
Trang Le
#math graduate. Postdoc fellow with Jason Moore.
Ali Torkamani, Nathan E. Wineinger and Eric J. Topol
TRANSLATIONAL GENETICS REVIEWS
Paper Discussion
Genetic architecture of common adult-onset diseases
common disease, common variant hypothesis
2007: first large-scale GWAS
2007 - 2012:
Latest GWAS meta-analysis:
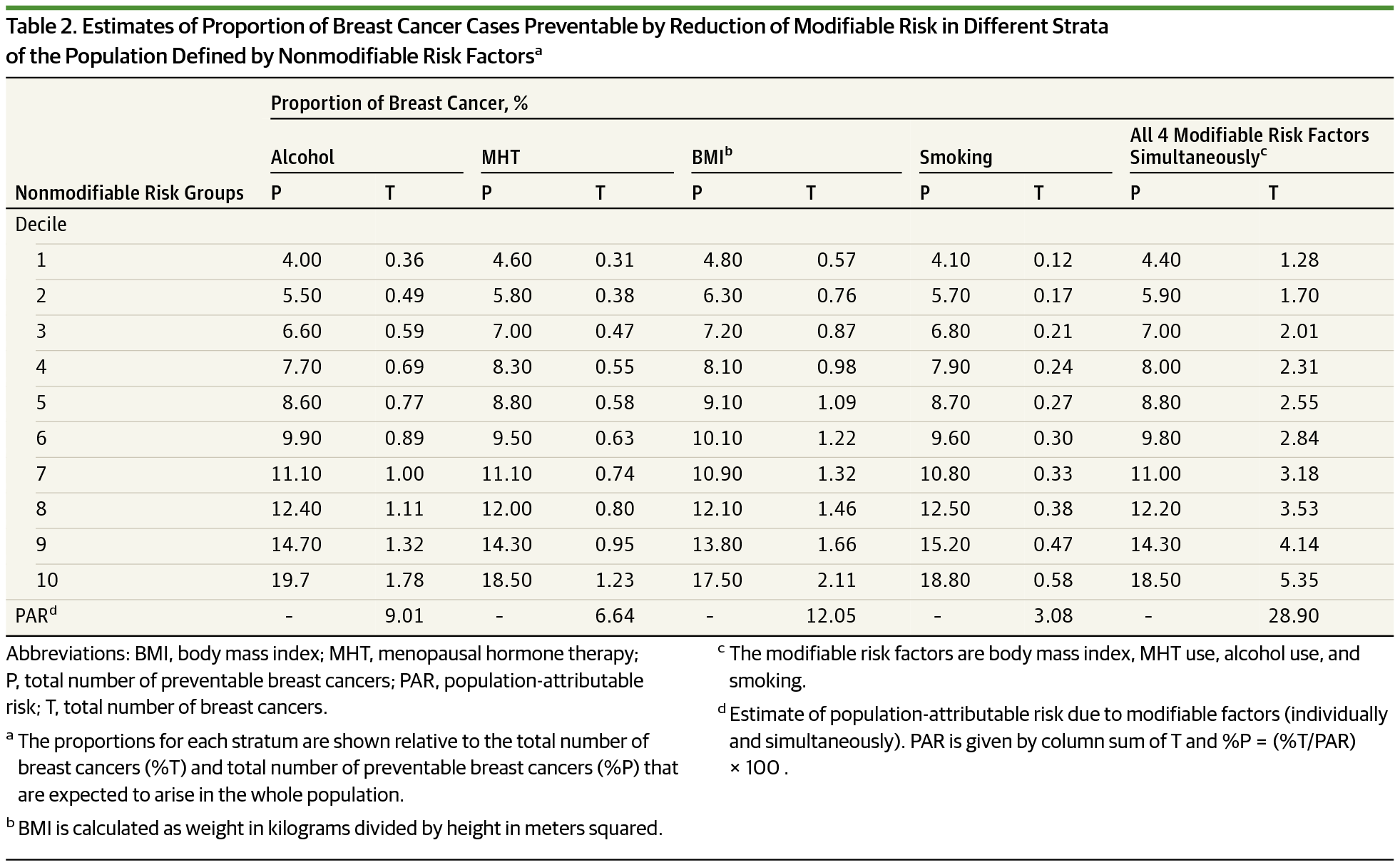
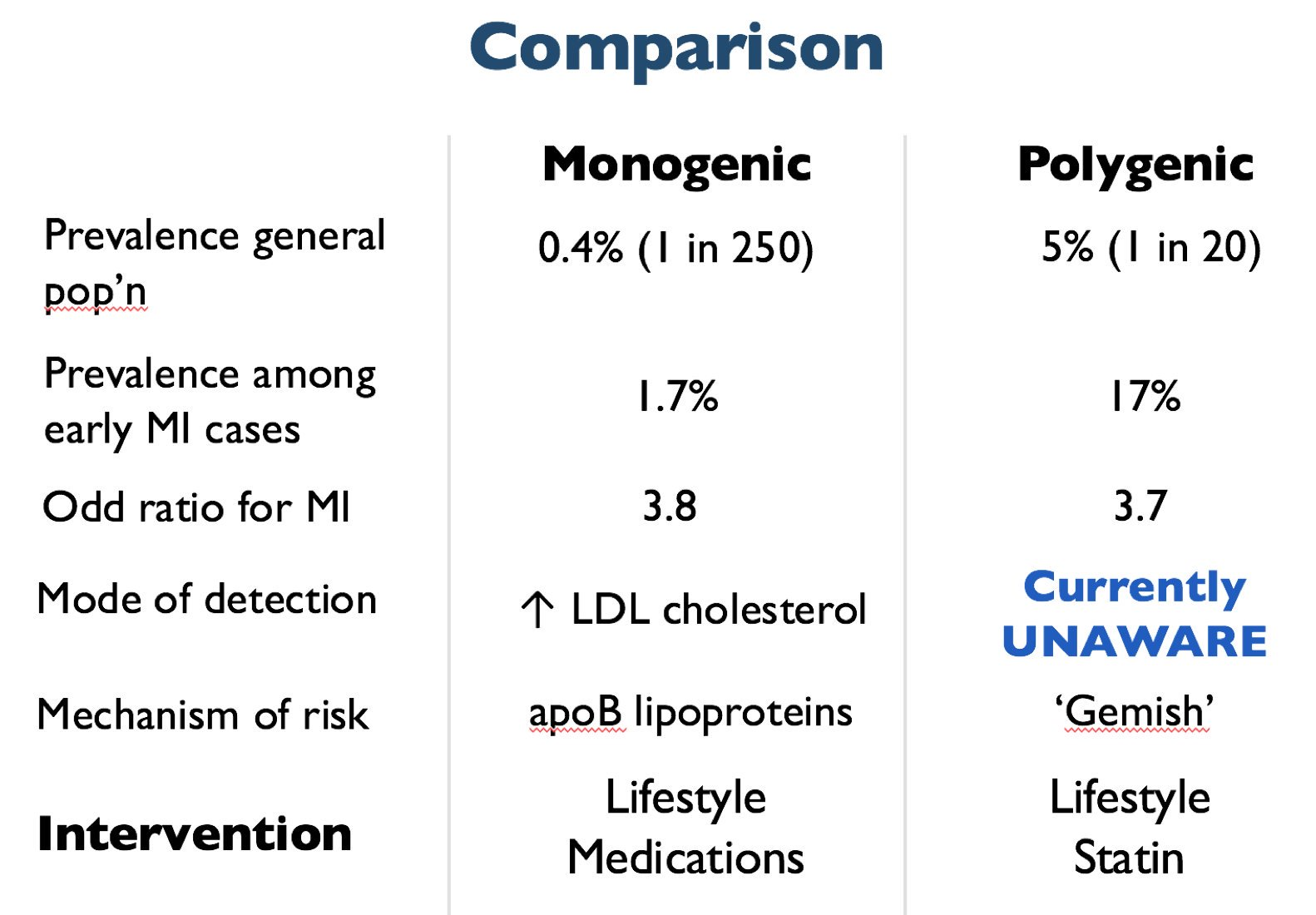
Although the total heritability explained by BRCA1 and BRCA2 variants is low [due to low prevalence of mutations], BRCA1 and BRCA2 testing can identify a subset of individuals whose absolute risk of disease is significantly higher than that of the average individual in the general population.
Disease risk:
β: effect size in discovery sample from OLS (continuous trait) or logistic reg (binary trait; log(OR))
SNP_{ij}: # alleles (0,1,2) for SNP i of person j in target sample
Probabilistic susceptibility
→ identify groups of individuals who could benefit
→ prioritize interventions and screening
→ life planning
Leading heritable causes of death:
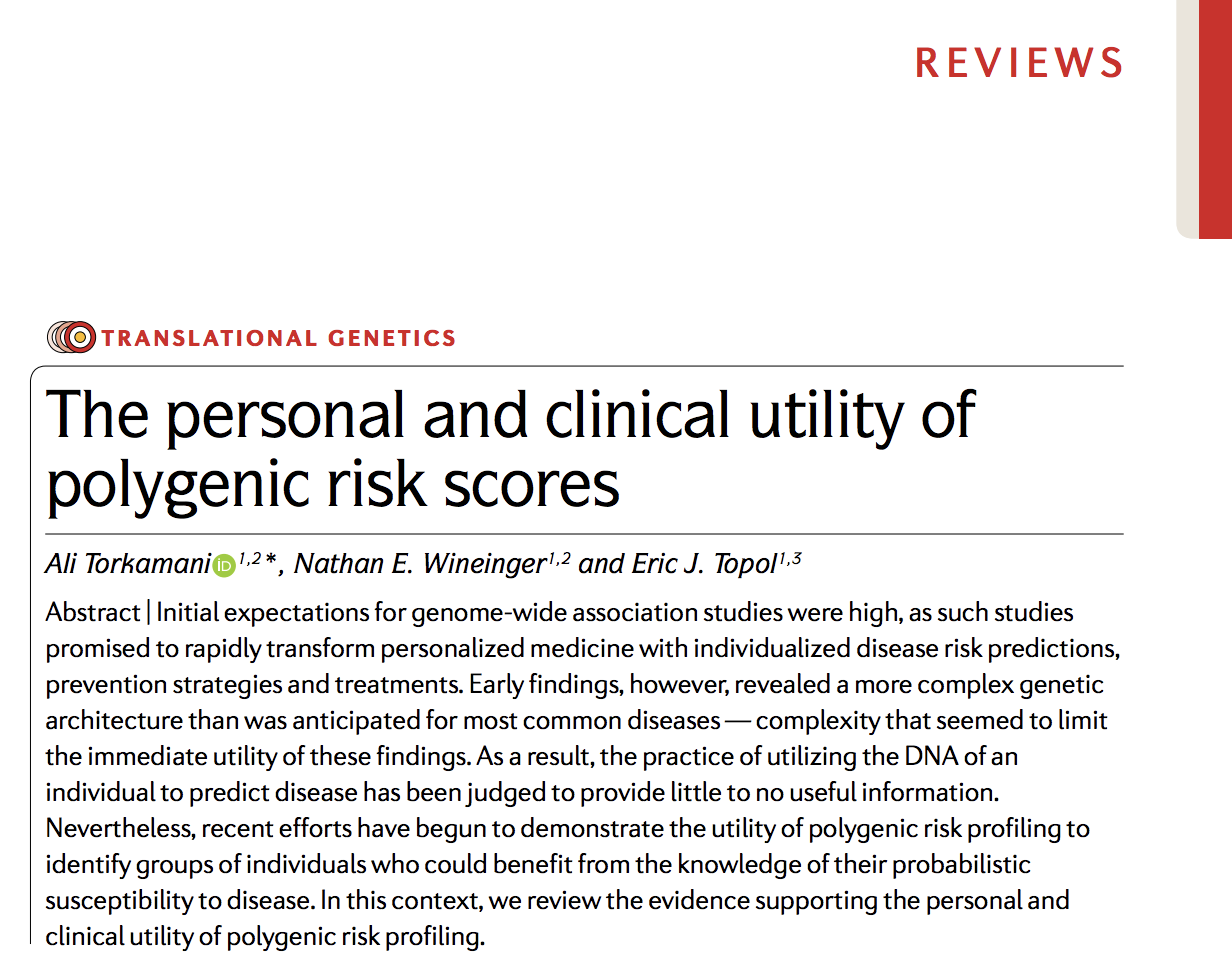
when combined with clinical risk estimates, a PRS may modify the estimated risk of some individuals so that their combined risk is at or above the level of risk recommended for the initiation of statin therapy
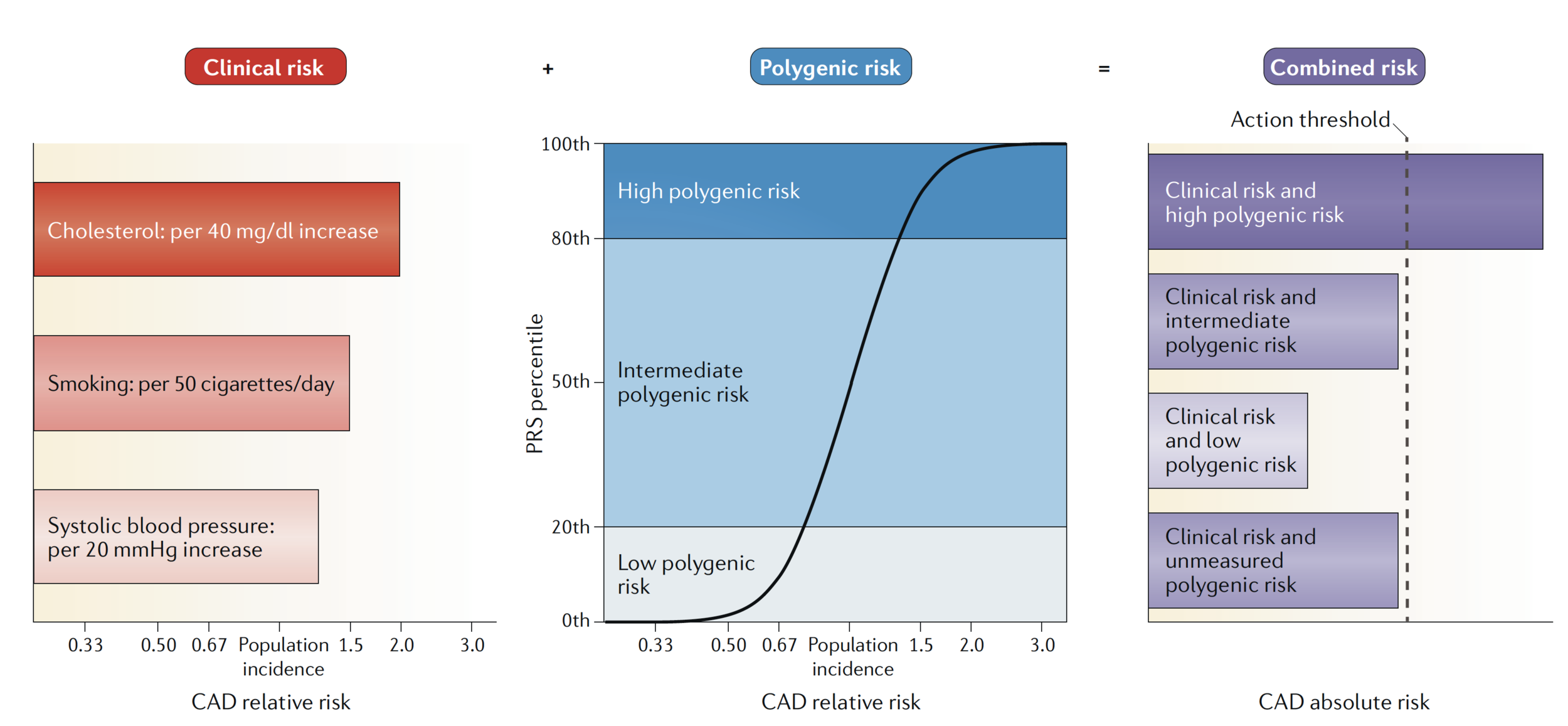
Model effect.
2 equivalent models (relative distribution of diseased vs. healthy individuals) yield different conclusions in utility
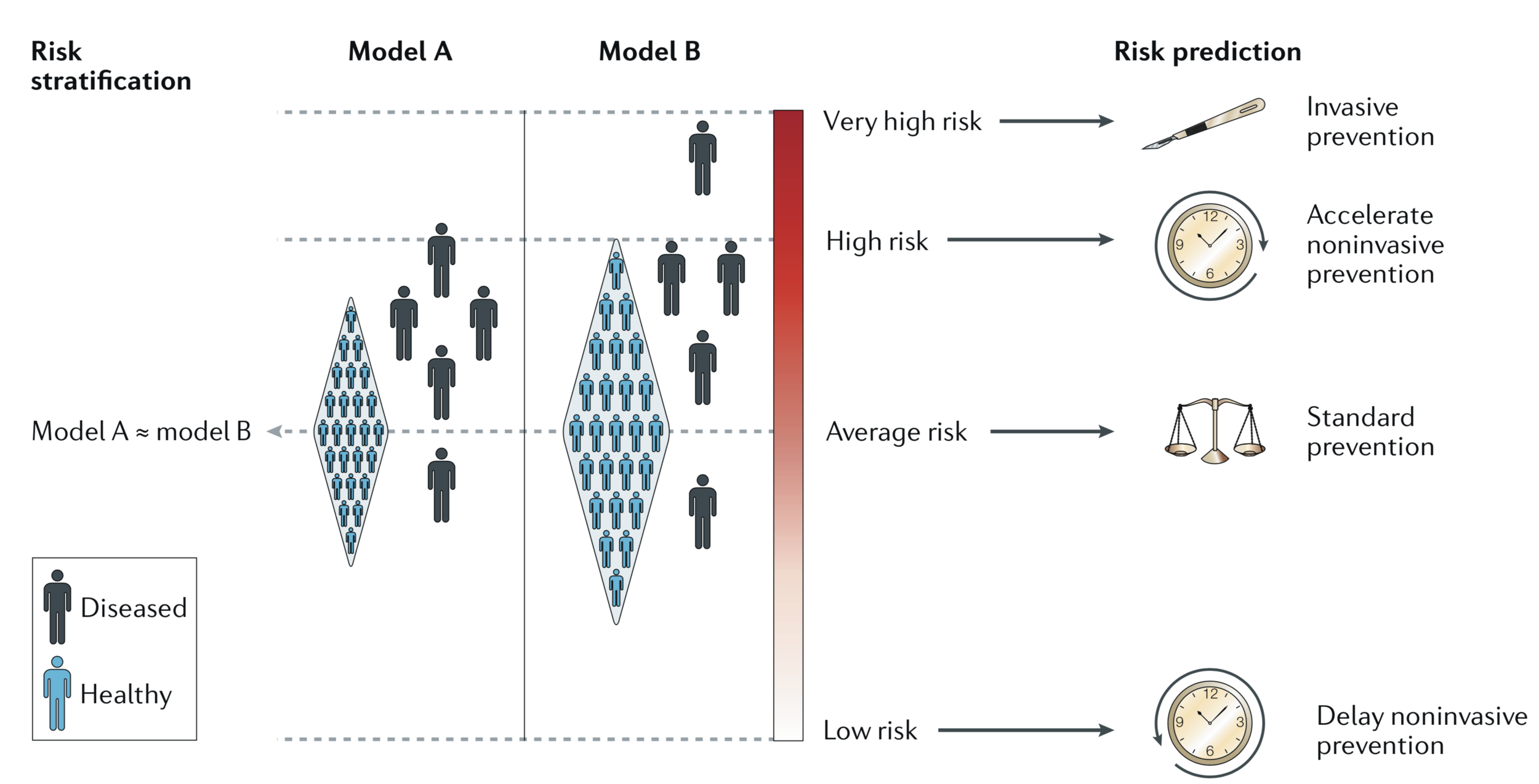
#individuals benefits from intervention/# individuals treated
by PRS tier
depends on a fairly complex interplay between disease-specific and intervention-specific risks and benefits
Disease screening: decision to initiate and the interpretation of disease screens
Life planning: the personal utility that PRSs can provide, even in the absence of preventive action
Coronary artery disease
Individualized management of disease is central to the philosophy of precision medicine, with genetic factors often invoked for this strategy to personalize health care.
Breast cancer
Colorectal cancer
Prostate cancer
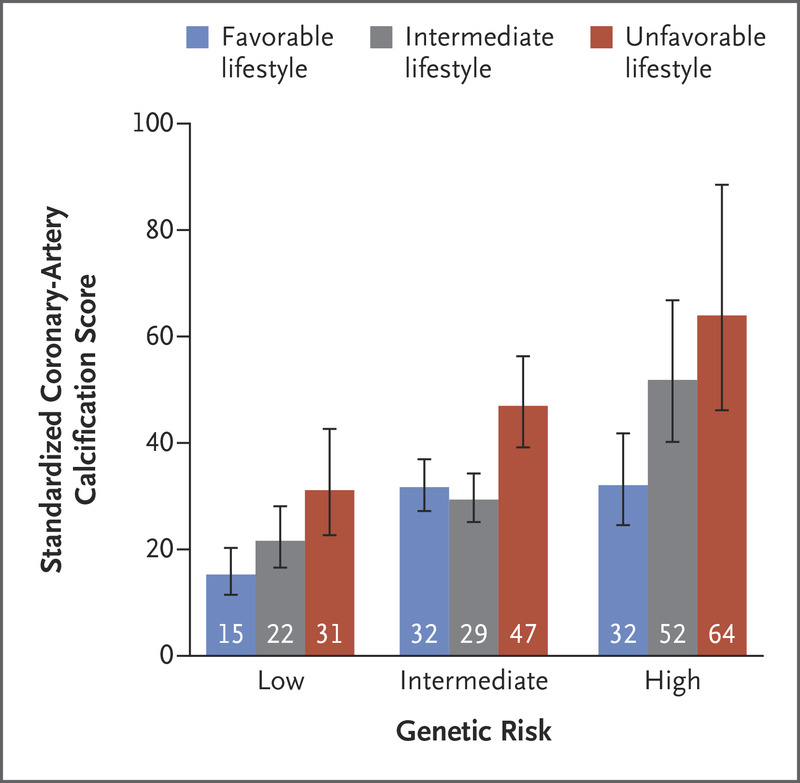
Clarifying susceptibility and quantifying benefits of healthy behavior → induce & maintain behavior change
Within each subgroup of genetic risk, a significant trend was observed toward decreased coronary-artery calcification among participants who were more adherent to a healthy lifestyle
Clarifying susceptibility and quantifying benefits of healthy behavior → induce & maintain behavior change
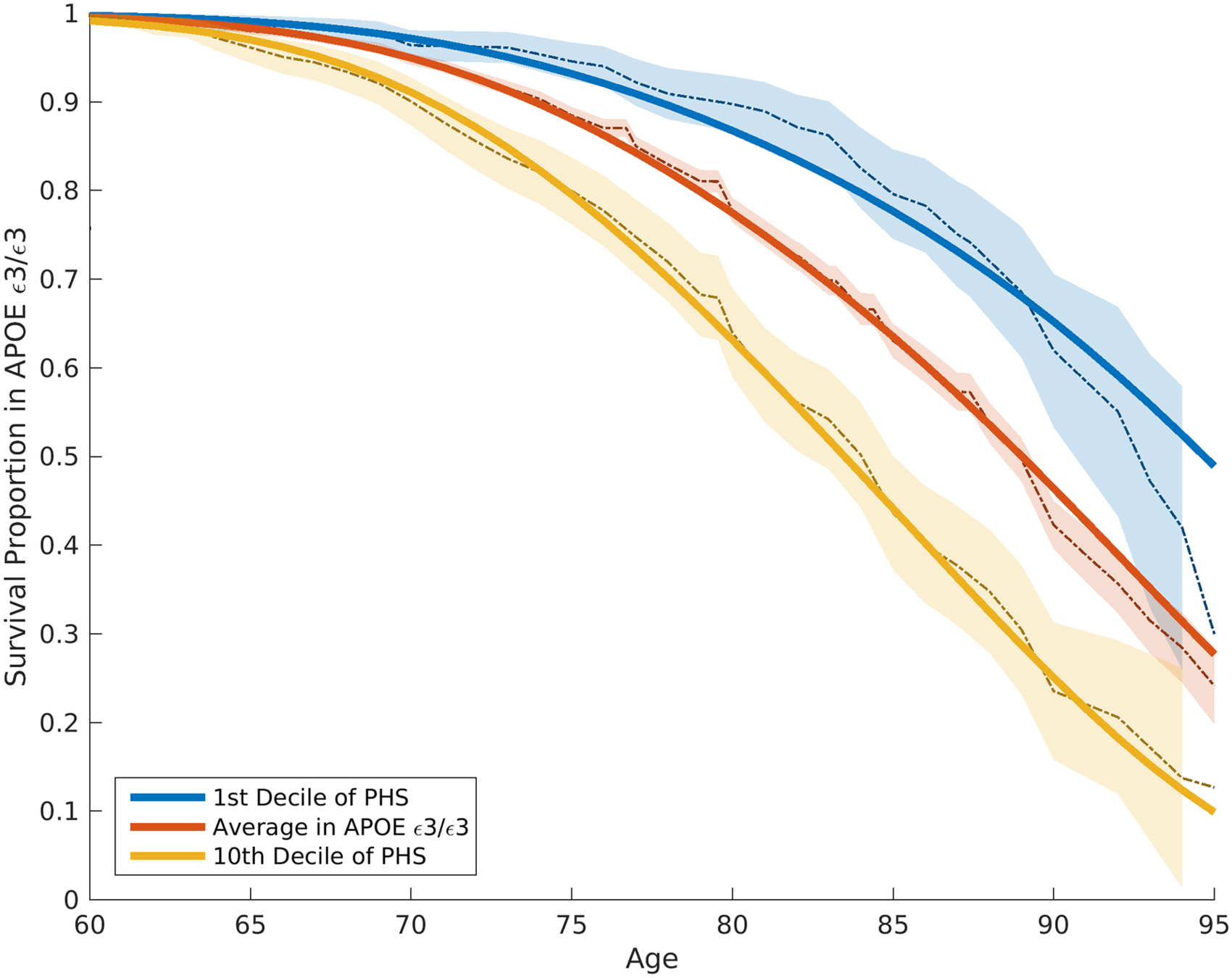
PRS informs financial, legal and care planning.
Imperfect correlation with causal genetic factor(s) → Uncertainty in variant’s estimated effect size → Poor transferability → Inequities
Improve comprehensiveness and generalizability
PRS model via ML and AI
https://slides.com/ttle/the-personal-and-clinical-utility-of-polygenic-risk-scores
Amit V. Khera, Mark Chaffin, Krishna G. Aragam, Mary E. Haas, Carolina Roselli, Seung Hoan Choi, Pradeep Natarajan, Eric S. Lander, Steven A. Lubitz, Patrick T. Ellinor &
Sekar Kathiresan
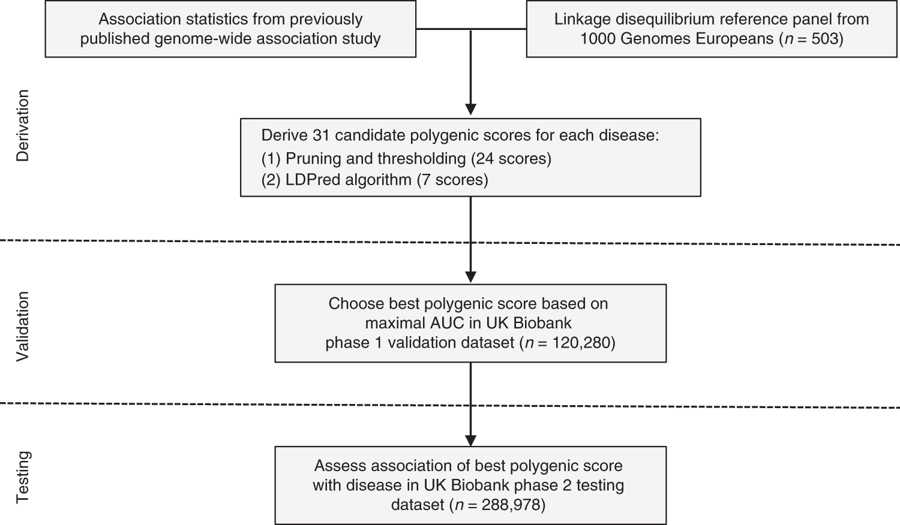
Statistical analysis (testing):
GPSs derivation:
GPSs calculation:
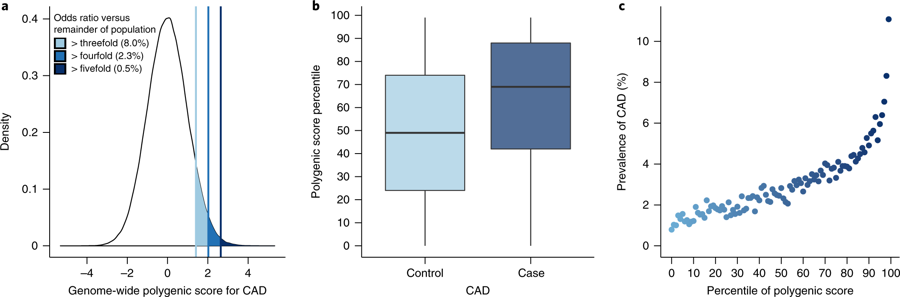
Fig. 2: Risk for CAD according to GPS.
2a: Distribution of GPSCAD in population. For those in top 1% of CAD score, 11% had a heart attack by mean age 57 (vs 0.8% in lowest 1%).
2c: Y axis = PPV for CAD (by mean age 57). X axis = percentile bins of score; 100 bins: percentile of the score & prevalence of CAD within each bin plotted
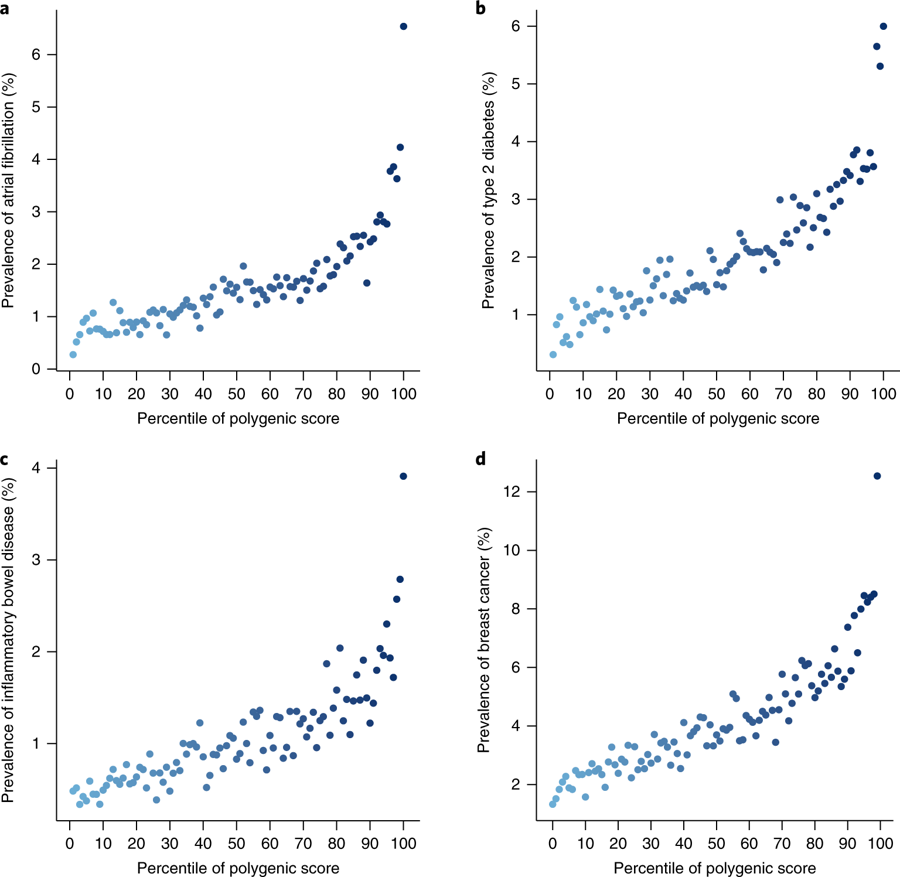
Fig. 3: Risk gradient for disease according to the GPS percentile.
For those in top 8% of scores, 3-4-fold higher risk than all others.
"Germline inherited component to any common disease can be captured by a single number that follows normal distribution."
By Trang Le
Presentation on 2018-10-01 for the joint Lunch&Learn between the Moore Lab and Ritchie Lab.



