



Tips & Tricks
Tips & Tricks
Skin. The largest organ of the human body. WebMD says that the skin has a total area of approximately 20 square feet. Another source reports that the skin equals about 15% of a person’s body weight and consists of more than 11 miles of blood vessels. When we think of a body’s organs, we think internally, but the skin is the exception to the definition.
That is not to say that the skin isn’t affected internally. It is so complex that it must fight the elements inside and outside the human body. Skin is vulnerable as well as strong, but it is not impervious. There are unknown possibilities awaiting our skin, but we can only discuss what we know. Dry skin treatments do exist.
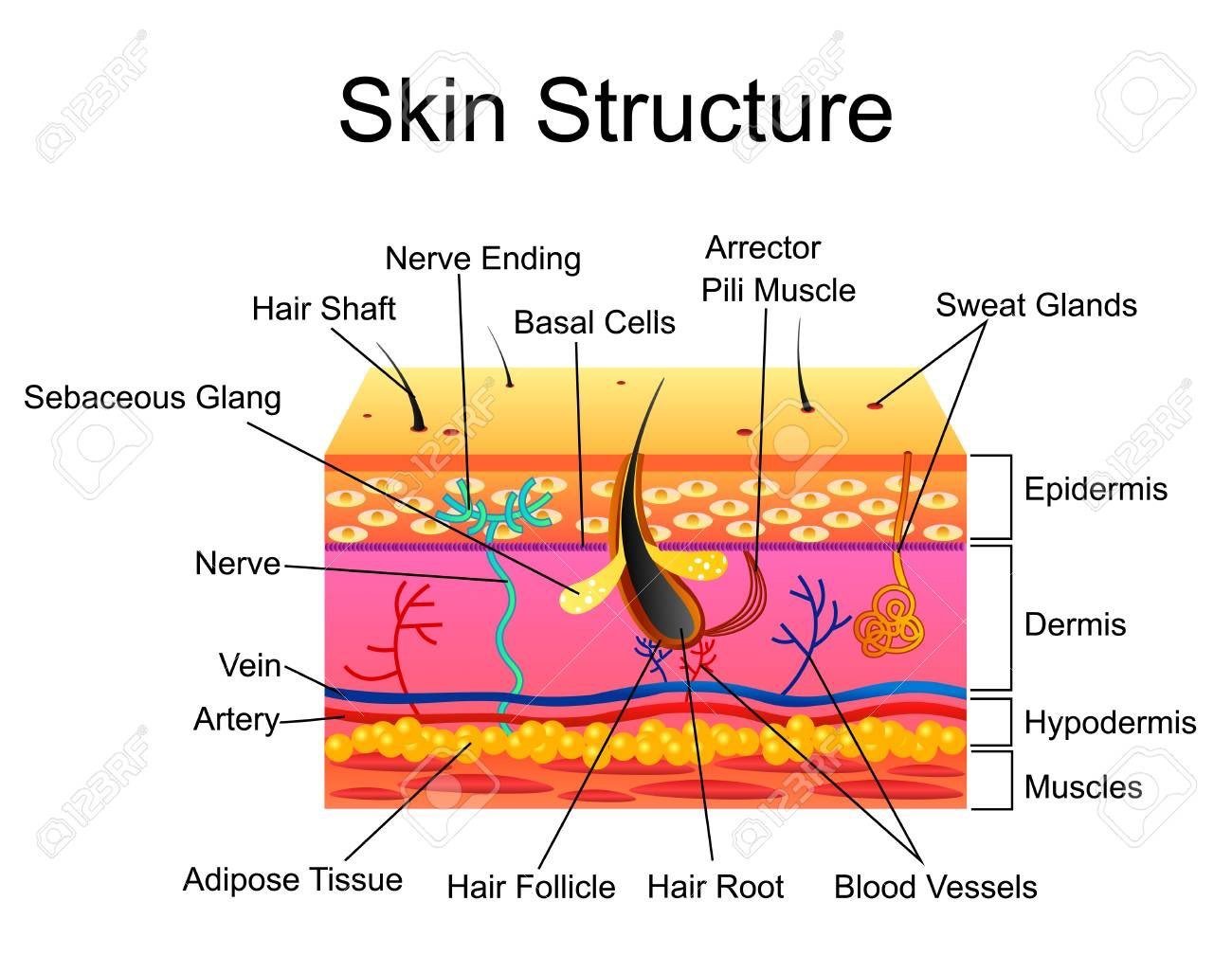
The skin has layers for protection. We might only think of the epidermis, the outer layer we see and feel. But there are two other layers, the dermis and the subcutaneous hypodermis. Each layer has other layers of its own, e.g. the epidermis is comprised of four layers.
With 5 or more types of receptors, the skin is affected by the sense of feeling or ‘touch’ and is sensitive to the balance of conditions, e.g. temperature, pH, bacteria, viruses, and foreign bodies. The skin is susceptible to damage, irritation, and infection, but it regenerates itself every 27 days approximately.
Bacteria
Think of our skin as a biosphere or host for more than 1,000 types of bacteria (part of the microbiome living in or on the body). By comparison, only a few are pathogenic and cause us real problems. The safe bacteria ‘colonise’ our bodies amicably, living in or on the body, even if they did distort the ‘facts’ to immigrate.
Viruses
Viruses act differently to bacteria. Their nature is to infiltrate and live inside the cell. These are the worst of the space invaders of the human condition. Viruses aren’t colonisers by nature. They are ‘parasites’, obligate intracellular parasites to be exact. They are only ‘alive’ while in a host cell.
3 Conditions
Eczema. Atopic dermatitis is caused by hypersensitivity to a foreign agent making contact with the skin, e.g. ingredients within soaps and fabrics, etc. It is an overreaction, like an allergy.
Its appearance is usually red, cracked surface that might weep or fill with pus. It can appear blister-like and feel intensely itchy to the point of discomfort and pain when scratched excessively. It does not generally appear scaly, but might peel.
Psoriasis. A chronic autoimmune condition with no cure, it is the overactive formation of new skin cells causing itchiness and potentially stinging or burning sensations to the skin.
The dead cells build up on the skin before flaking away. Psoriasis is identifiable by its white, scabby, scaly plaque over underlying red skin. It is not contagious.
Seborrheic Dermatitis. A superficial fungal skin disease that may be an abnormal immune reaction to Malassezia yeasts living on the skin is a likely culprit of this particular irritation.
It can present with red, flaky, scaly, itchy areas on the skin’s surface, usually in areas with oily glands, e.g the scalp and nose crease. It can also cause a burning sensation.
Inflammation, the appearance of a scaly rash, and itchiness are common symptoms for psoriasis, seborrheic dermatitis and eczema. The skin might ooze or be dry and flaky. None of these are contagious.
Both seborrheic dermatitis and psoriasis can appear scaly and can almost look indiscernible in some cases. Note the thickness of the skin and how inflamed it is. Triggers, such as stress, hormonal changes, dry, cold weather and immune system infections might be cause of two or any of the conditions.
Psoriasis comes from an internal struggle with the immune system and can cause extra symptoms such as joint stiffness or a visible change in the nails that do not arise with types of dermatitis. It can flare up through an injury to the skin and through the use of some medications.
The severity of the itch sensation varies between the three conditions, as do their causes. Eczema is often ‘outgrown’ in adulthood. Psoriasis can be linked to other serious health conditions.
Treatment plans are quite different for both psoriasis and eczema, but there may be some overlap in types of treatment within each plan, e.g phototherapy with UV light, topical anti-fungal creams, topical corticosteroids and non-corticosteroid medicine, medicated shampoos, gentle cleansers and moisture therapy and emollients.
If symptoms persist and/or intensify, a doctor should be consulted. The GP may refer patients to a dermatologist. In some cases, antibiotics might be prescribed.
All three of these skin conditions are closely related, cause discomfort and potential embarrassment. None are contagious and might be avoided with proper skincare, especially moisturisers.
In Conclusion
References: Cloud9skin, WebMD
By Tips & Tricks
