
Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
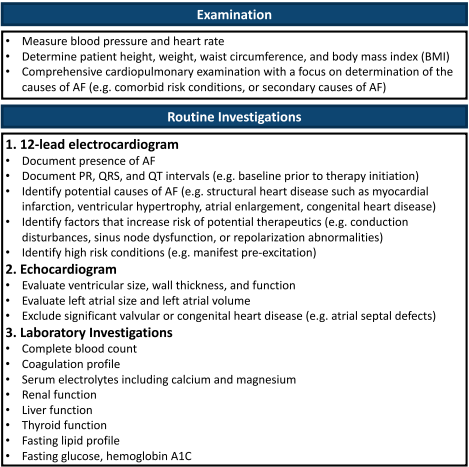
You are seeing a 68 year old male (Class I obesity, Hypertension, and diet controlled DM2) in clinic who presents with anxiety. His brother developed atrial fibrillation and he is wondering whether he should have screening. How should we approach screening in this patient?
https://theskepticalcardiologist.com/
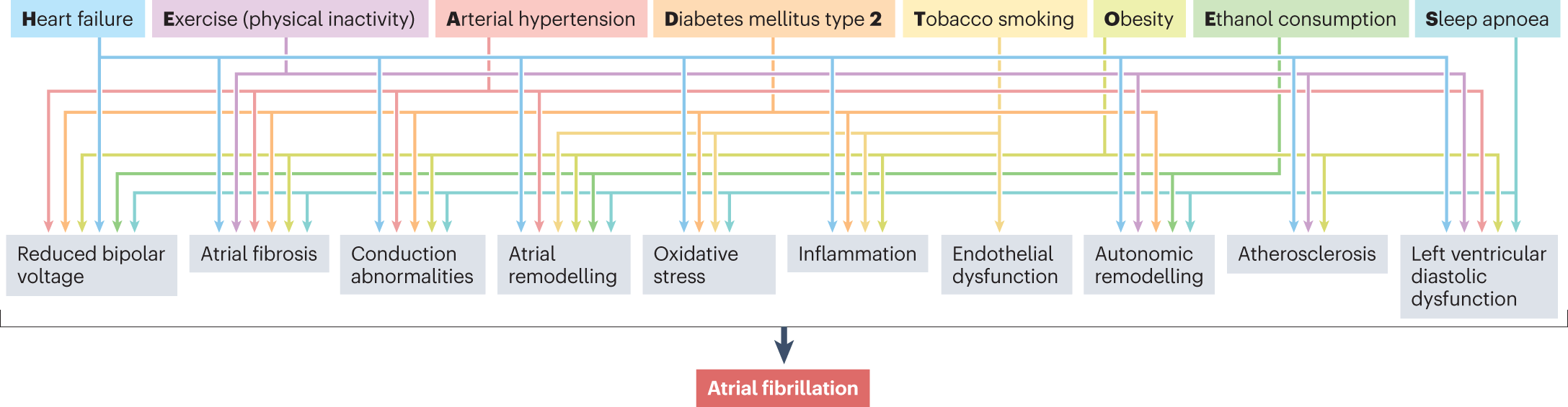
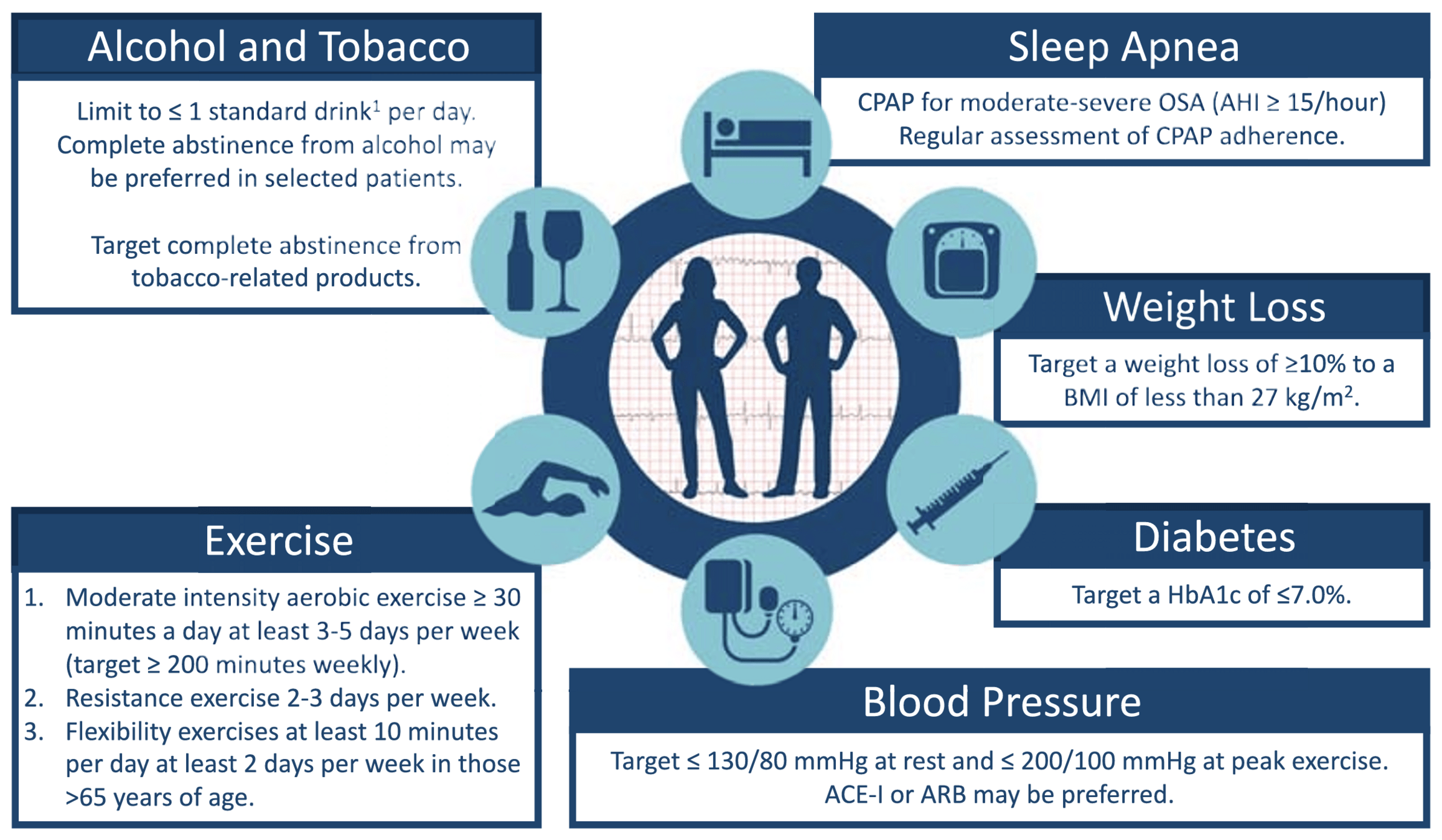
What are risk factors for atrial fibrillation and how would you counsel the patient on modifying them?
"HEAD 2 TOES"
https://www.nature.com/articles/s41569-022-00820-8
"HEAD 2 TOES"
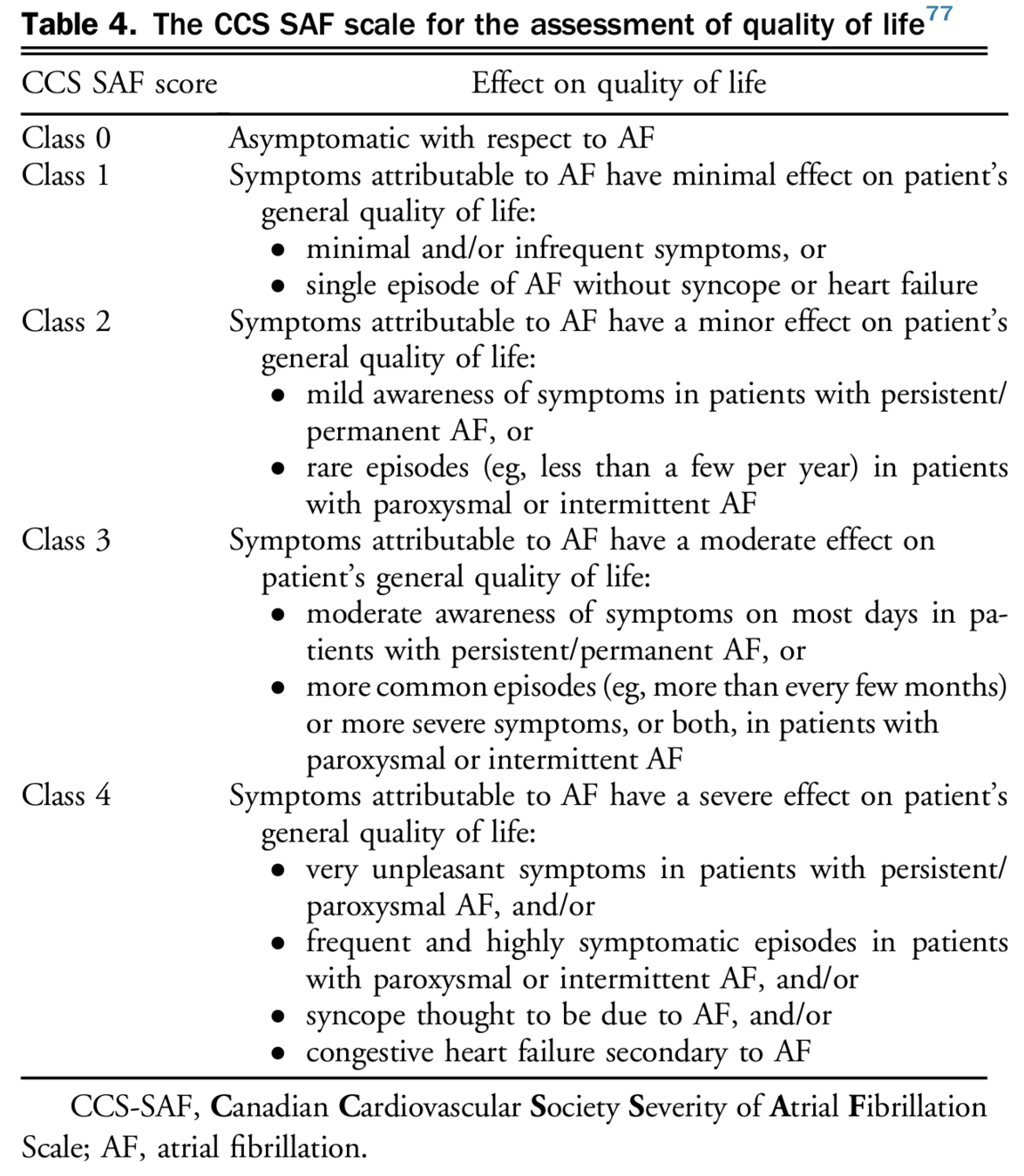
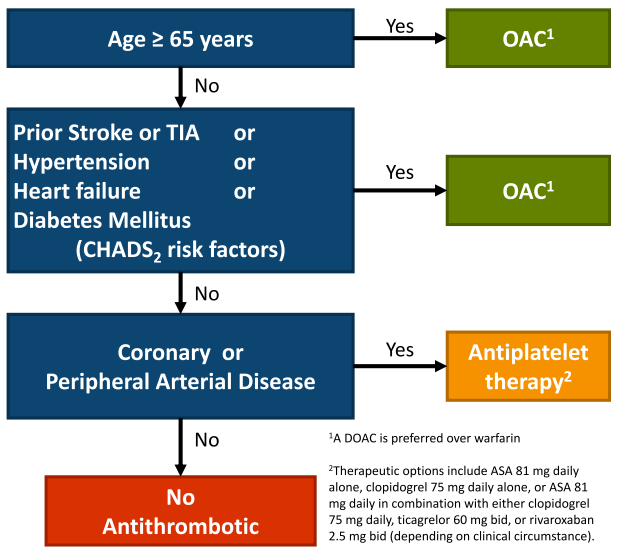
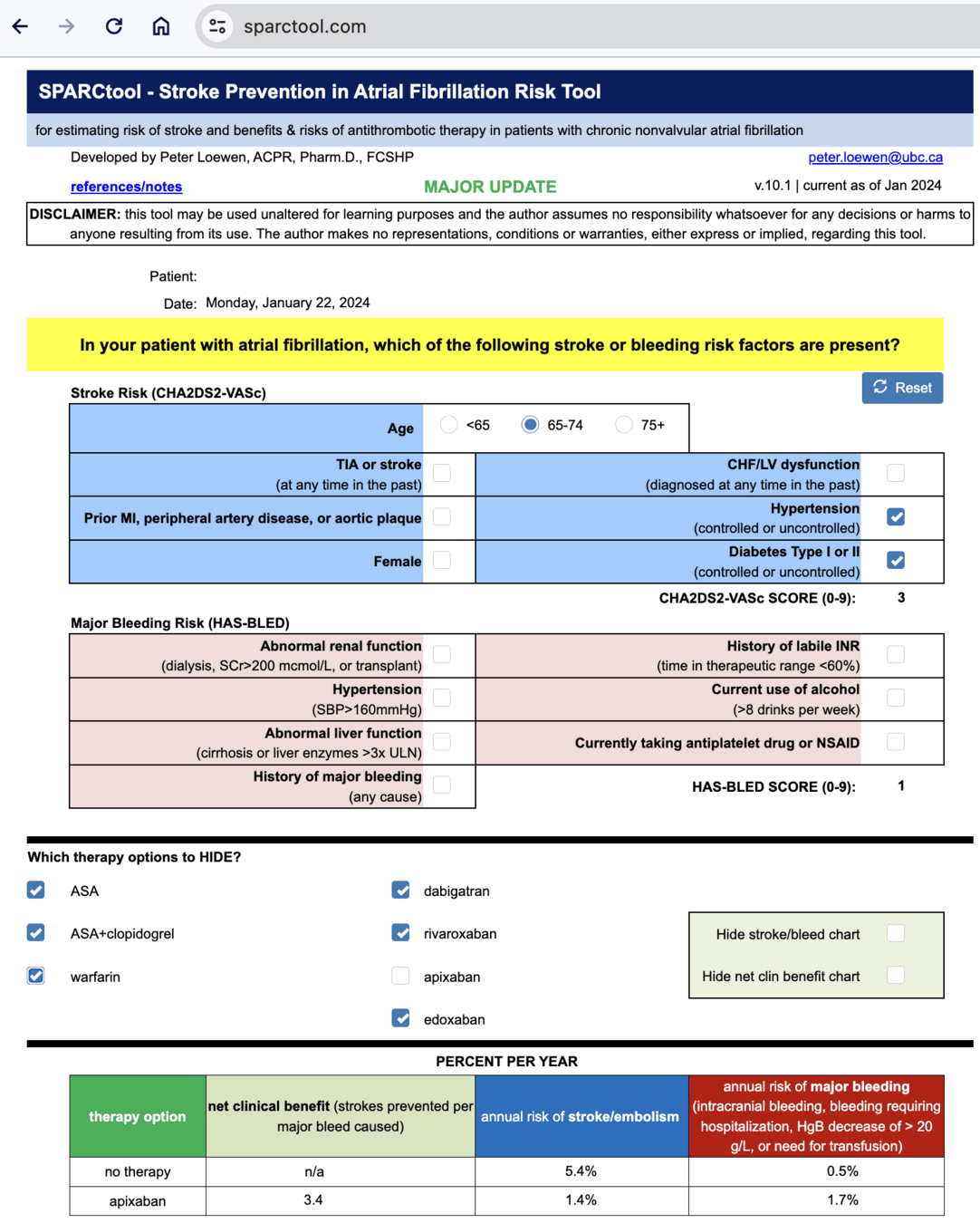
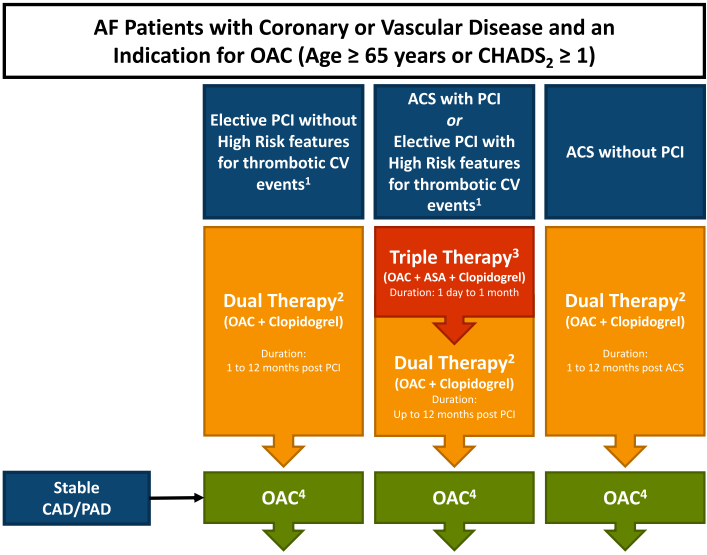
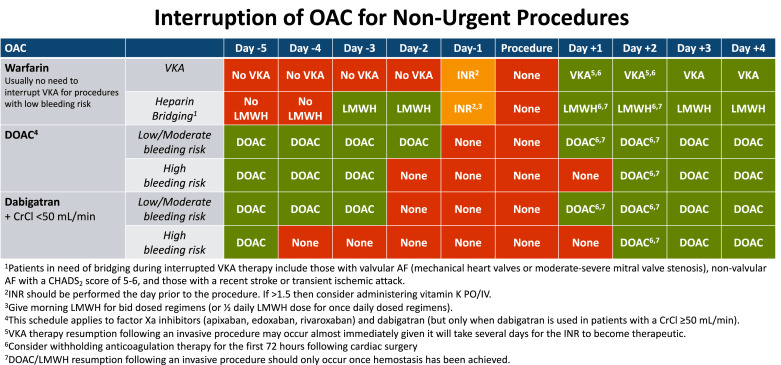
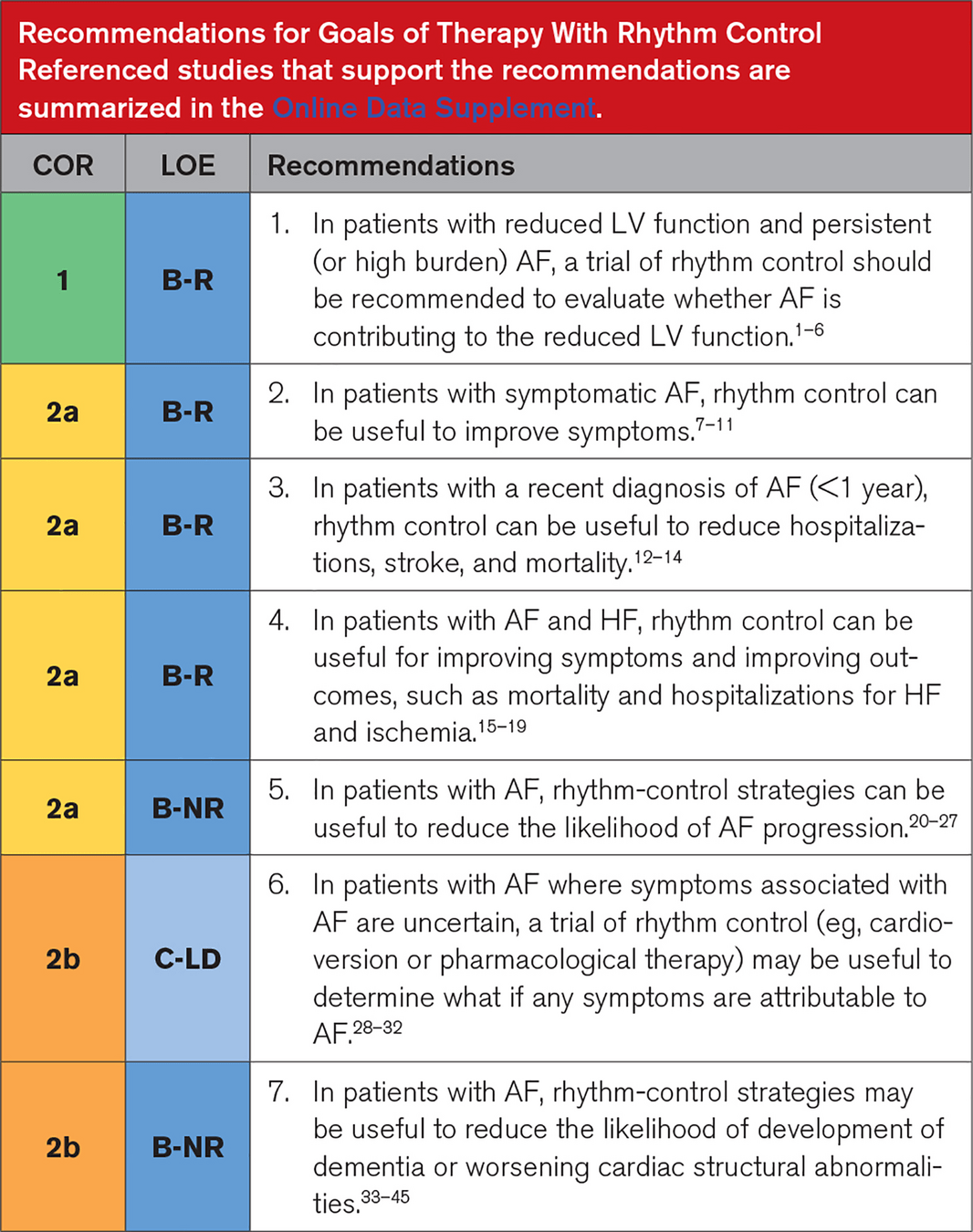
We have initiated a multi-disciplinary risk factor modfication plan for the patient and now move to the stroke prevention and arrhythmia management. How should we manage this patient?
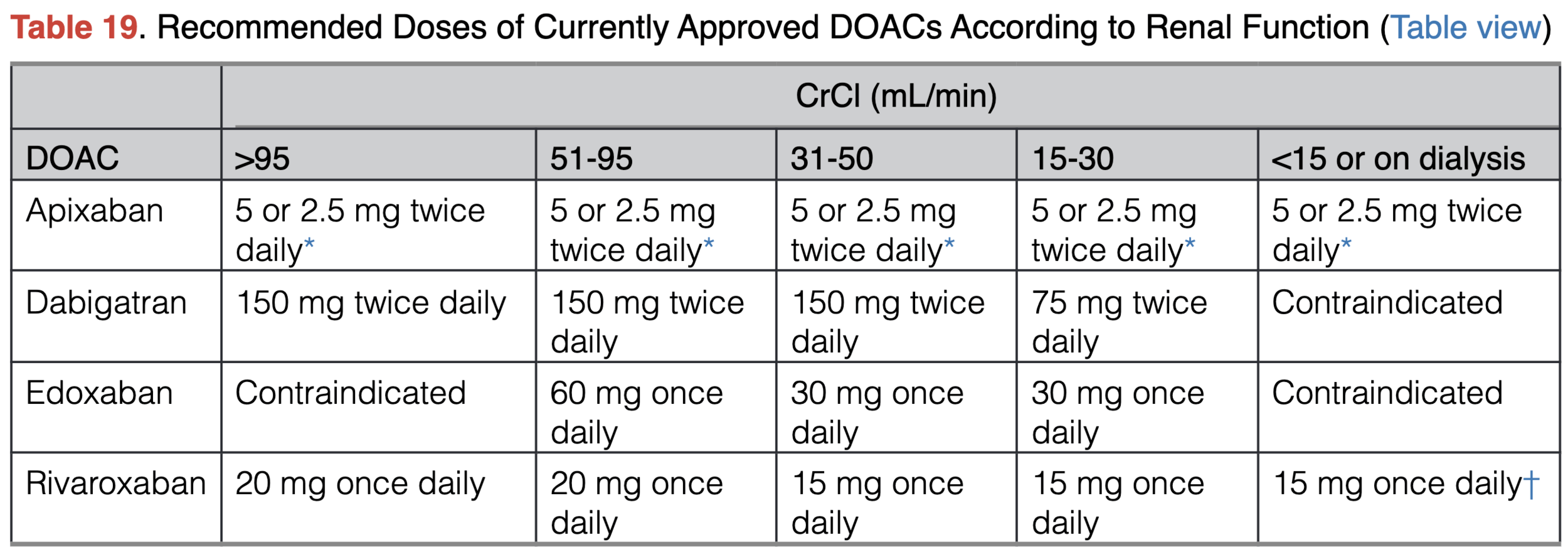
*If at least 2 of the following are present: serum creatinine ≥1.5 mg/dL, age ≥80 y, or body weight ≤60 kg, the recommended dose is 2.5 mg twice daily
Note: would initiate AC CrCl <30 in conjunction with Nephro
By Atul Jaidka
Afib



