

Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
Note: Will not be discussing ECG diagnosis
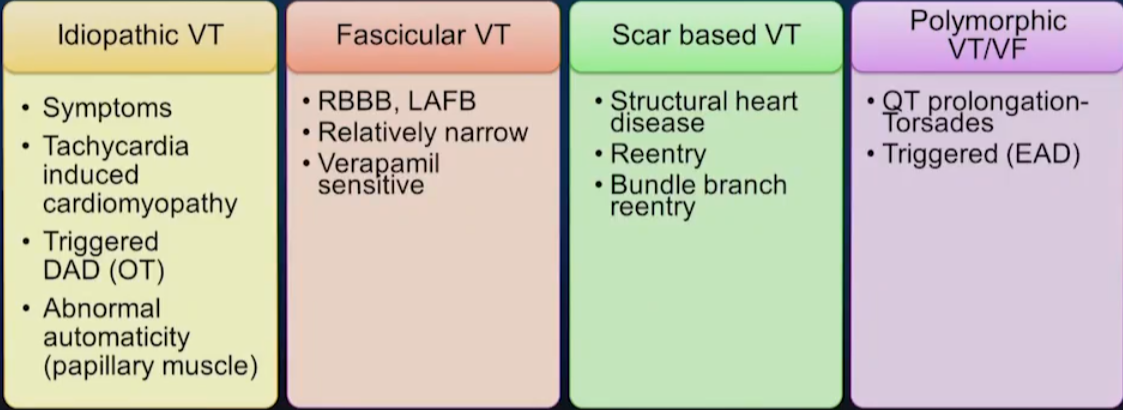
Seen in a structurally normal heart
Examples:
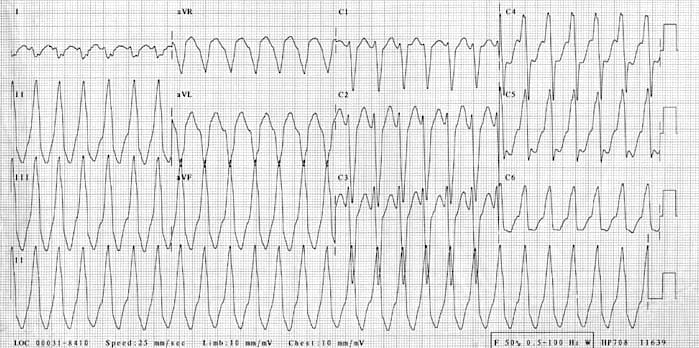
RVOT VT
https://litfl.com/right-ventricular-outflow-tract-rvot-tachycardia/
RVOT VT
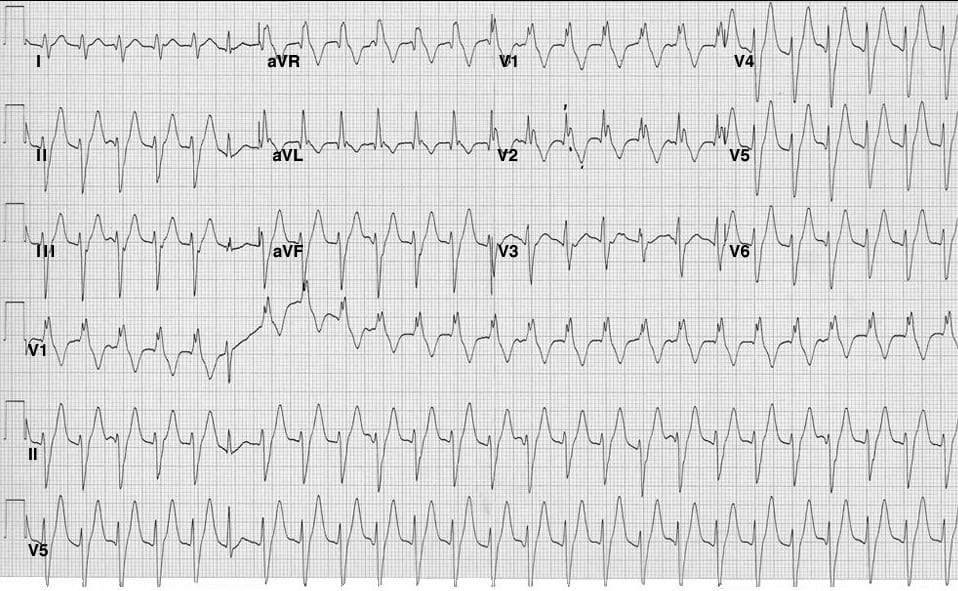
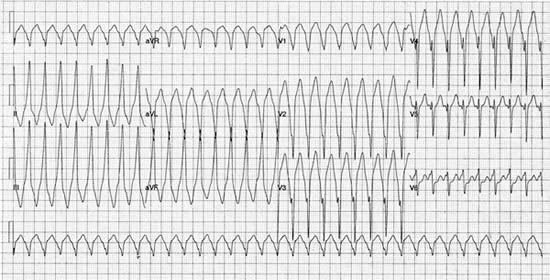
Fascicular VT
https://litfl.com/idiopathic-fascicular-left-ventricular-tachycardia/
Fascicular VT
https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-8/How-to-recognise-and-manage-idiopathic-ventricular-tachycardia
Tx symptoms with meds and ablation
Generally no ICDs
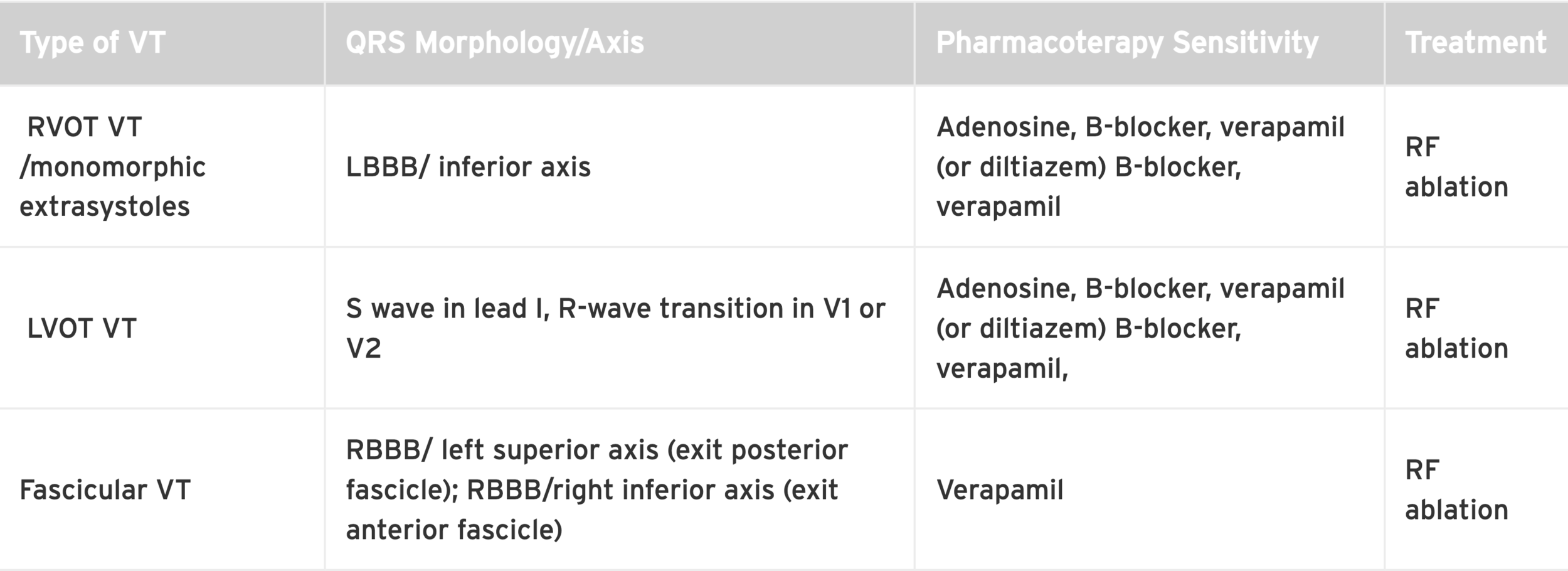
Morphology of VT depends on exit site
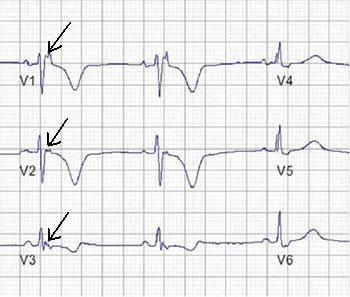
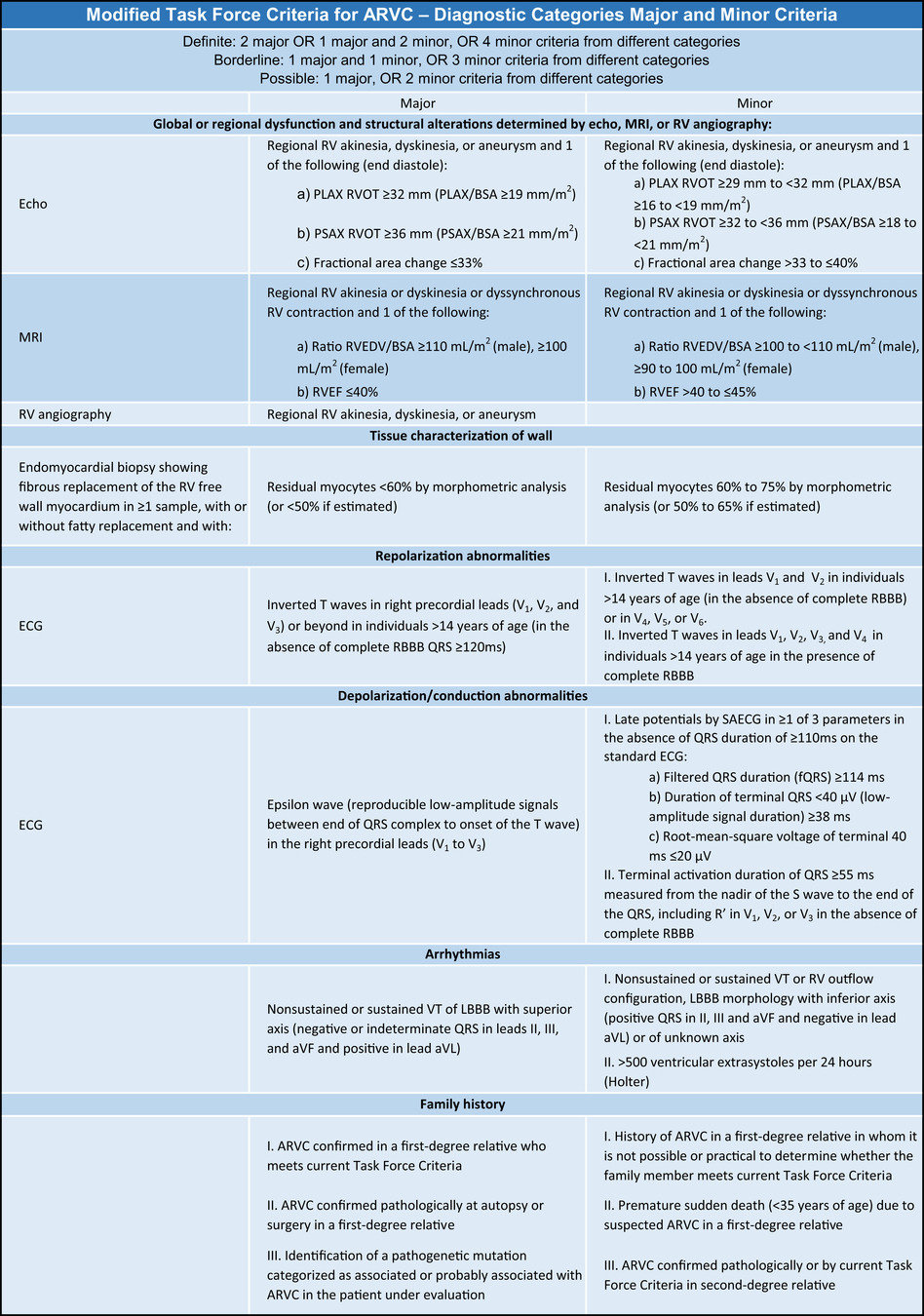
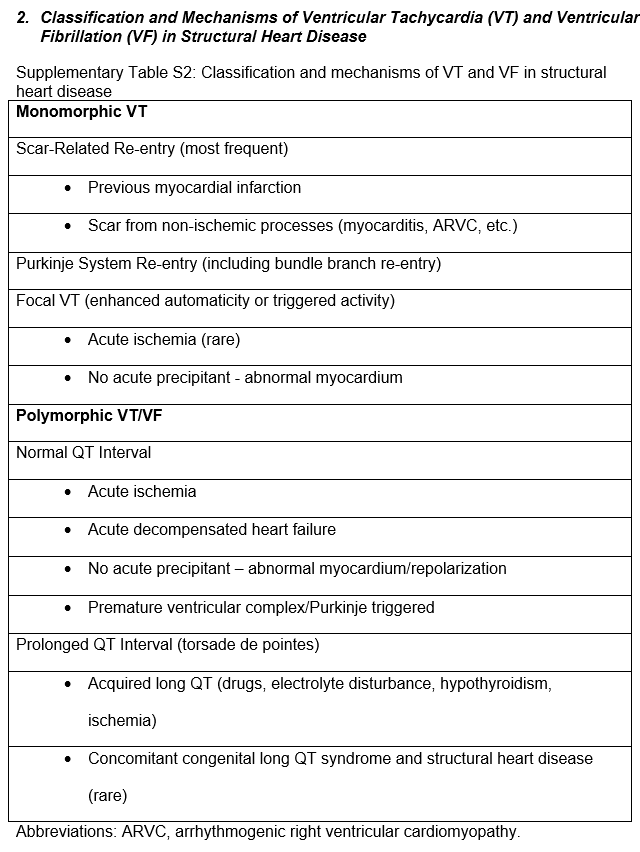
ARVC
https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-7/Diagnosis-and-management-of-arrhythmogenic-right-ventricular-dysplasia
ARVC
https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-7/Diagnosis-and-management-of-arrhythmogenic-right-ventricular-dysplasia
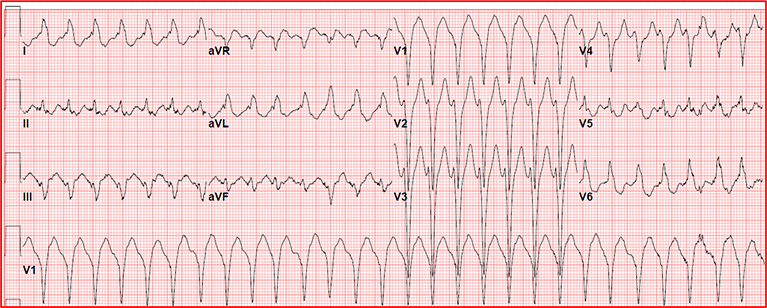
LBBB, Superior Axis
Further Reading:
Sarcoid
Durocher et al. https://www.cjcopen.ca/article/S2589-790X(21)00192-X/fulltext
Sarcoid
https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.118.034687
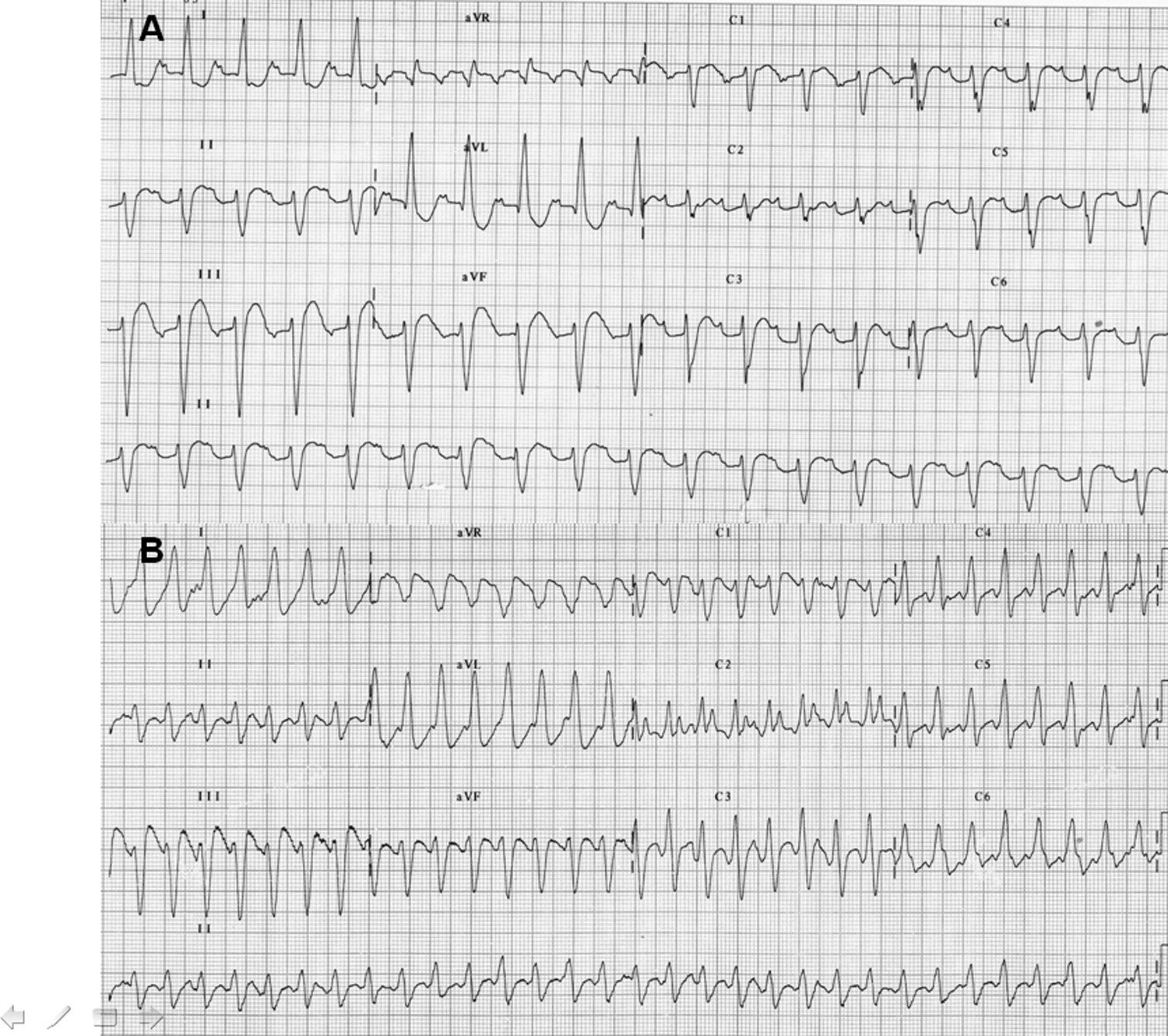
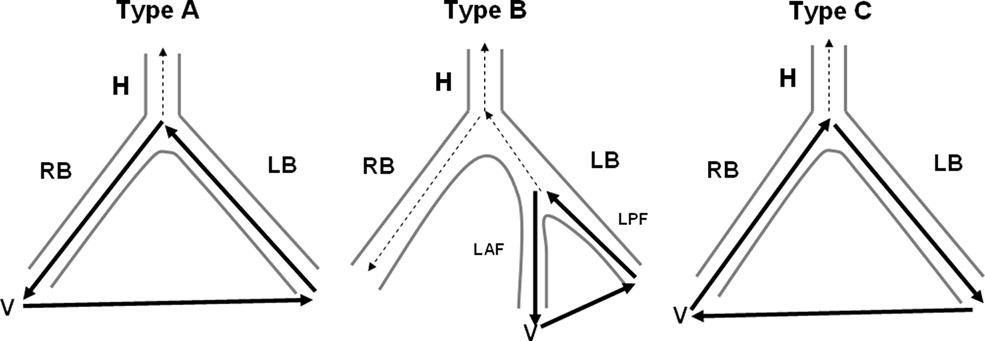
Bundle Branch
Reentry
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S1547527108002270?via%3Dihub
Bundle Branch Reentry
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S1547527108002270?via%3Dihub
By Atul Jaidka



