CLINICAL ASSESSMENT OF CERVICAL DYSTONIA
Professor Con Yiannikas
Assessment
Cervical Dystonia
- This can be done with the patient seated but assessment should also be done
-
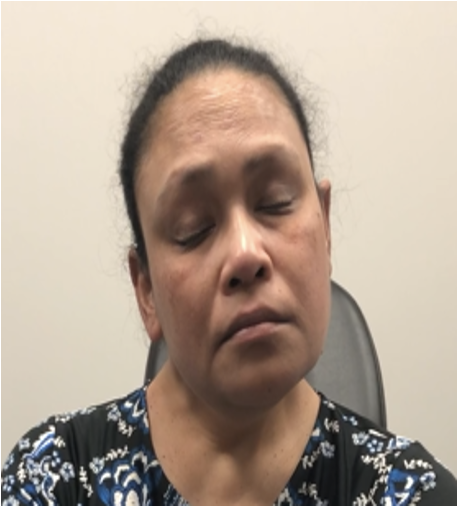
With eyes closed and open
-
Following repetitive voluntary movements to look for overflow, writing, typing, drinking
-
Walking and laying down
-
Clinical Assessment
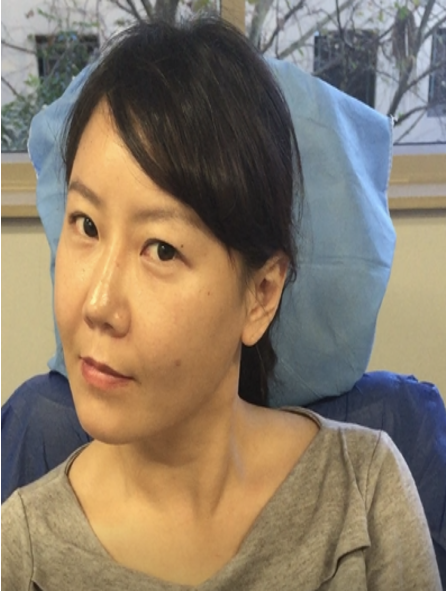
Analyse Posture
Assessment
Cervical Dystonia
-
From behind – best position for shoulder assessment and tilt
-
If possible from top – good for assessing rotation
Clinical Assessment
-
The patient may adopt a compensatory posture in opposition to the dystonic spasm, which can be misleading

Assessment
Cervical Dystonia
-
Palpation for muscle soreness or hypertrophy
Clinical Assessment
-
In the presence of tremor look for “null position”
-
Localise pain - although may also be occurring in muscles opposing spasm
Assessment
Cervical Dystonia
Clinical Assessment
-
Examine the shoulder muscles, looking for elevation of one shoulder, comparing the position of the scapulae.

-
Examine for trunk rotation.
-
Patients often have a mixed pattern of cervical dystonia.
Clinical Clues
Cervical Dystonia
Clinical Assessment
Degree of Movement
Clinical Clues
Cervical Dystonia
Clinical Assessment
Head Tilt
- The degree of tilt helps in the assessment of laterocaput versus collis
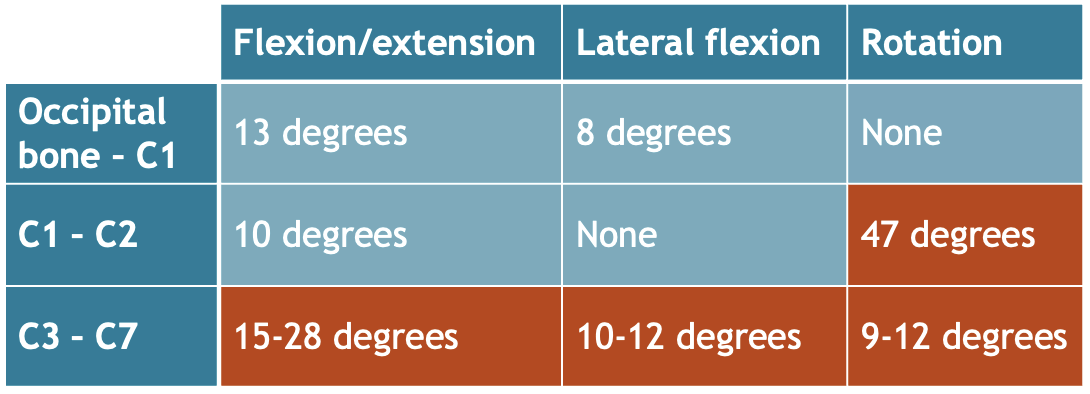
- Lateral flexion of head is at Occ-C1- maximum movement at this joint is 10 degrees
Clinical Clues
Cervical Dystonia
Clinical Assessment
Head Tilt
Movement between C2-C6 is up to 37 degrees so likely to be laterocollis and involve long spine to spine muscles

Clinical Clues
Cervical Dystonia
Clinical Assessment
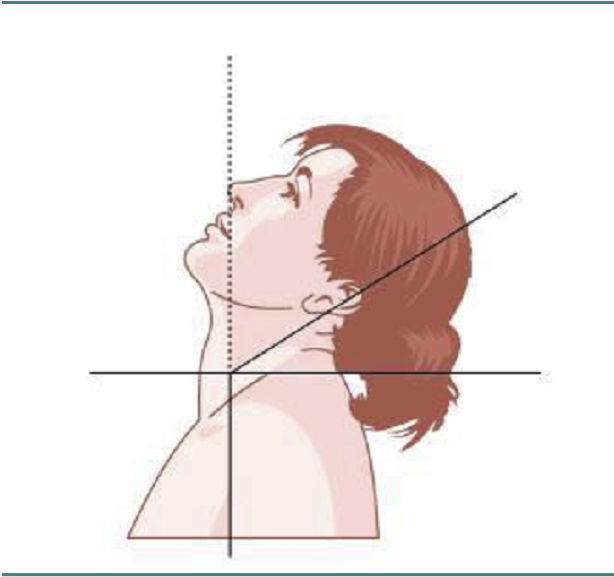
Extension
Maximum Extension C2-7 is up to 66 degrees so likely to be retrocollis

Clinical Clues
Cervical Dystonia
Clinical Assessment
Extension

Movement between Occiput and C1 up to 13 degrees so most likely retrocaput
Clinical Clues
Cervical Dystonia
Clinical Assessment
Rotation
- Shoulder elevation on the side of rotation therefore suggesting dystonic levator scapulae
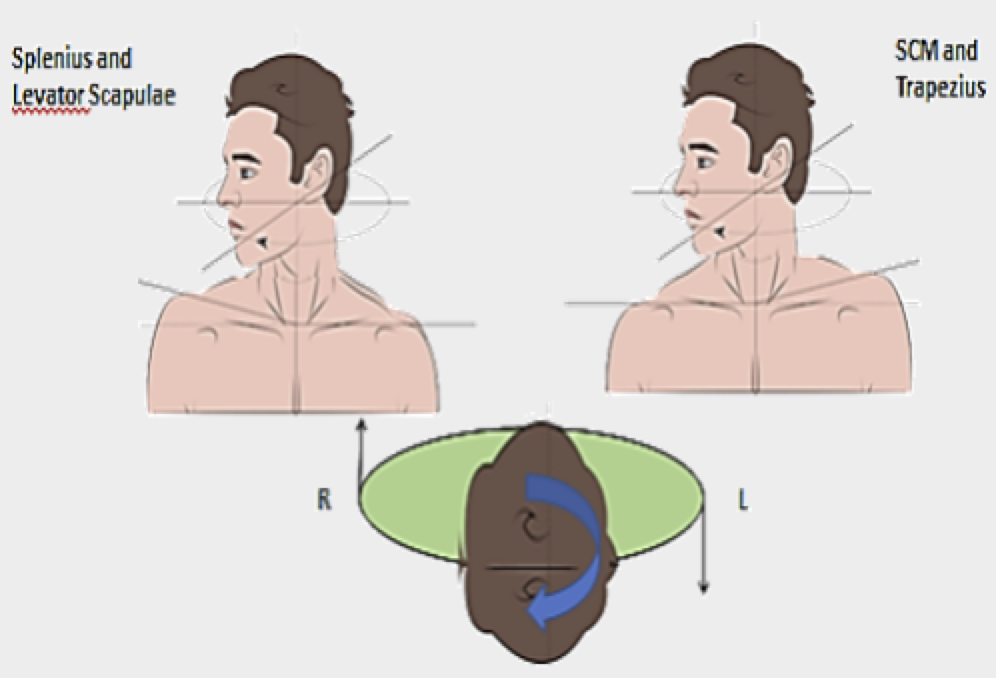
- Shoulder elevation on the opposite side of rotation suggests dystonic trapezius
Clinical Clues
Cervical Dystonia
Clinical Assessment
Rotation

Clinical Clues
Cervical Dystonia
Clinical Assessment
Rotation
Identical muscle fibre orientation explains the synergy of action in the rotation of the head between sternocleidomastoid and trapezius and between splenius and levator scapulae


Clinical Clues
Cervical Dystonia
Clinical Assessment
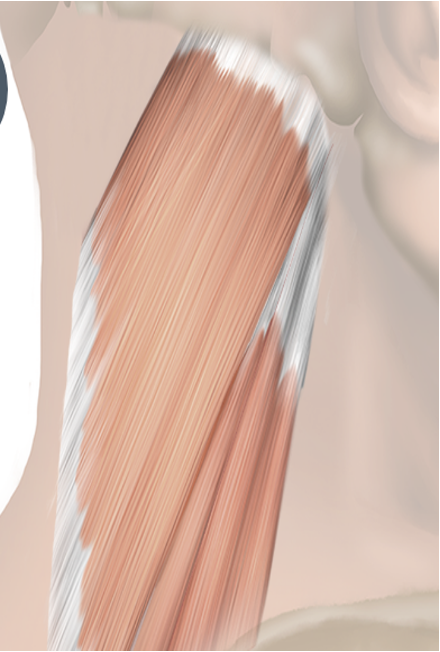
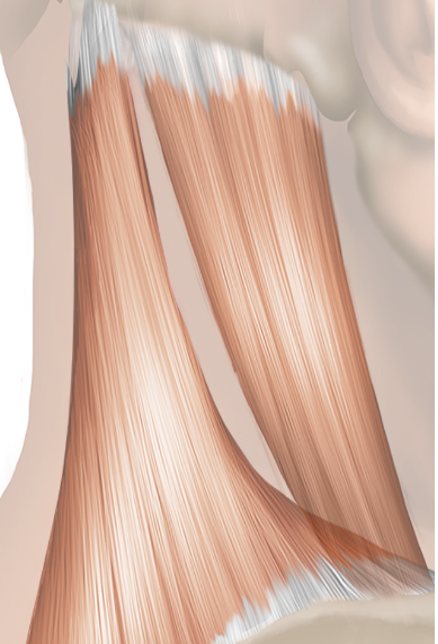
SCM
- Overinjected - not always involved in rotation or flexion

Sternal
Clavicular Head
- Sternal head rotates
- Clavicular head tilts
Clinical Clues
Cervical Dystonia
Clinical Assessment
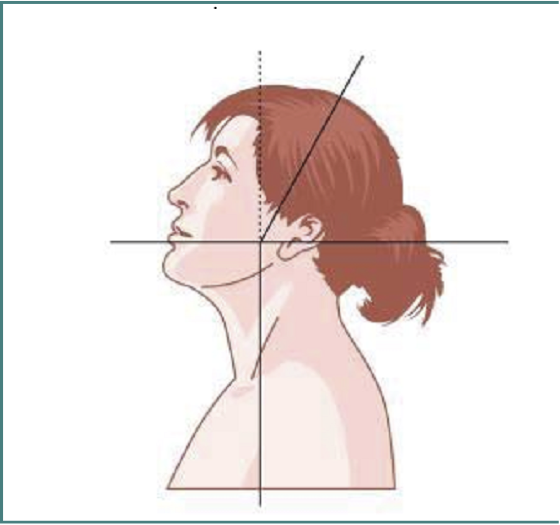
Determination of Axis
Head versus Spin
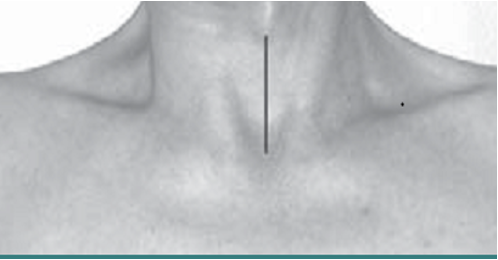
Line from Thyroid cartilage to sternum
Head to left and neck to the right - lateral shift
Sensory Tricks
Cervical Dystonia
Clinical Assessment
-
Touching specific parts of the face, cheek, chin, occipital region, temple, forehead, nose, mastoid, occipital region, back of neck
-
Raising the arm and holding the finger near the target region without touching the face or prior to touching the face
-
Resting the back of the head or neck, bending the trunk forward, resting the back or shoulder, yawning, wearing a collar/a scarf, leaning the elbows on the armrest
CD_Clinical Assessment
By Integra


