Chest Pain
in Primary Care
Chandni R. Nijjar
PGY2 FM
- Clinical scenarios
- History
- Physical Examination
- Life Threatening Conditions
- Differential Diagnosis
- Management of common causes
- SAMP questions
Outline
Common causes
1. Chest wall pain (20-50%)
2. Gastroesophageal reflux (10-20%)
3. Costochondritis (13%)
4. Cardiac (1%)
Chest pain on and off since 2 weeks.
Age: 47
Gender: F
Name: Suzan
Status: HTN, DM with dyslipidemia
Age: 28
Gender: F
Name: Carol
Status: Healthy
Complaint
👀
1. Demographic: Male, Elderly, risk factors for CAD.
2. Currently experiencing chest pain, SOB or lightheadedness
3. Patient looks quite unwell, diaphoretic or has unstable vitals
4. Special Populations
2. Past Medical history
3. Family History
4. Social History
History
1. HPI
1. Onset and Duration
2. Position
3. Quality
4. Severity
5. Aggravating and Relieving factors
6. Timing
7. Associated symptoms
1. HPI
8. Cardiac risk factors
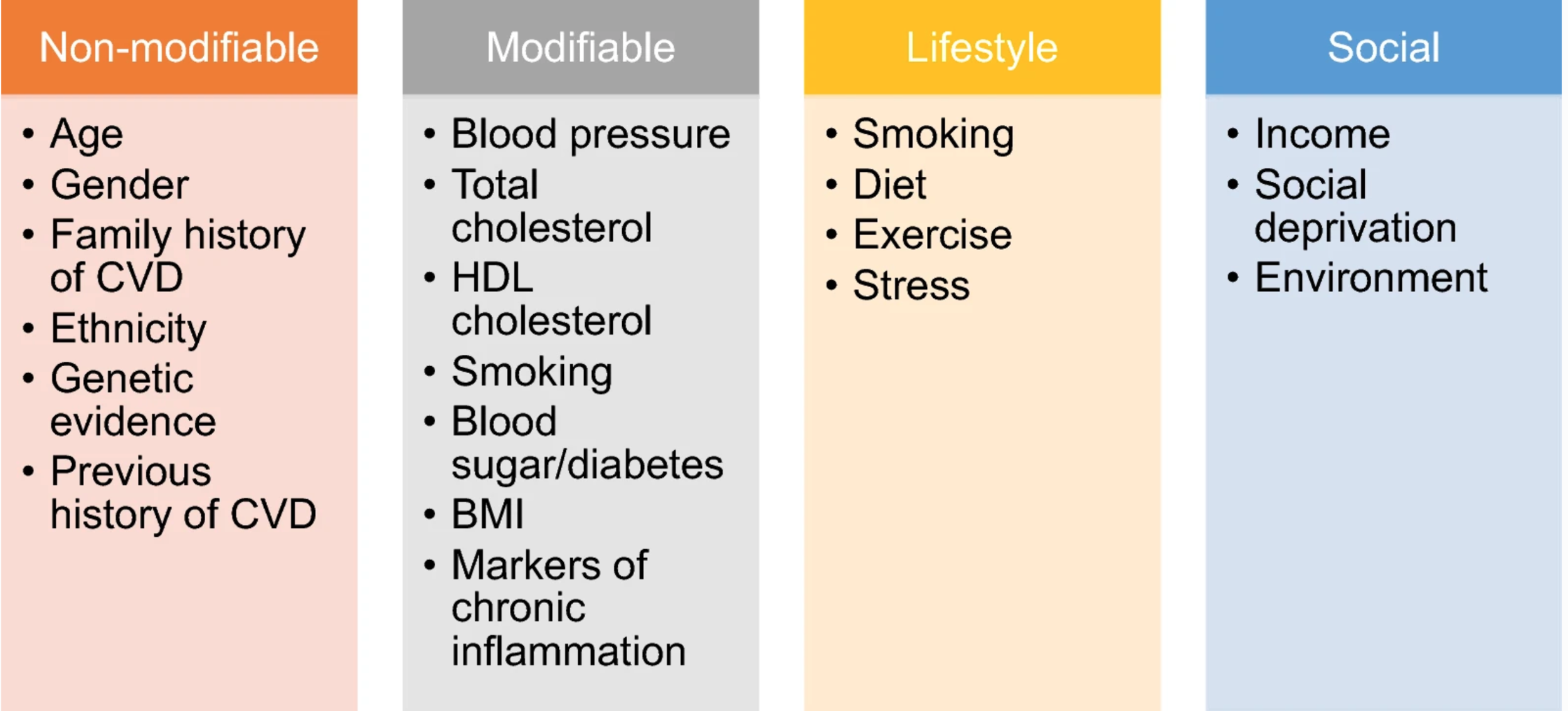
8. Cardiac risk factors
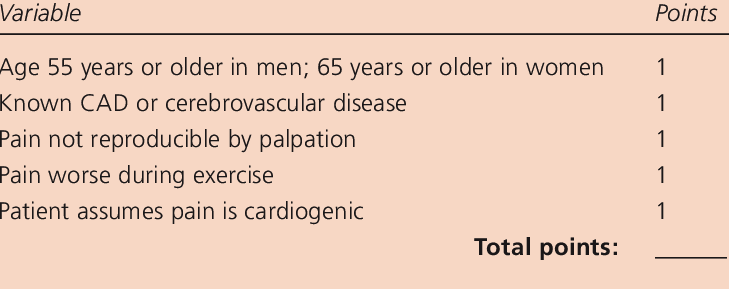
Clinical Decision making rule: CAD
1. Vitals: Including BP in both arms
2. Inspection and palpation of the precordium
3. Cardiovascular exam
4. Respiratory exam
5. Abdominal exam
Physical Examination
Life Threatening Conditions
| 1. Acute coronary Syndrome | - Retrosternal CP reproducible by exertion - Associated with Nausea/ diaphoresis/presyncope - History of CAD |
| 2. Aortic Dissection | - Tearing, severe, radiating to the back - Angina like, not relieved with nitro - Vital Signs: Difference in BP (>20) |
| 3. Tension pneumothorax |
- Mechanism of injury/ Stabbing pain/dyspnea - Hemodynamic compromise - Absent breath sounds on any one side |
| 4. Esophageal rupture | - History of severe vomiting/ retching - Severe retrosternal CP |
| 5. Pulmonary Embolism | - Dyspnea, pleuritic chest pain, symptoms of DVT, risk factors - Elevated heart rate - Wells Criteria |
| 6. Cardiac Tamponade | - Elevated HR, Elevated JVP |
Differential
CVS
R/S
GI
MSK
Psych
Panic attack
Stable / unstable Angina
Pericarditis
Aortic dissection
Cardiac tamponade
Pneumonia
Pulmonary Embolism
Pneumothorax
GERD
Mallory Weiss tears
Esophageal spasm
Costochondiritis
Rib Fracture
Herpes Zoster
Chest pain on and off since 2 weeks.
Age: 47
Gender: F
Name: Suzan
Status: HTN, DM with dyslipidemia
Age: 28
Gender: F
Name: Carol
Status: Healthy
Complaint
- Gradual onset
- Retrosternal chest pain, burning type
- Worse when laying down, worse with food
- Associated with sour taste in the mouth
- Severity: 5-6/10
- No associated dyspnea, palpitations, syncope or presyncope
- No significant past medical or family history.
- Exam: Epigastric tenderness, other exam normal.
Age: 28
Gender: F
Name: Carol
Most likely diagnosis
- GERD/ gastritis
Management
- Symptomatic with PPI or H2 blocker
- Lifestyle modifications
Age: 28
Gender: F
Name: Carol
Chest pain on and off since 2 weeks.
Age: 47
Gender: F
Name: Suzan
Status: HTN, DM with dyslipidemia
Age: 28
Gender: F
Name: Carol
Status: Healthy
Complaint
- Gradual onset, currently experiencing pain
- Retrosternal discomfort, heaviness
- Worse with physical activity but sometimes at rest as well
- Associated with dyspnea, palpitations
- Severity: 5-6/10
- Past medical history: DM, HTN, Dyslipidemia, no previous history of CAD
- Family history: CAD in dad, age 65
- Medication: Metformin, Ramipril, Atorvastatin
- Exam : BP: 220/110, HR: 62, RR: 22
- Appears Diaphoretic and uncomfortable
- CVS: ESM at the aortic area, R/S: normal, P/A: normal
Age: 47
Gender: F
Name: Suzan
Most likely diagnosis
1. ACS
2. Congestive heart failure
Management
-
Call 911
-
Administer aspirin/Oxygen/ sublingual nitrate if available
Age: 47
Gender: F
Name: Suzan
| MI/Angina | ECG, Trop | 1. ASA, Oxygen 2. Nitro 3. PCI/ Thrombo |
Management of common causes
| Pulmonary Embolism | CBC, D Dimer, INR, PTT Spiral CT |
1. Heparin/ LMWH |
| Pneumothorax | Clinical Diagnosis Cxray |
1. Oxygen, IVF 2. Needle Thoracocentesis 3. Chest Tube |
| Percicarditis | ESR, RF, ANA, anti DNA, TSH ECG Echo |
1. ASA 2-4 g/day 2. Ibuprofen 1200-1800mg/day 3. Colchicine 75-150mg/day |
| GERD | CBC, Hpylori +/- Endoscopy |
1. PPI 2. Lifestyle management 3. H pylori treatment |
| Costochondritis | None | 1. NSAID |
| Herpes Zoster | None | 1. Valacyclovir 1000mg TID x 7 days 2. Famciclovir 500mg TID x 7 days 3. Acyclovir 800mg 5x/day x 7 days |
| Condition | Investigations | Treatment |
|---|
SAMP Questions

1. What are the initial steps? List 4.
2. List 5 components of clinical decision making rule for CAD
3. How would you manage Aleksander if he subsequently went into cardiorespiratory arrest?
Aleksander and his wife were visiting relatives near your office when he began to feel very unwell and they unexpectedly presents to the office. The receptionist recognizes that he looks very unwell and calls the nurse, who immediately escorts Aleksander into a clinic room. He is complaining of chest pain, feeling faint and very nauseated. You are subsequently summoned from another patient room.
Aleksander
1. What are the initial steps? List 4.
1. Activate office protocol for emergencies and call 911
2. Conduct a primary survey including assessment of their level of consciousness and ABCs
3. Obtain a set of vital signs including heart rate, blood pressure and respirations.
4. Administer aspirin (2 x 81 mg uncoated tablets, chewed).
5. Give supplemental oxygen only if the oxygen saturation is less than 90%
6. Consider nitroglycerine spray SL if systolic blood pressure > 90 mmHg.
7. Consider getting an ECG if available.
Aleksander
2. List 5 components of clinical decision making rule for CAD
1.Age/sex: Men>55, women>65
2.Known CAD or Cerebrovascular disease
3.Pain worse with exertion
4.Pain not reproducible by palpation
5. Patient assumes that the pain is cardiac in origin
Aleksander
3. How would you manage Aleksander if he subsequently went into cardiorespiratory arrest?
- Alert 911 of Aleksander’s change in status
- Start compressions and artificial ventilations.
- If equipment and expertise are available, you might use an AED and secure the airway
Aleksander
1. Give 5 differential diagnosis.
2. List 5 physical signs suggestive of tension pneumothorax.
A 36 year old male comes to the office with left sided chest pain that started suddenly after he got into a fist fight with his colleague. He is having some trouble breathing and pain is worse when leaning forward or coughing. He is a smoker and is otherwise healthy. He has a family history of early MI in his dad at the age of 55.
Peter
1. Give 5 differential diagnosis.
Peter
- Pneumothorax/ Pleuritis
- Rib fracture
- Cardiac Tamponade
- ACS
- Musculoskeletal pain
2. List 5 physical signs suggestive of tension pneumothorax.
Peter
- Hypotension and tachycardia
- Tachypnea
- Tracheal deviation
- Hyperresonant note on percussion
- Absence of breath sounds on one side
Thank you
Chandni R. Nijjar
PGY2 FM
Chest Pain
By Tarun Batra


