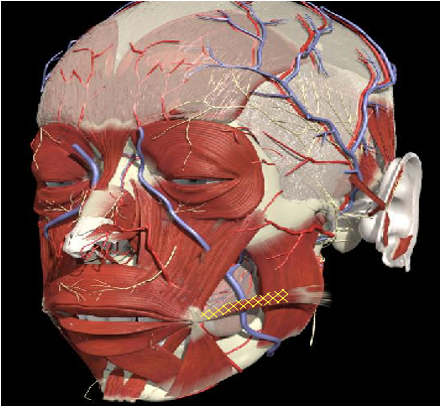
Injection Pitfalls
Hemifacial Spasm
Injection Technique
Muscle Overlap
-
Pitfalls with O Oculi injections
-
Dropping angle of mouth
(lower lateral injection) -
Nasolabial fold
-
Inability to elevate upper lip
(lower medial injection)
-

Injection Pitfalls
Hemifacial Spasm
Injection Technique
Muscle Overlap
-
Pitfalls with O Oculi injections
-
Dropping angle of mouth
(lower lateral injection) -
Nasolabial fold
-
Inability to elevate upper lip
(lower medial injection)
-
Injection Pitfalls
Hemifacial Spasm
Injection Technique
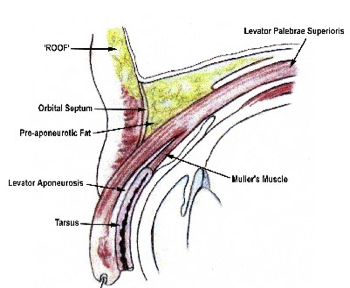
Facial Spasm - Pitfalls Ptosis
-
Ptosis
-
Levator palpebrae becomes aponeurotic already at the level of the superior transverse ligament 14 to 20 mm above the tarsus. Preseptal injections closer
-

Injection Pitfalls
Hemifacial Spasm
Physiological Principles
Spindles
-
Muscle spindle block can lead to increased atrophy and changes in function- location and number differs between muscles
-
Important in terms of pain and maintenance of tone and control of posture and fine movements
-
Neck has greater number than shoulders
-
Proximal greater than distal in UL
-
Masseter and deep neck muscles (part OCI) have much higher spindle concentration than lateral muscles such as splenius
Injection Pitfalls
Hemifacial Spasm
Physiological Principles
Capacity to Sprout
-
Muscle spindle block can lead to increased atrophy and changes in function - location and number differs between muscles
-
SC cells affected by age
-
Capacity to regenerate after botulinum toxin injections will be affected by these factors
-
Motor axon length - Proximal greater capacity than distal
Injection Pitfalls
Hemifacial Spasm
Physiological Principles
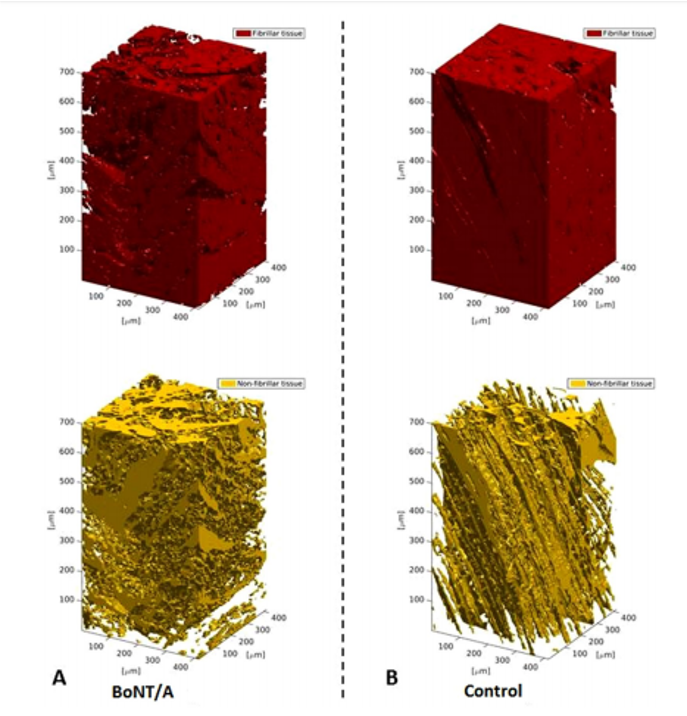
Fibre Type
-
Type I fibers tend to develop early, multiple sprouting, compared to type IIb fibers after BoTx
-
Toxin dose and frequency of injections could be adjusted when injecting muscles that have predominantly type IIb fibers in order to lessen atrophy in susceptible patients
-
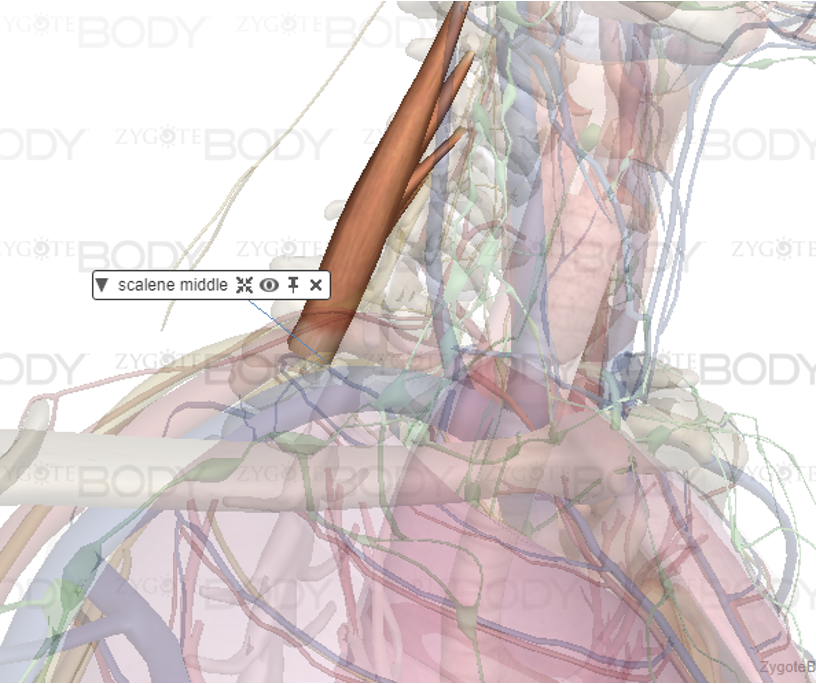
Muscles such as vastus lateralis and sternocleidomastoid (SCM) have a lower proportion of type I fibers and a higher proportion of type IIb fibers compared to splenius capitis, trapezius, and scalenus medius.
Injection Pitfalls
Hemifacial Spasm
Physiological Principles
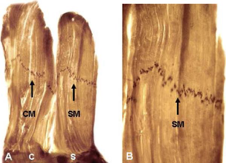
Endplate Location
-
The importance of targeting the motor endplate has been emphasized in animal models.
-
Using rat anterior tibialis muscle, Shaari and Sanders demonstrated that toxin injection into the motor endplate region produces the greatest paralysis. Injections only 0.5 cm away from the region resulted in a 50% decrease in paralysis.
-
In a canine model, placement of BTX at the motor endplate potentiated the toxic effect and decreased muscle force generation.
-
Injection Pitfalls
Hemifacial Spasm
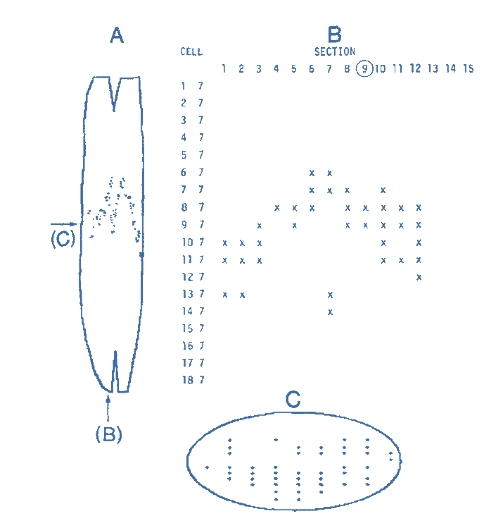
Endplate Injections
Rat Anterior Tibialis
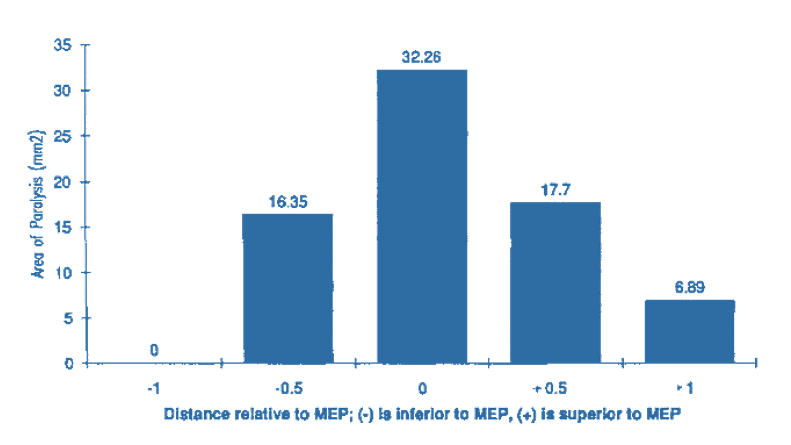

Normal
1 cm

MEP
0.5 cm
Injection Pitfalls
Hemifacial Spasm
Diffusion and End Plates
-
BTX diffuses outside of target muscles.
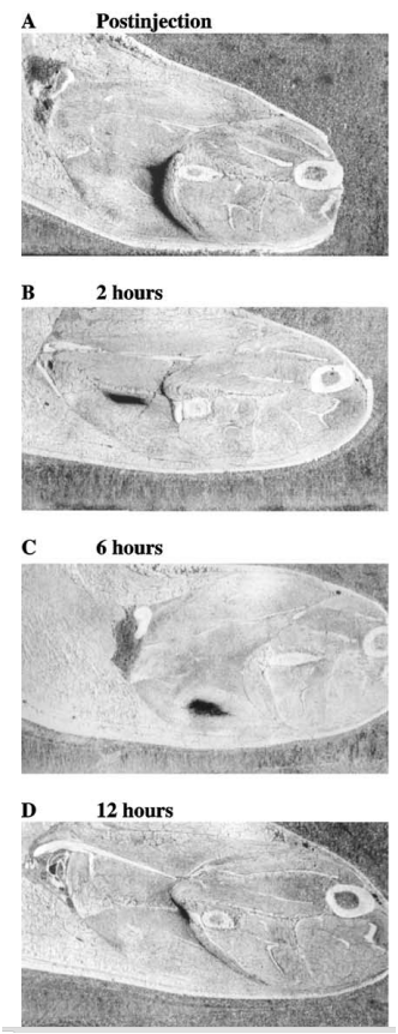
-
Spread is estimated to be 2.5–4.5 cm, with the size of the diffusion field being proportional to the amount of toxin delivered.
-
Can occur across fascial planes. Weaken non dystonic muscles
-
Series of patients with upper limb dystonia, weakness of uninjected muscles adjacent to those injected was found in 63% of patients.
-
The closer you are to endplate the less diffusion to inappropriate muscles occurs.
Injection Pitfalls
Hemifacial Spasm
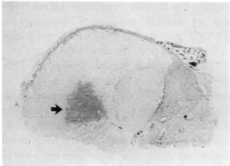
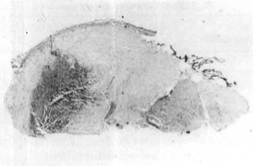
Distribution of End Plates
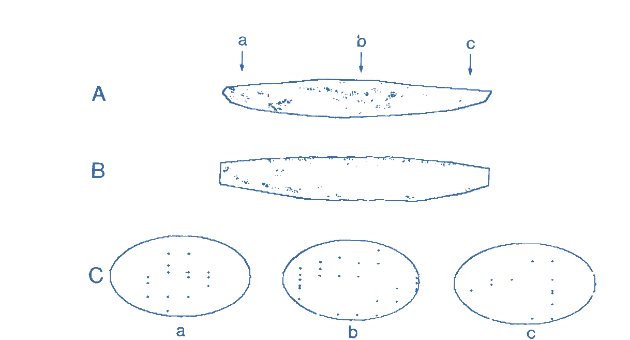
Tibialis Anterior
Biceps
Injection Pitfalls
Hemifacial Spasm
The studies in humans have shown that the spindle density is in general highest in hand, foot and neck muscles, lowest in the shoulder and thigh muscles and intermediate in the more distal muscles of the arm and the leg (Voss, 1971). The spindle density can be regarded as an indicator of functional differences between muscles. In general, high spindle density characterizes muscles initiating fine movements (e.g. lumbrical muscles) or maintaining posture (e.g. neck muscles) whereas low spindle density is characteristic of muscles initiating gross movements (e.g. biceps brachii).
The deep neck muscles have an unusually high muscle spindle density which is nearly five times higher than that of the large splenius capitis and three times that of the semispinalis capitis muscle (Cooper and Daniel, 1963; Kulkarni et al., 2001; Peck et al., 1984; Voss, 1971). In adults, the spindle density is about 30.0 in both the rectus capitis posterior major and the obliquus capitis inferior; 36.0 in the rectus capitis posterior minor and 40~43 in the obliquus capitis superior (Peck et al., 1984; Voss, 1971). The convergence of sensory afferents from deep neck muscles with vestibular and ocular inputs at various levels of the neuroaxis is well recognized (Cooper and Daniel, 1963; Kulkarni et al., 2001; Richmond and Abrahams, 1975, 1979a). The complex integrative mechanisms involved in head positioning in relation to vestibular and visual control probably demand finely tuned proprioceptive inputs from the deep neck muscles, therefore requiring such a high spindle density.
Injection Pitfalls
Hemifacial Spasm
CD & HFS_Injection Pitfalls
By Integra


