Features of Resolving and Nonresolving Indeterminate Pulmonary Nodules at Follow-up CT: The NELSON Study
Zhao YR, Marjolein AH, et. al.
Journal club 6/3/2014
Background
- 66% of participants in CT screening trials have at least 1 pulmonary nodule
- Most indeterminate nodules benign
- granulomatous or infectious lesions
- benign lymph nodes
- Purpose: to retrospectively identify features allowing prediction of disappearance of solid, indeterminate intraparenchymal nodules
The NELSON Study
Nodule management based on volume and volume doubling time
Population
- 7557 participants
- 46-76 years old (mean age 59)
- high risk for lung cancer
- current or former smokers
- > 15 pack years
CT protocol
- 1.0 mm slice thickness, low dose
- baseline, 1 year, 3 years
- If indeterminate nodule found,
followup scan at 3 months
-
No growth or < 25% growth:
- regular screening
- > 25% growth or volume doubling time < 400 days:
- referred for further workup
Image Reading
- Read twice independently
- 1st by one of 13 radiologists 1-20 yrs experience
- 2nd by one of 2 radiologists at least 6 yrs experience
- If discrepancy
- 3rd radiologist > 15 yrs experience arbitrated
Discrepancies between 1st and 2nd reading found in 43 lesions
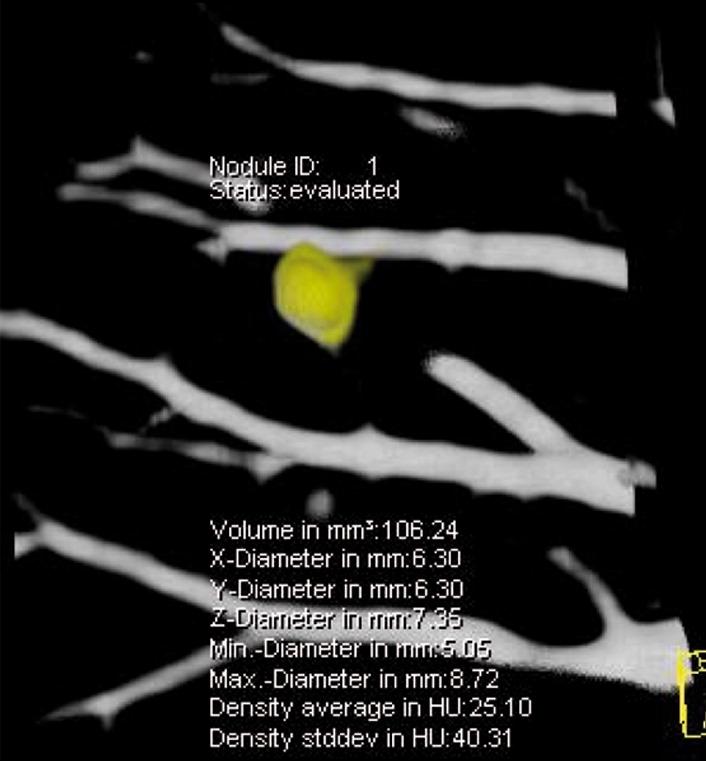
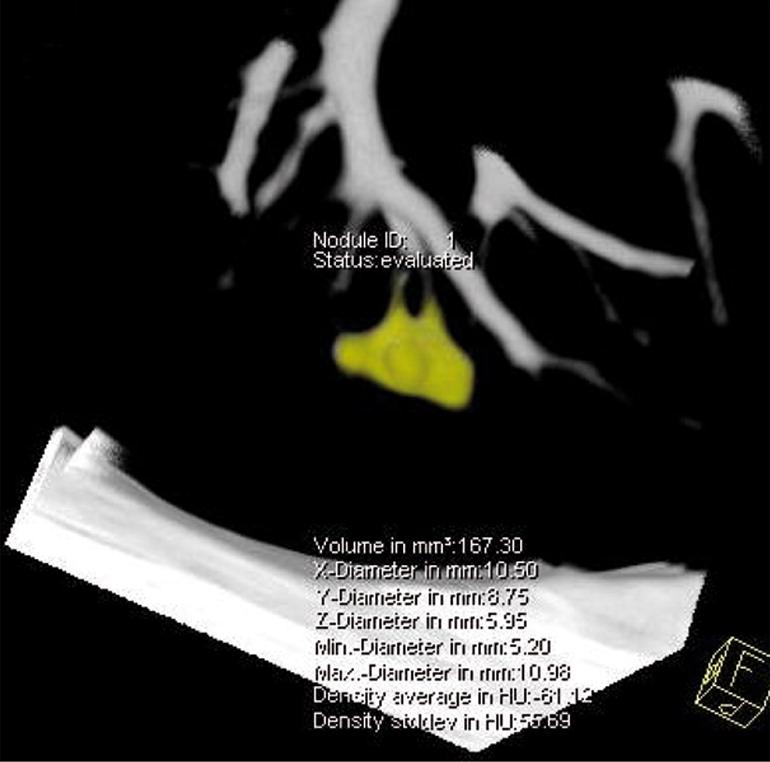
Volume calculation
- Syngo Lungcare software package
- 3D template generated after clicking nodule with automated volume measurements
- In 86% of >4000 nodules, double reading gave same volume
- Differences >15% found in 4% of nodules
- If volumes differed, 2nd reader measurements used
Nodule characteristics
- Indeterminate size:
- 50 - 500 mm^3 (4.6 - 9.8 mm)
- Considered benign if no growth after 2 years
or benign histology - Considered resolved if disappeared on followup CT
- Peripheral defined as outer 1/3 of lung
- Margins defined as smooth vs.
non-smooth (lobulated, irregular, spiculated)
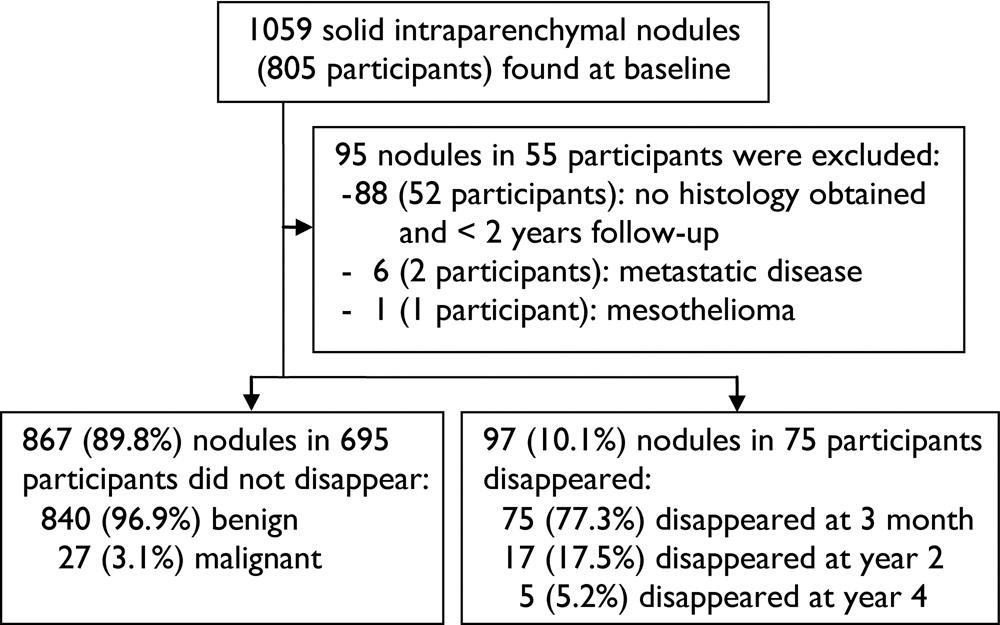
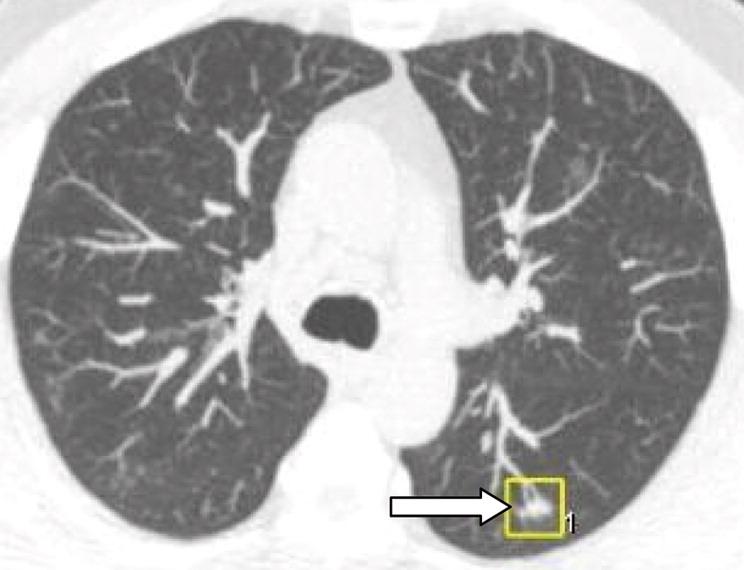
Results: Figure 1
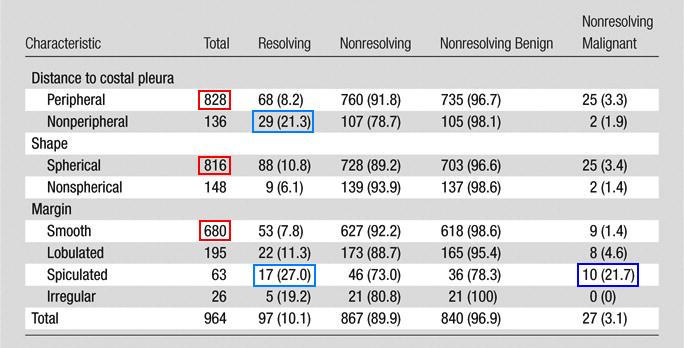
Results: Table 1
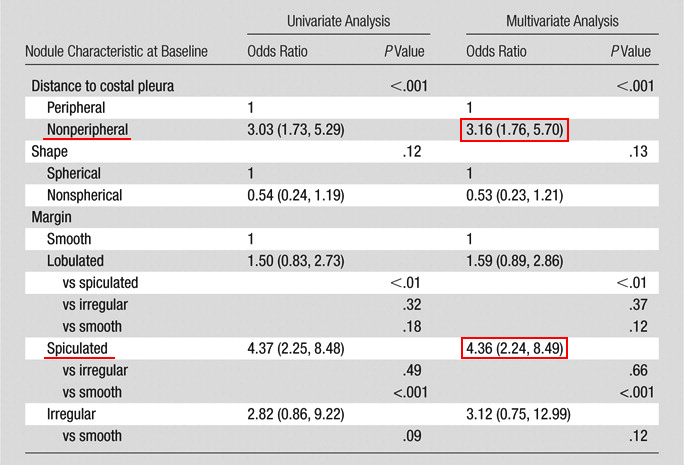
Results: Table 2
Results: Table 3
Nodule resolution by size

Results: Table 4
Moment of resolution by nodule size

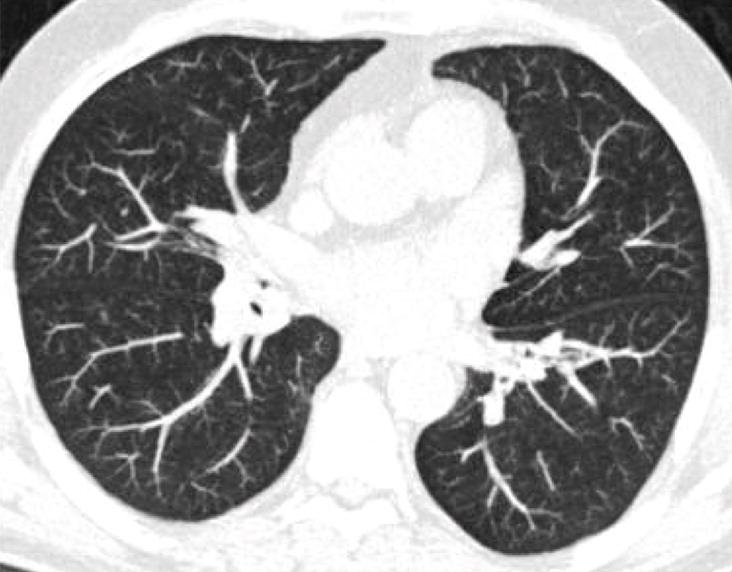
Results: Figure 2 (smooth, round)
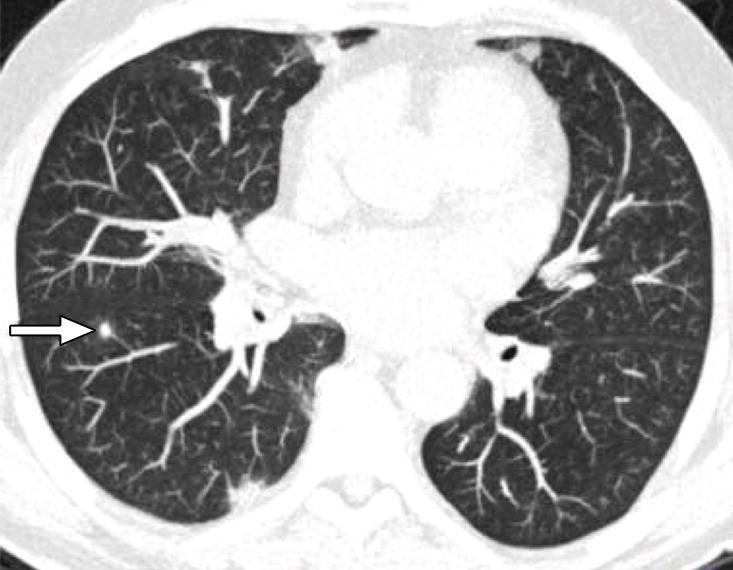
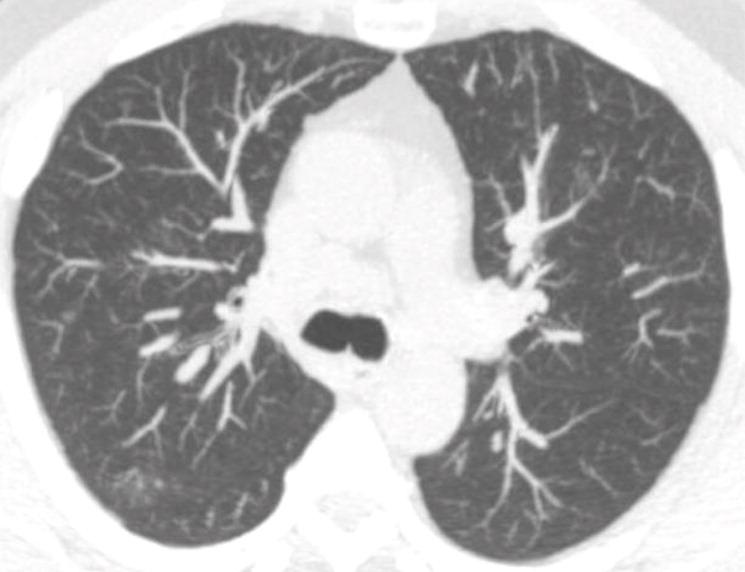
Results: Figure 2 (lobulated)
Discussion
In NELSON, 10.7% of participants had solid, intraparenchymal nodule with volume 50-500 mm^3
10.1% disappeared at followup
Though most do not resolve, 75% of those that do resolve can be identified at 3-month repeat CT
Discussion
Nodules with non-smooth edges disappeared more frequently than those with smooth edges
However, non-smooth edges also more frequently found in malignant nodules
No distinction can be made between resolving and nonresolving malignant nodules based on nodule edge
Discussion
The rate and speed of disappearance higher for larger nodules (>= 8 mm)
However, rate of malignancy also higher
May be explained by benign conditions like inflammation commonly showing nodules with a larger diameter
Limitations
Precise time of nodule resolution could not be ascertained
No histology for resolving nodules
Generalizability to incidental nodules found on non-screening exams
Conclusions
About 10% of solid intraparenchymal nodules of intermediate size resolve during followup
Short term followup CT valuable for detecting fast-growing nodules and for identifying 3/4 of resolving nodules
Resolving pulmonary nodules share CT features with malignant nodules.
Journal club 6/3/2014
By Jason Hostetter



