
Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
Cardiology Rounds Oct 16, 2024 | Atul Jaidka
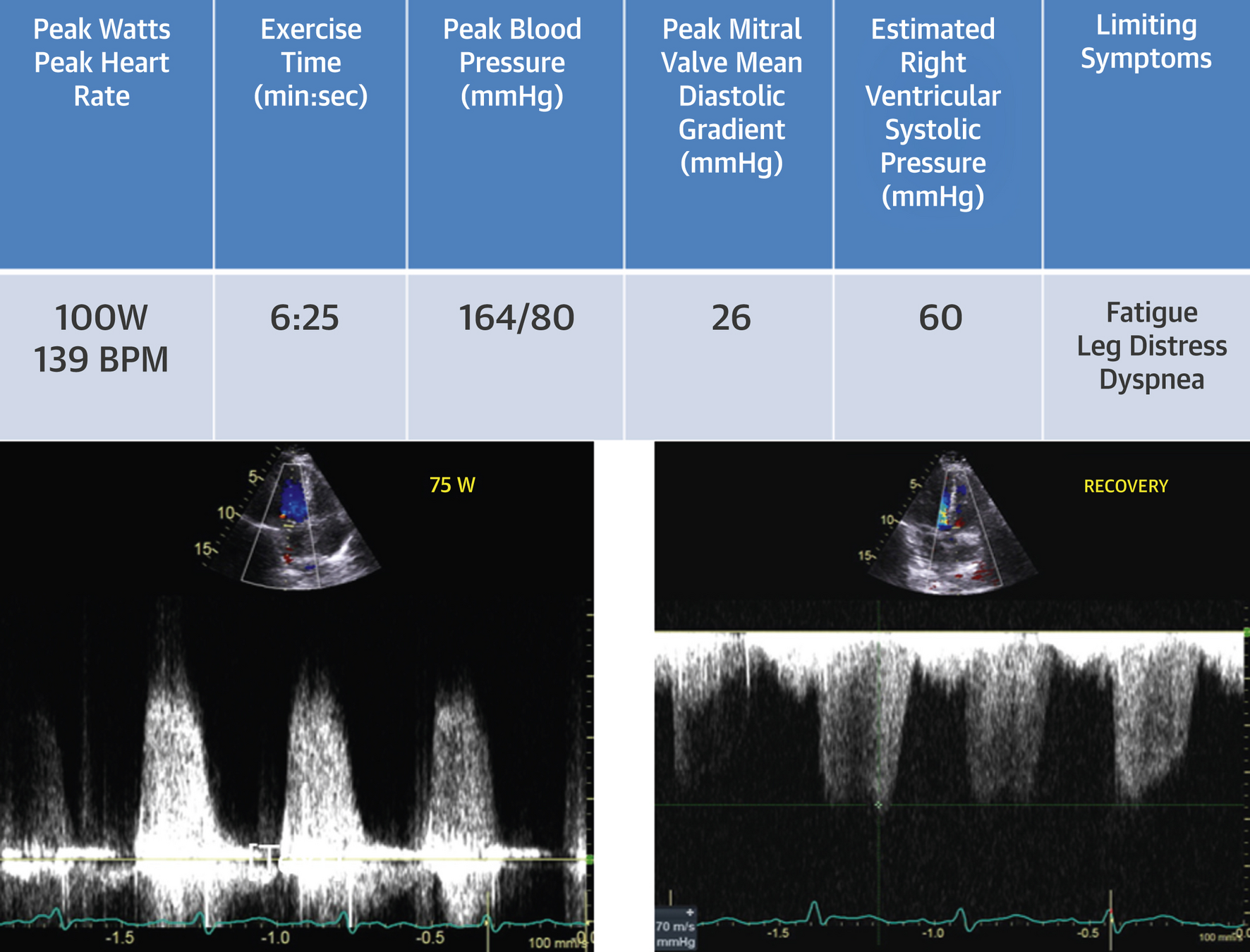
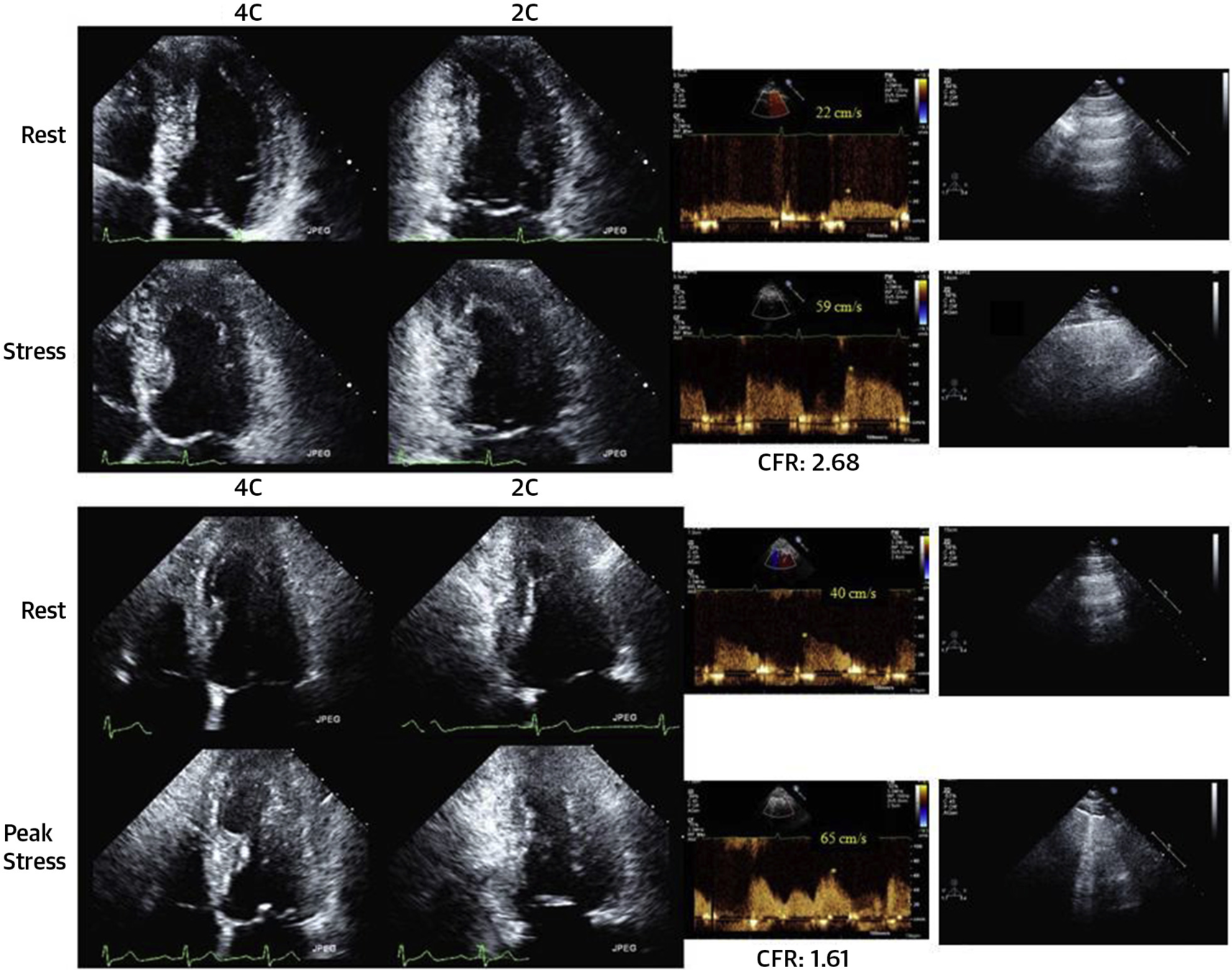
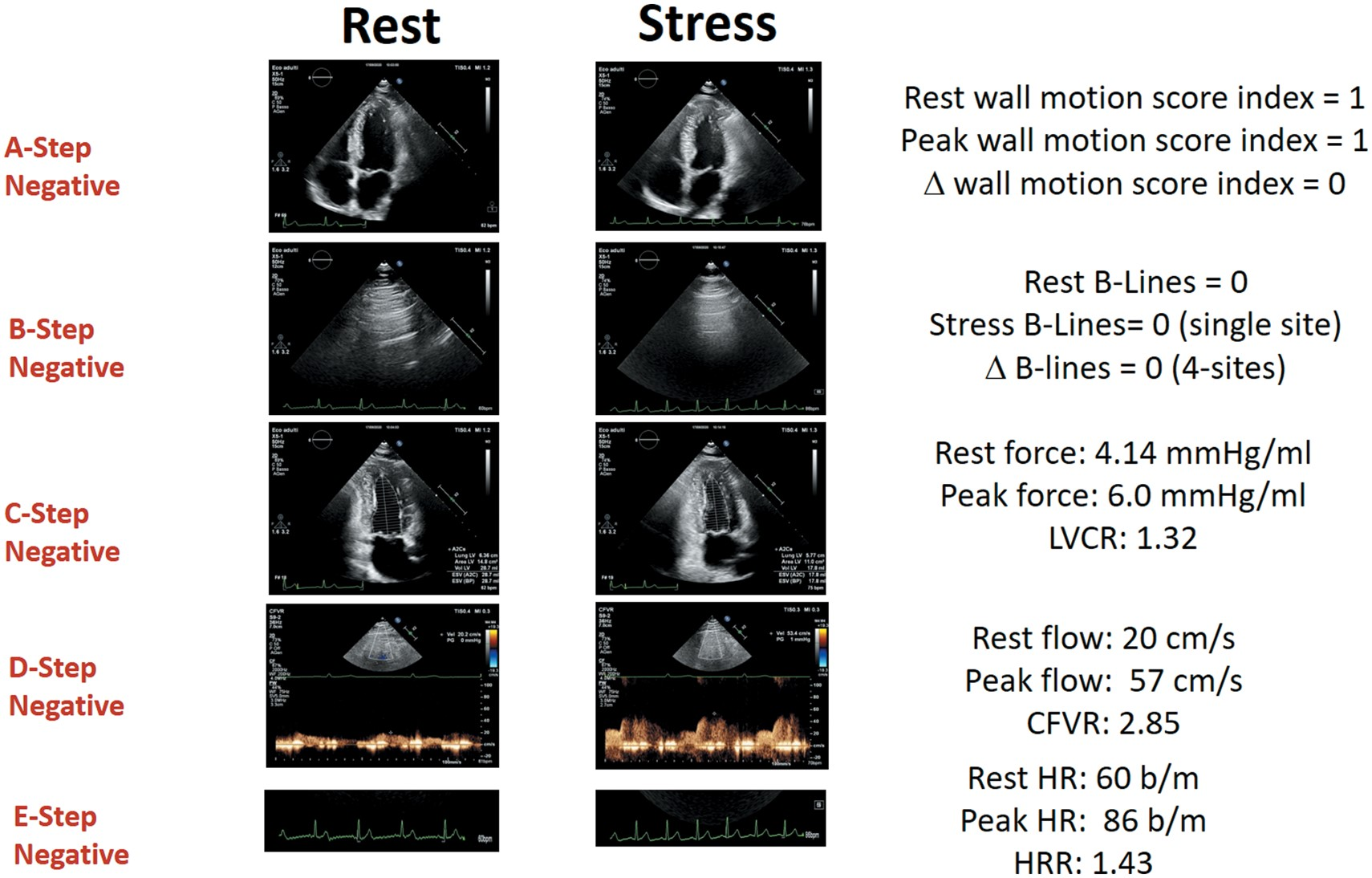
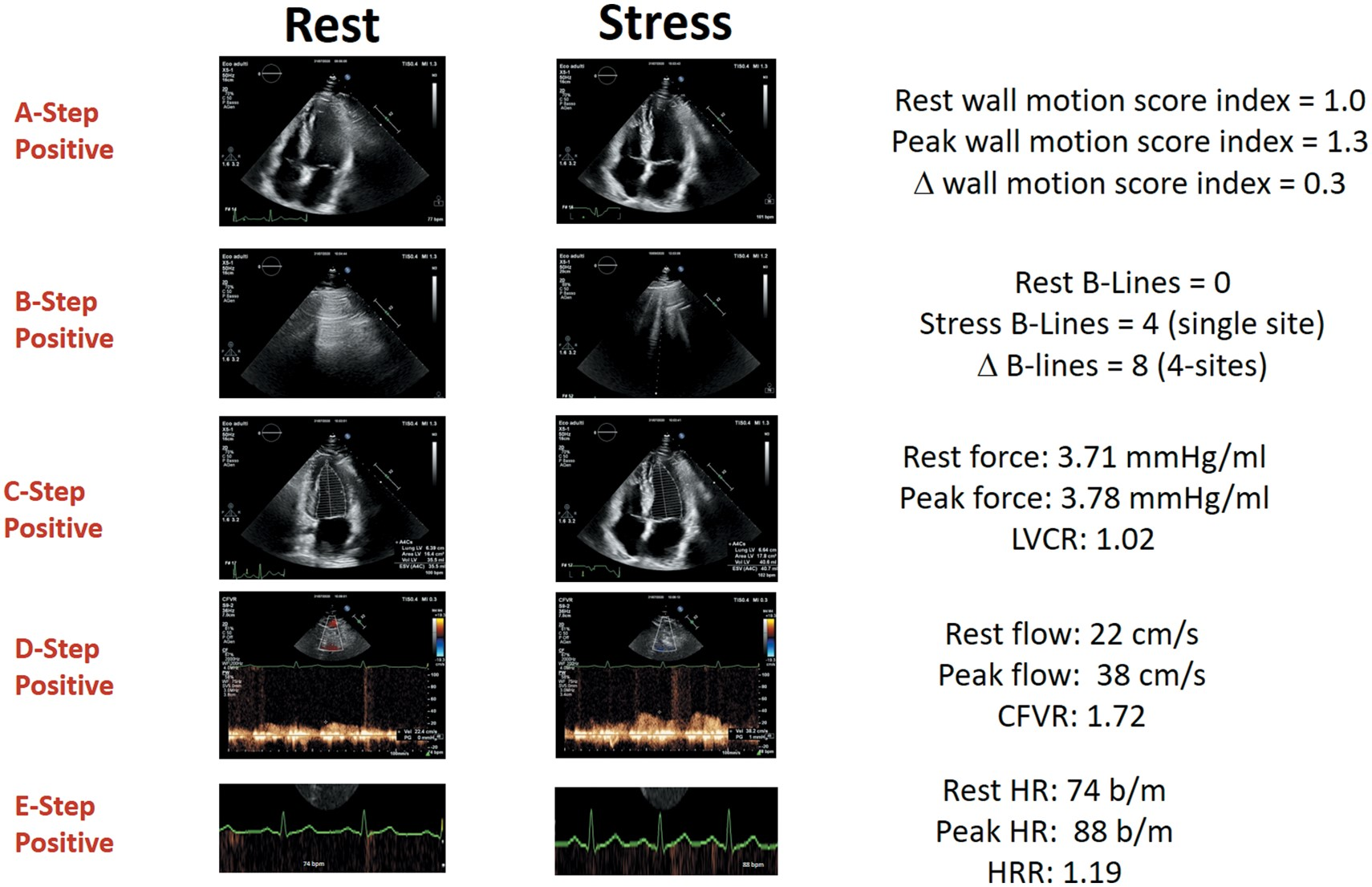
Rest
Post Exercise
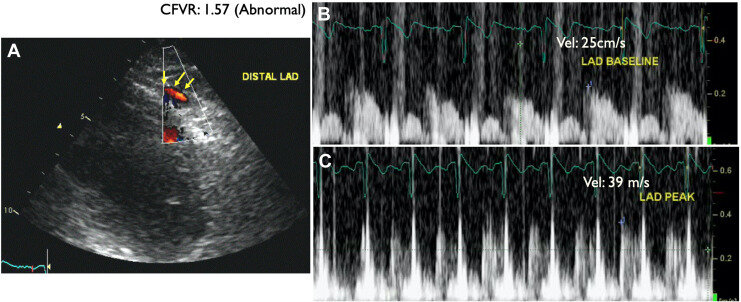
LAD Ischemia
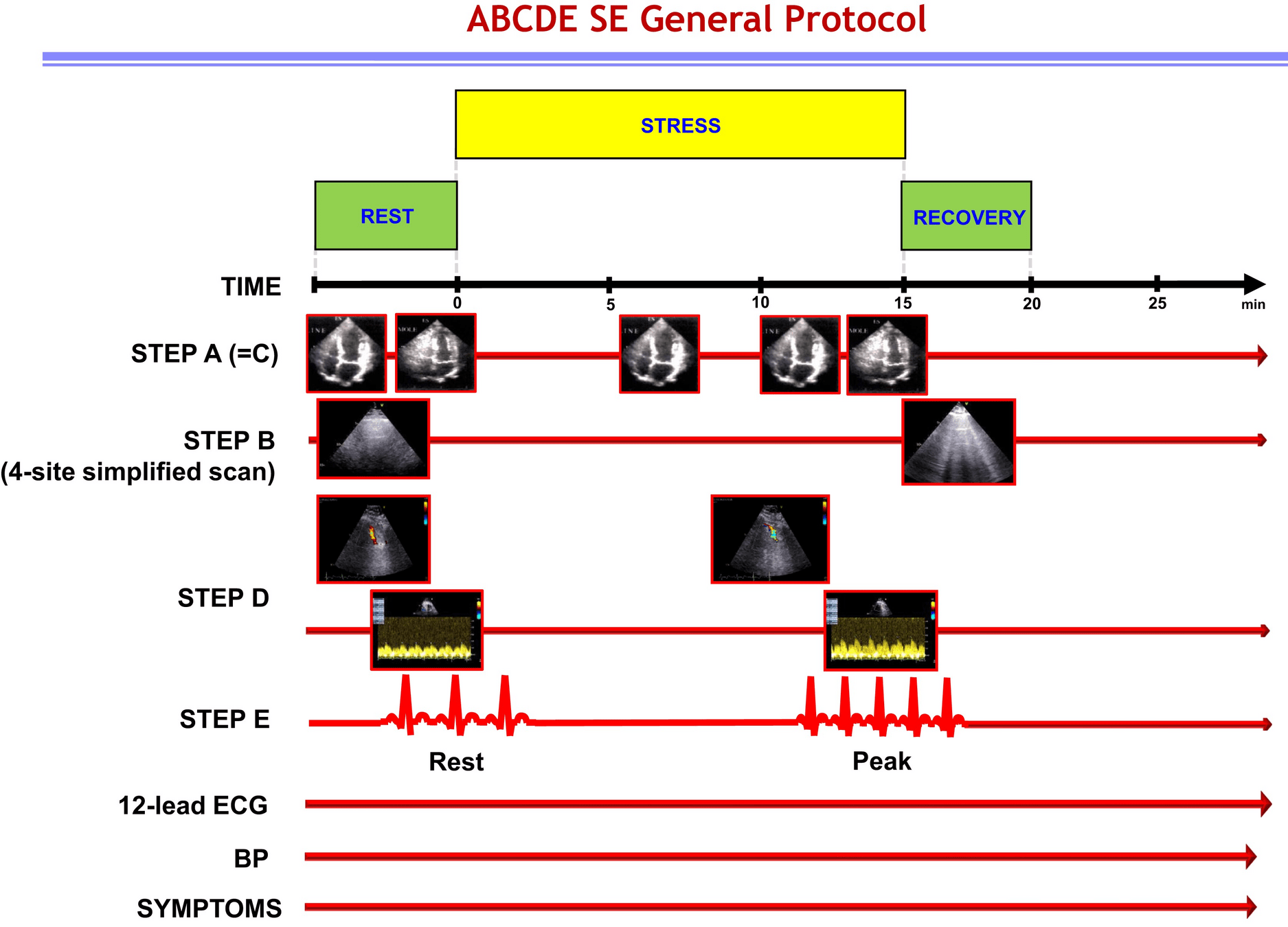
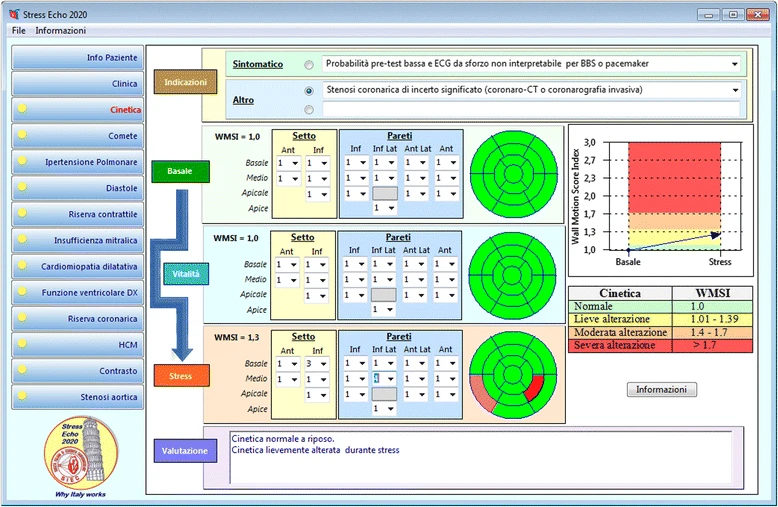
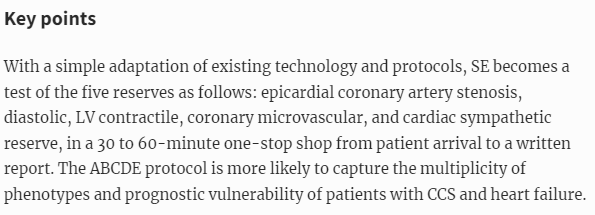
A - Wall motion abnormalities, volumes*
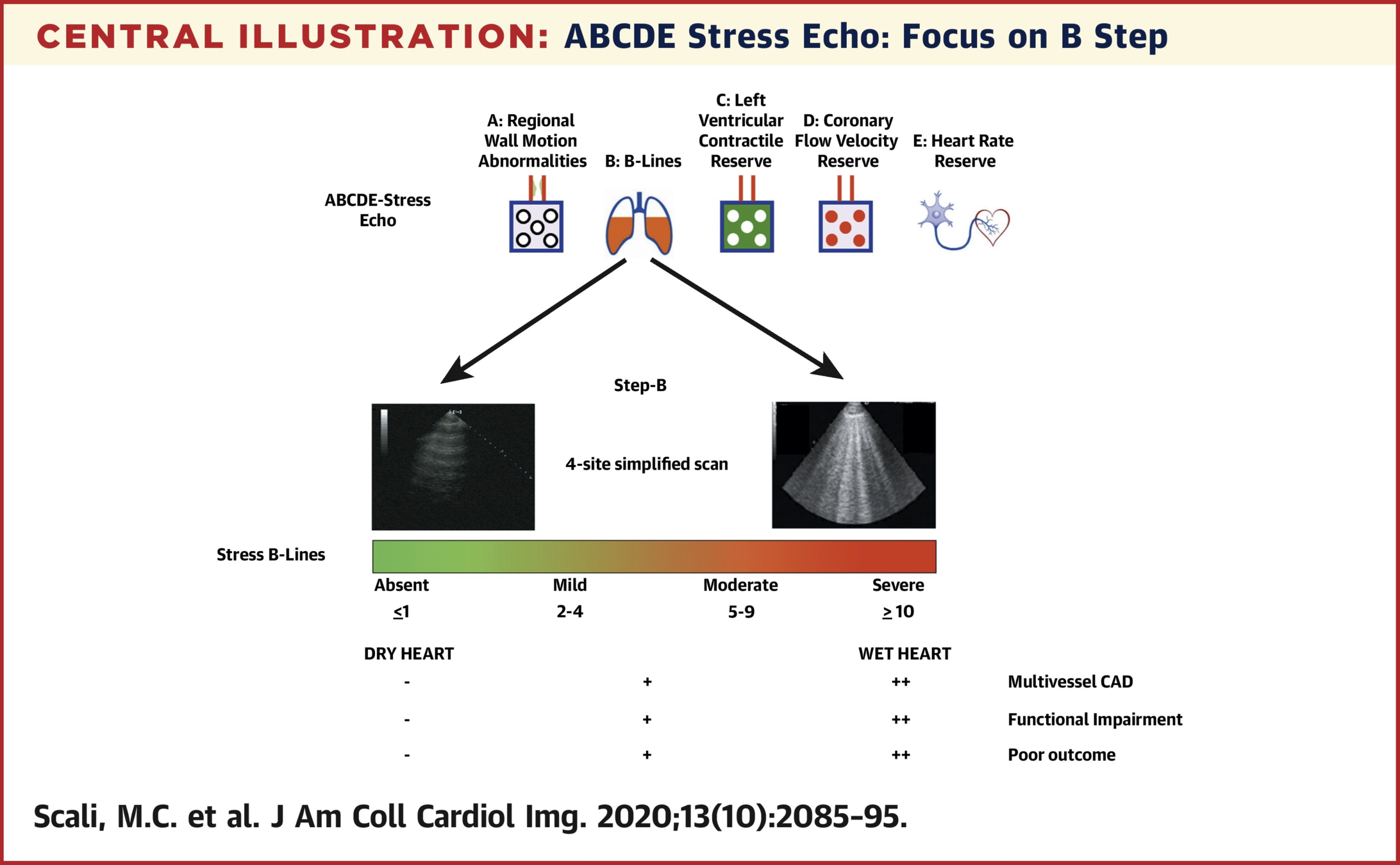
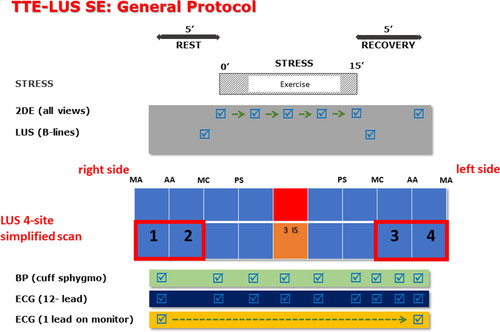
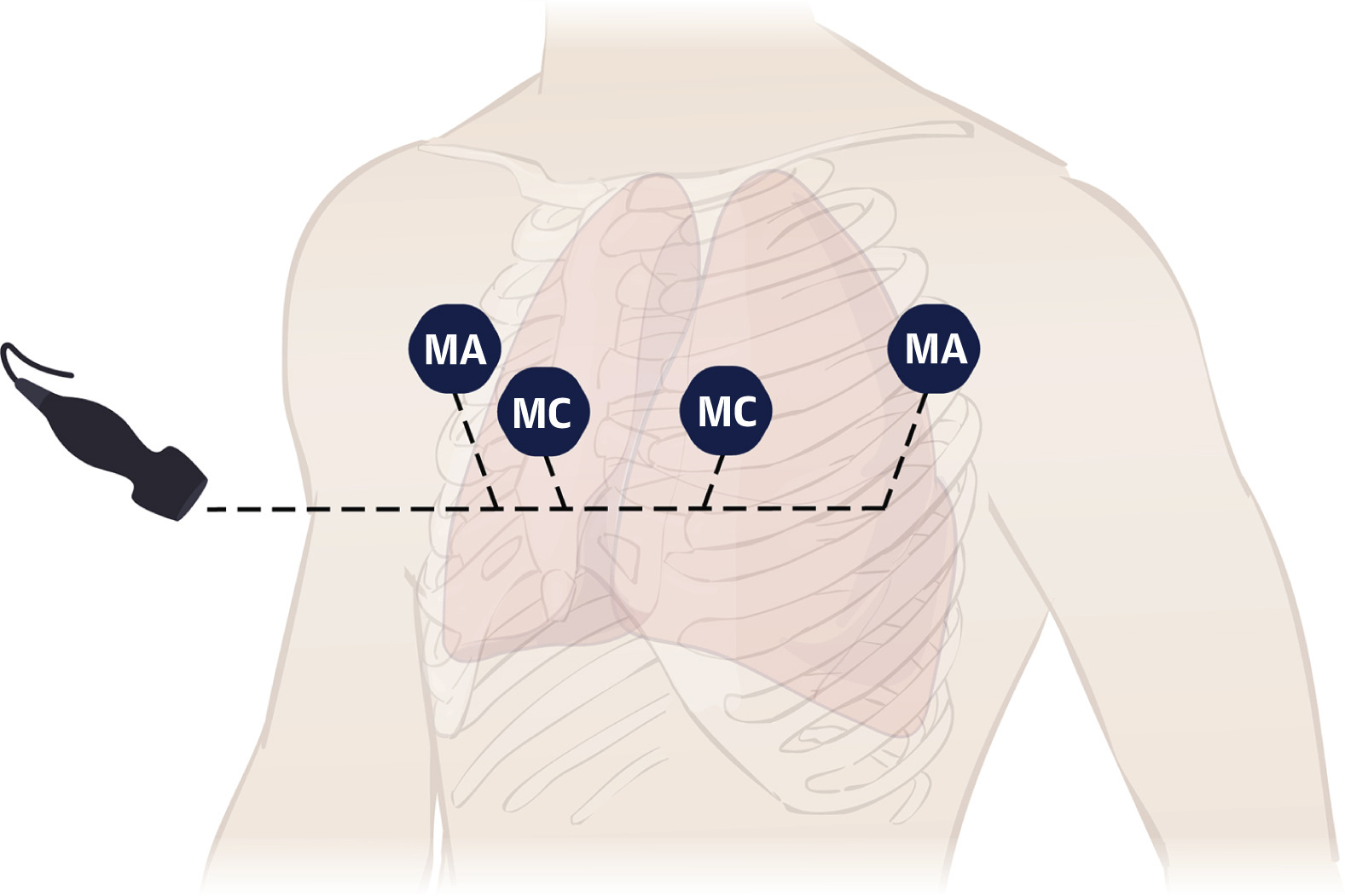
B - B Lines
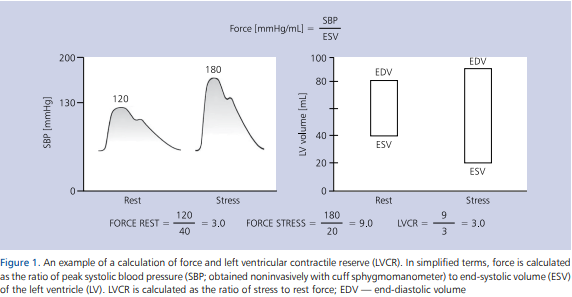
C - Left ventricular contractile reserve*
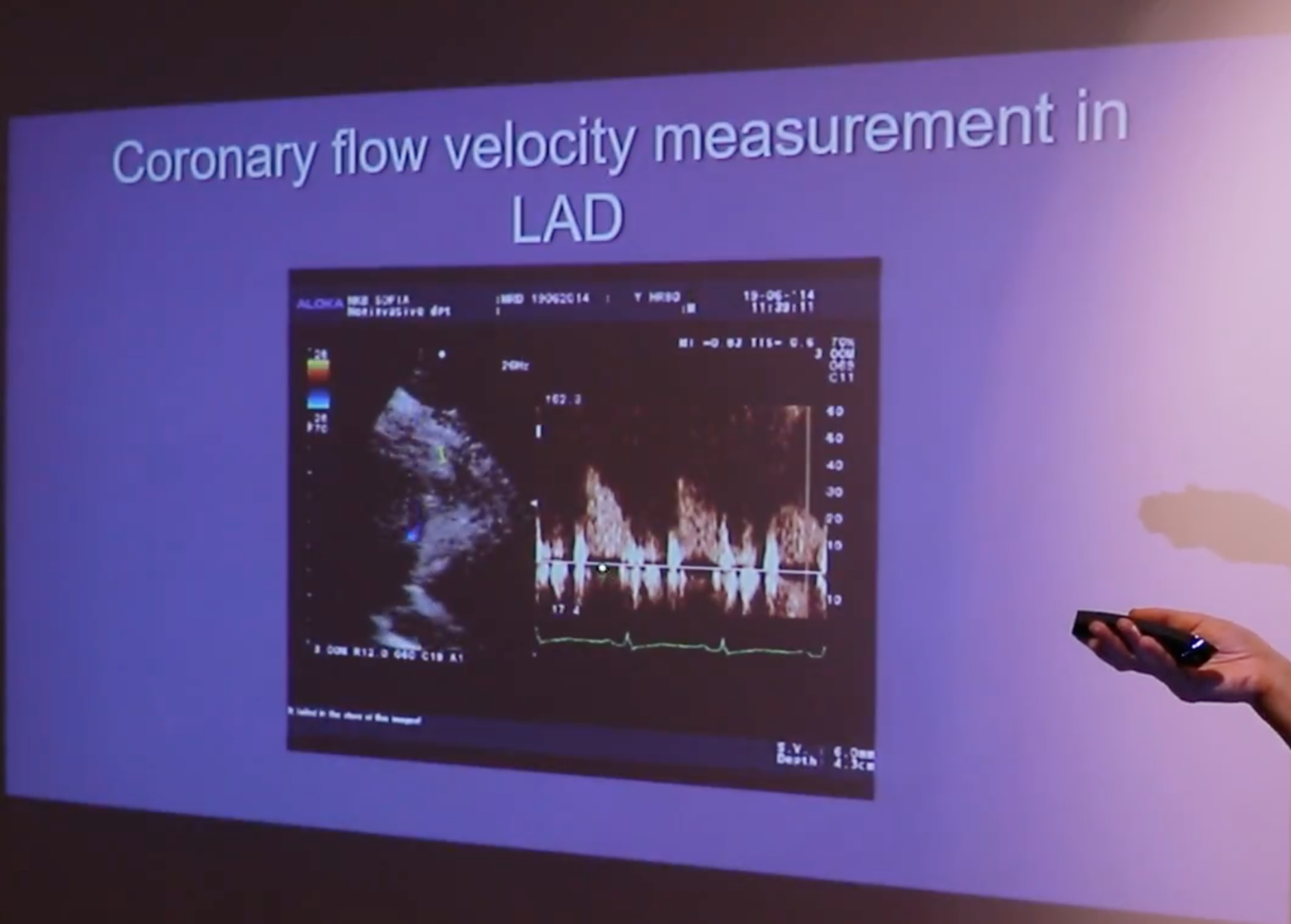
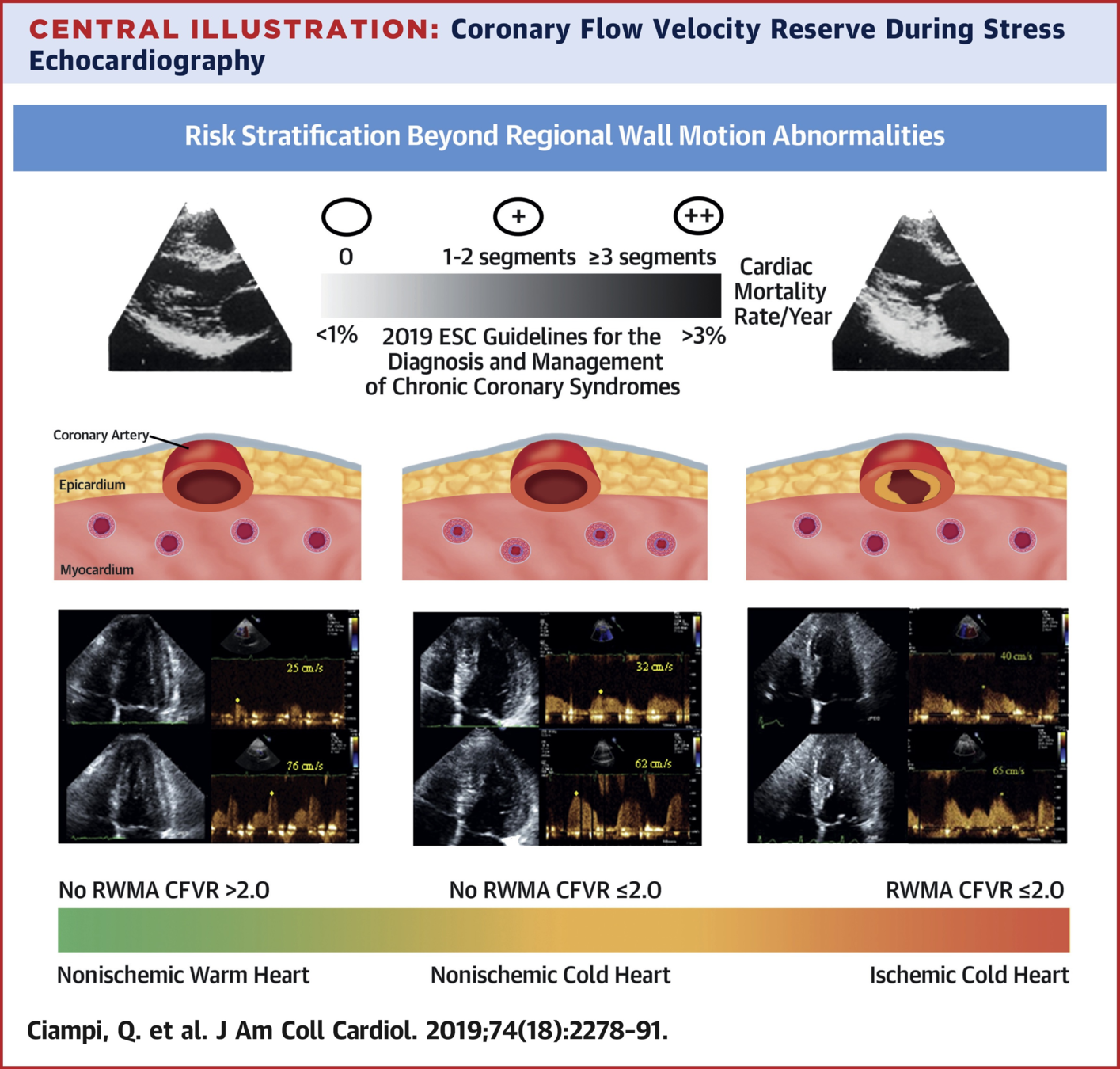
D - Coronary flow reserve
E - Heart rate reserve*
*do not require additional imaging based on current protocol
Scali MC, et al. (2020) Lung Ultrasound and Pulmonary Congestion During Stress Echocardiography. JACC Cardiovasc Imaging 13:2085-95.
Picano E, et al.. Stress lung Ultrasound stress echo2020.2019. Available at https://www.youtube.com/watch?v=BwzgoG15E_A
Scali MC, et al. (2020) Lung Ultrasound and Pulmonary Congestion During Stress Echocardiography. JACC Cardiovasc Imaging 13:2085-95.
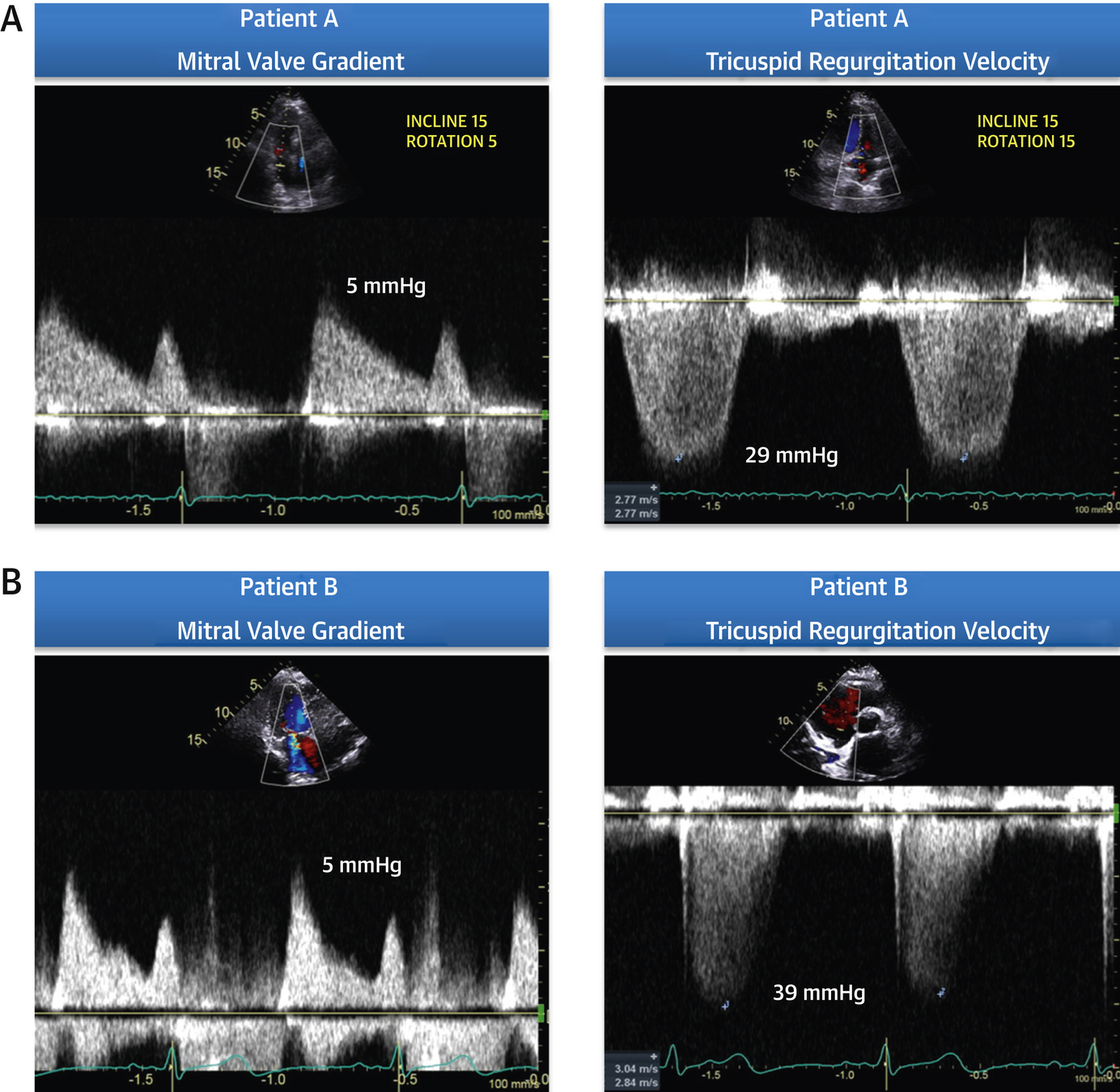
Wiley BM, et al. (2020) Lung Ultrasound During Stress Echocardiography Aids the Evaluation of Valvular Heart Disease Severity. JACC Cardiovasc Imaging 13:866-72.
Wiley BM, et al. (2020) Lung Ultrasound During Stress Echocardiography Aids the Evaluation of Valvular Heart Disease Severity. JACC Cardiovasc Imaging 13:866-72.
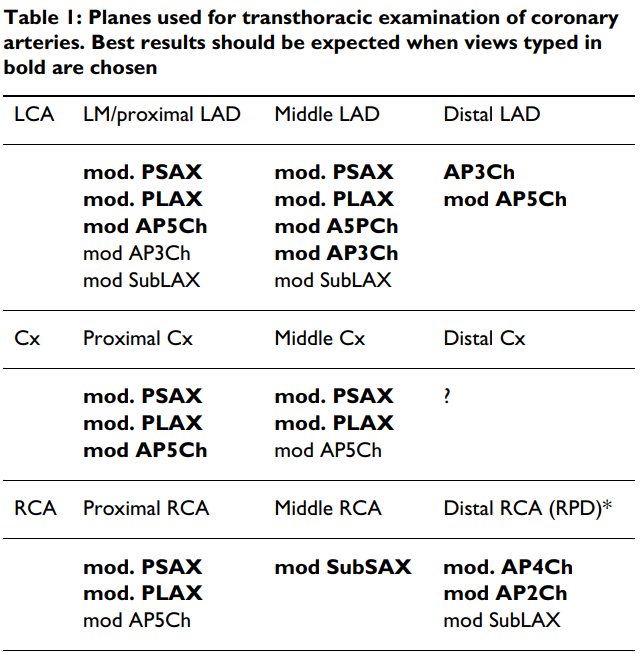
Mod PSAX
Mod PLAX
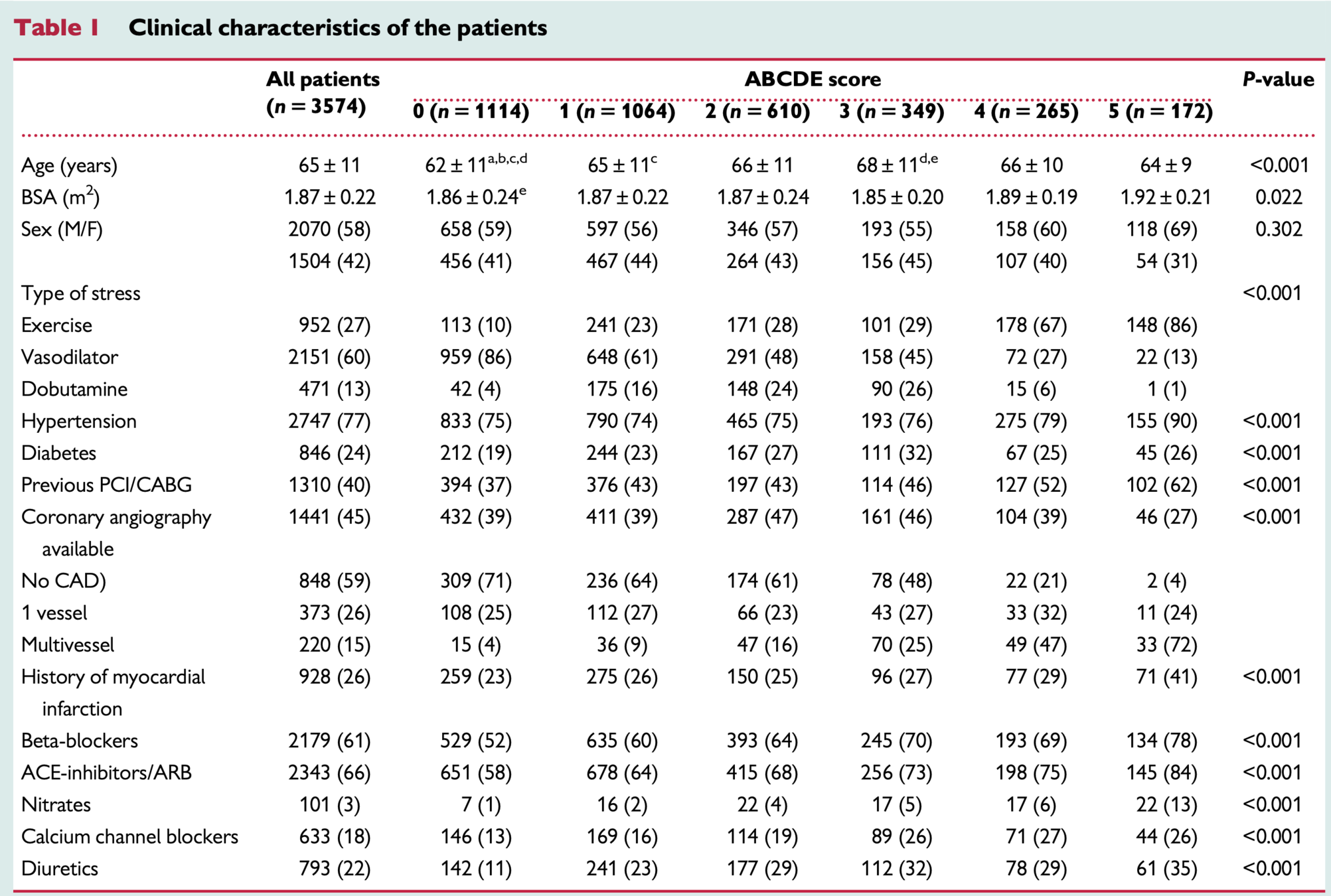
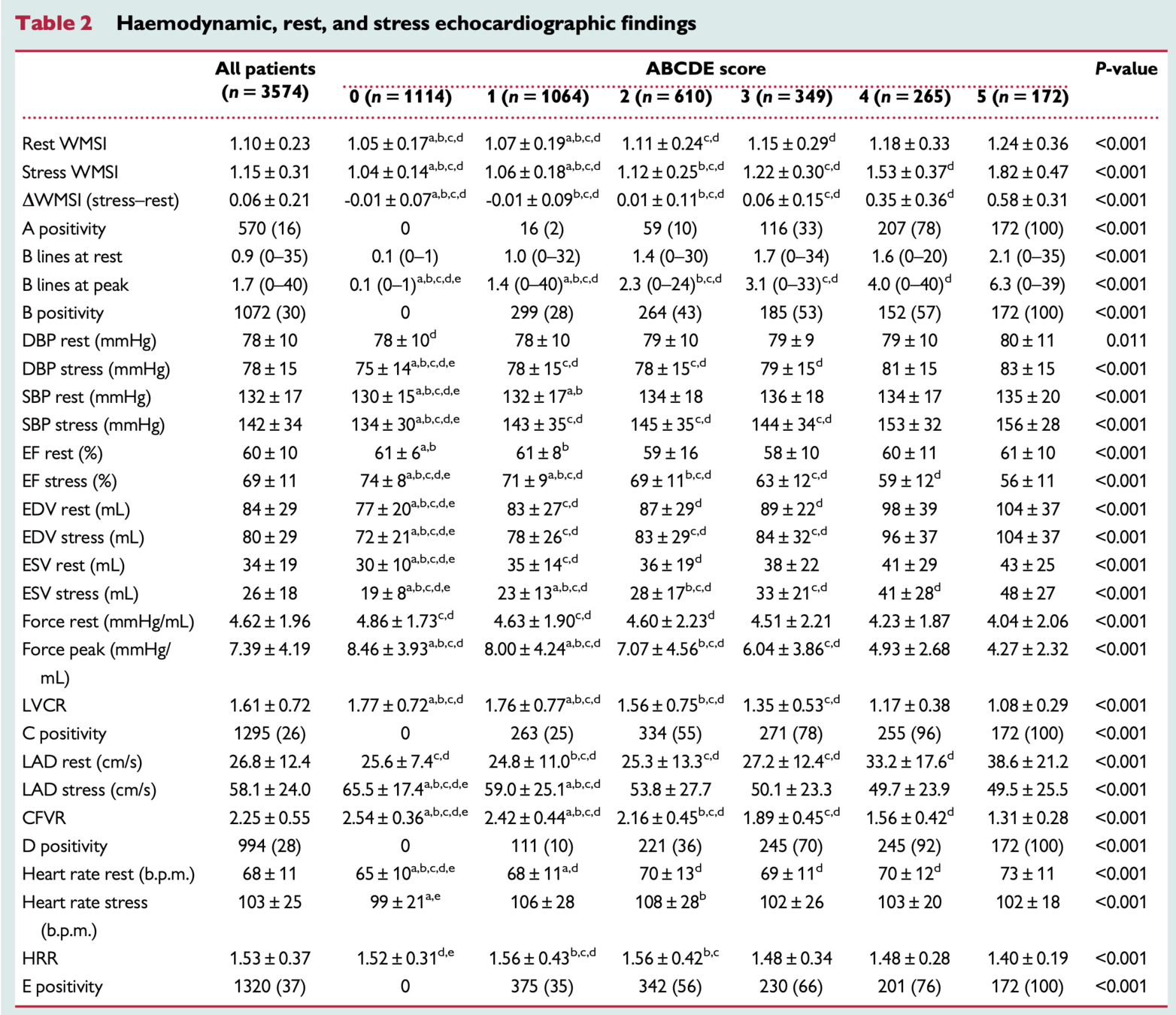
European Heart Journal 2021
Ciampi et al.
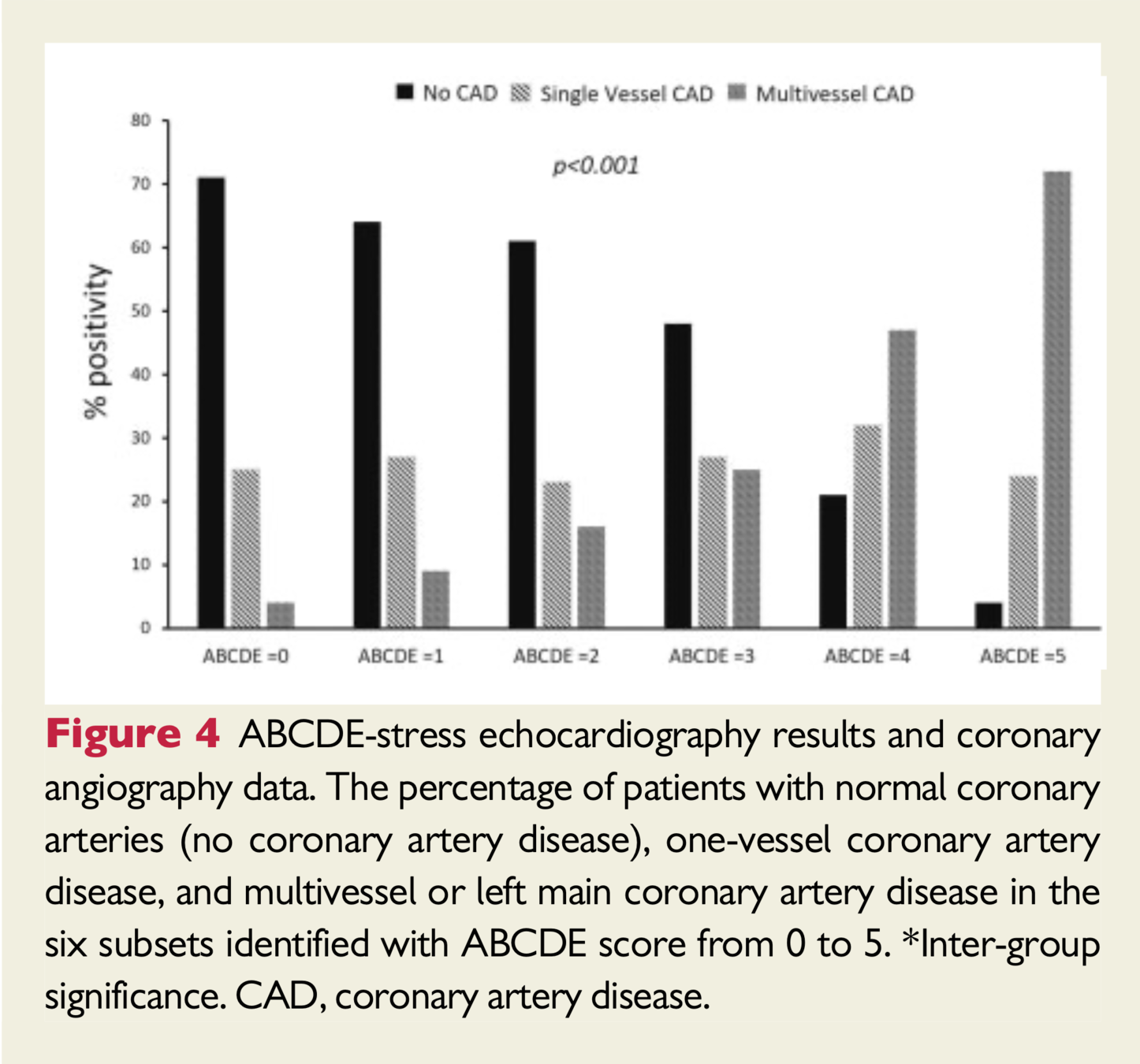
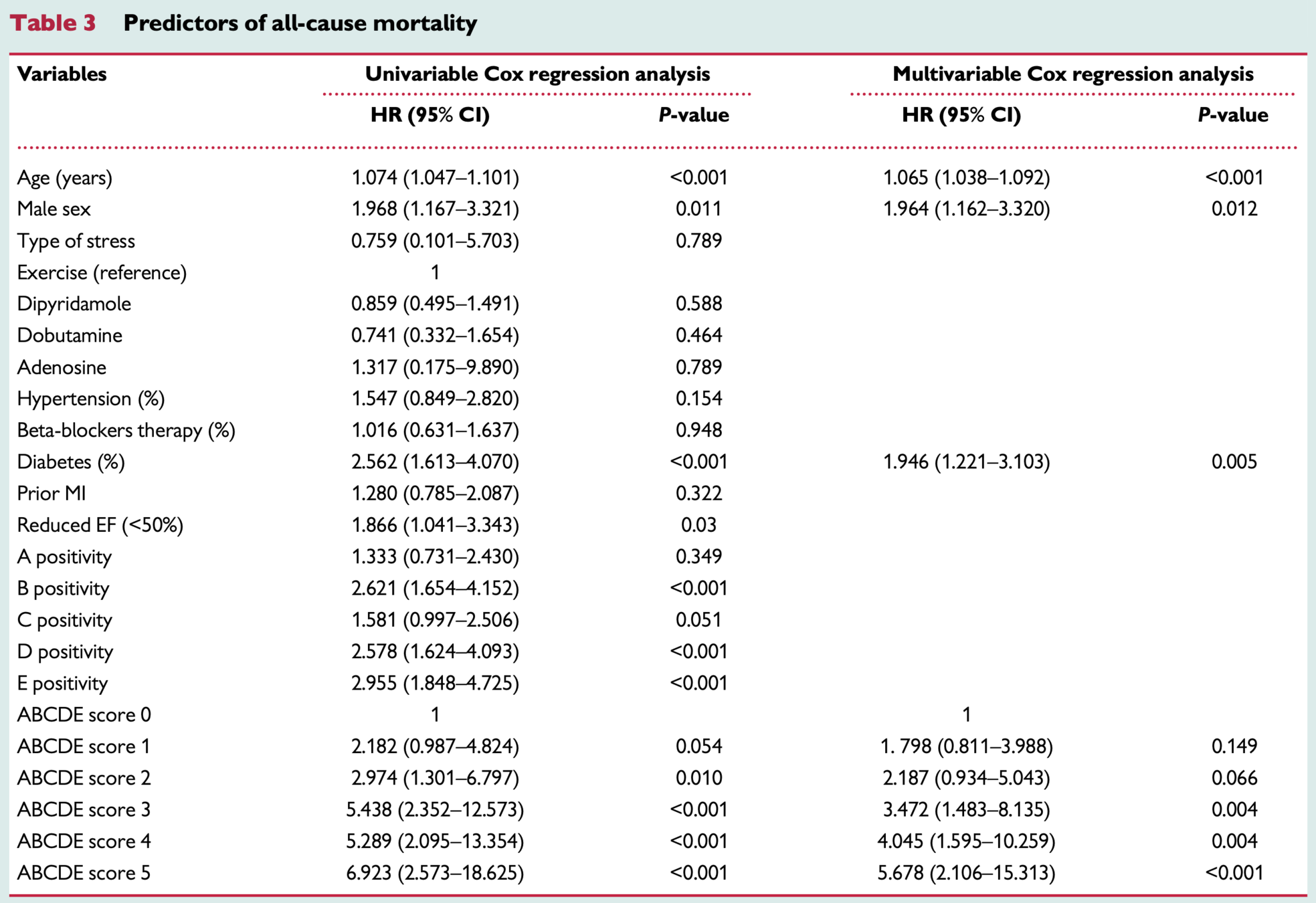
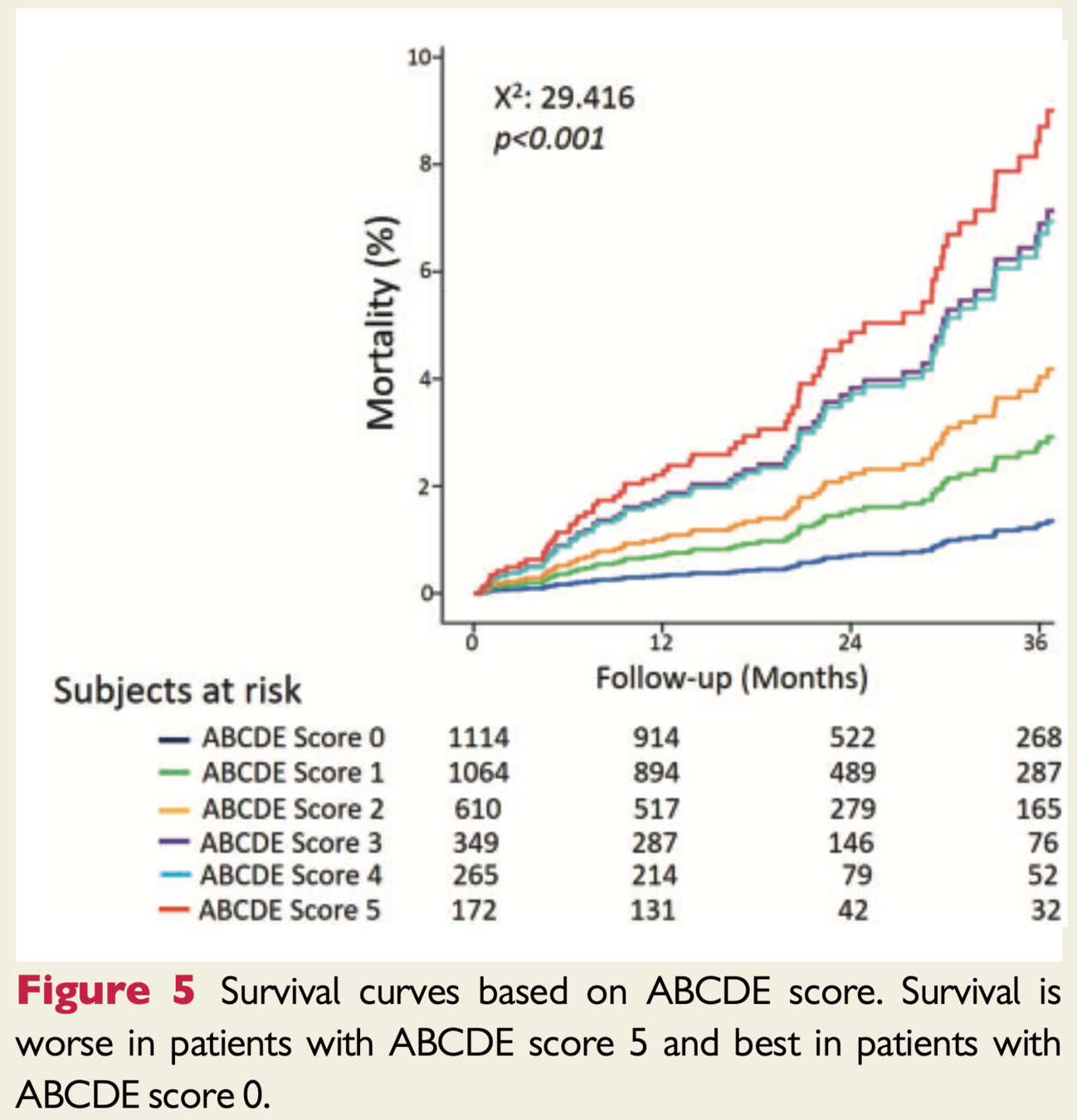
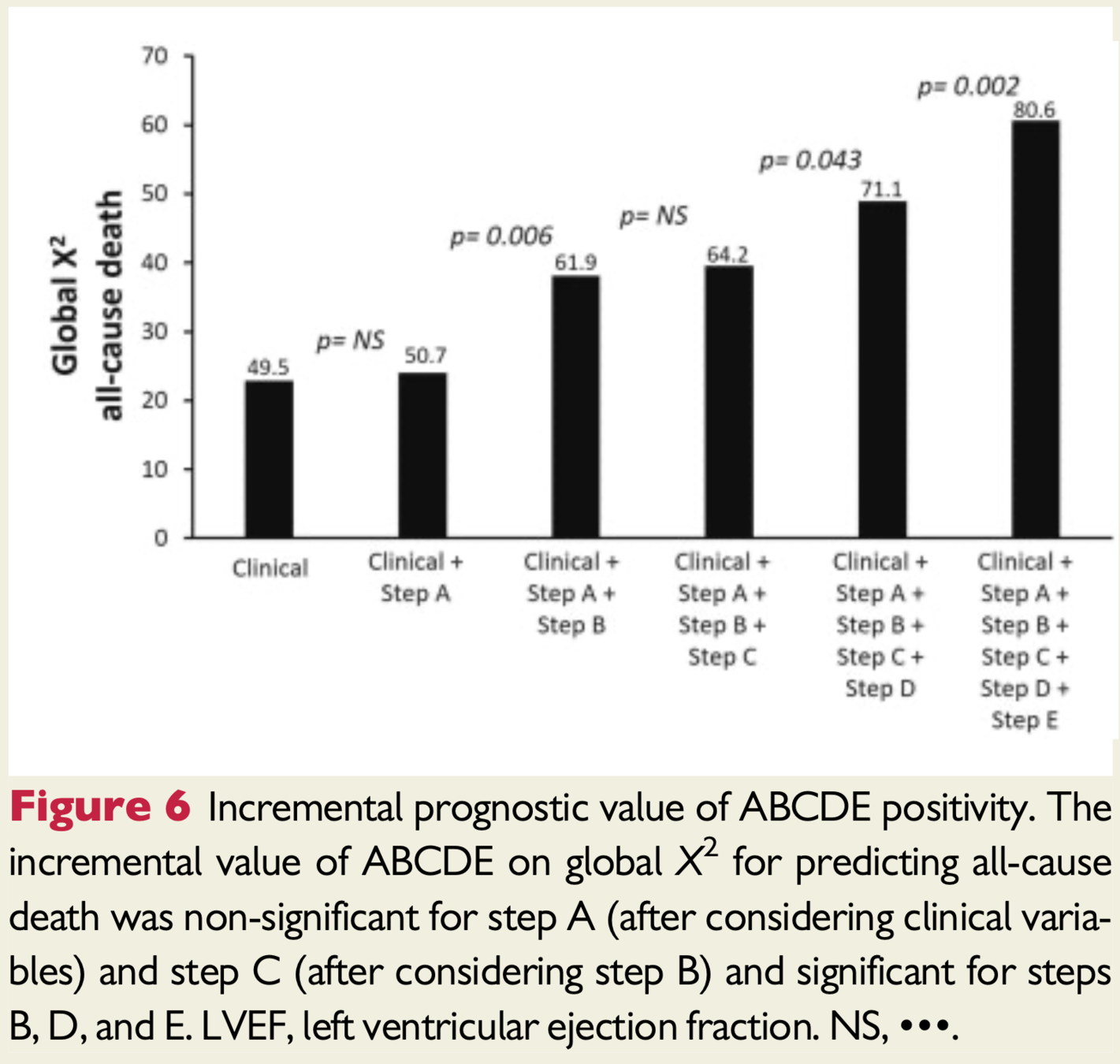
Prognostic value of stress echocardiography assessed by the ABCDE protocol
Treatments potentially titratable to ABCDE risk score
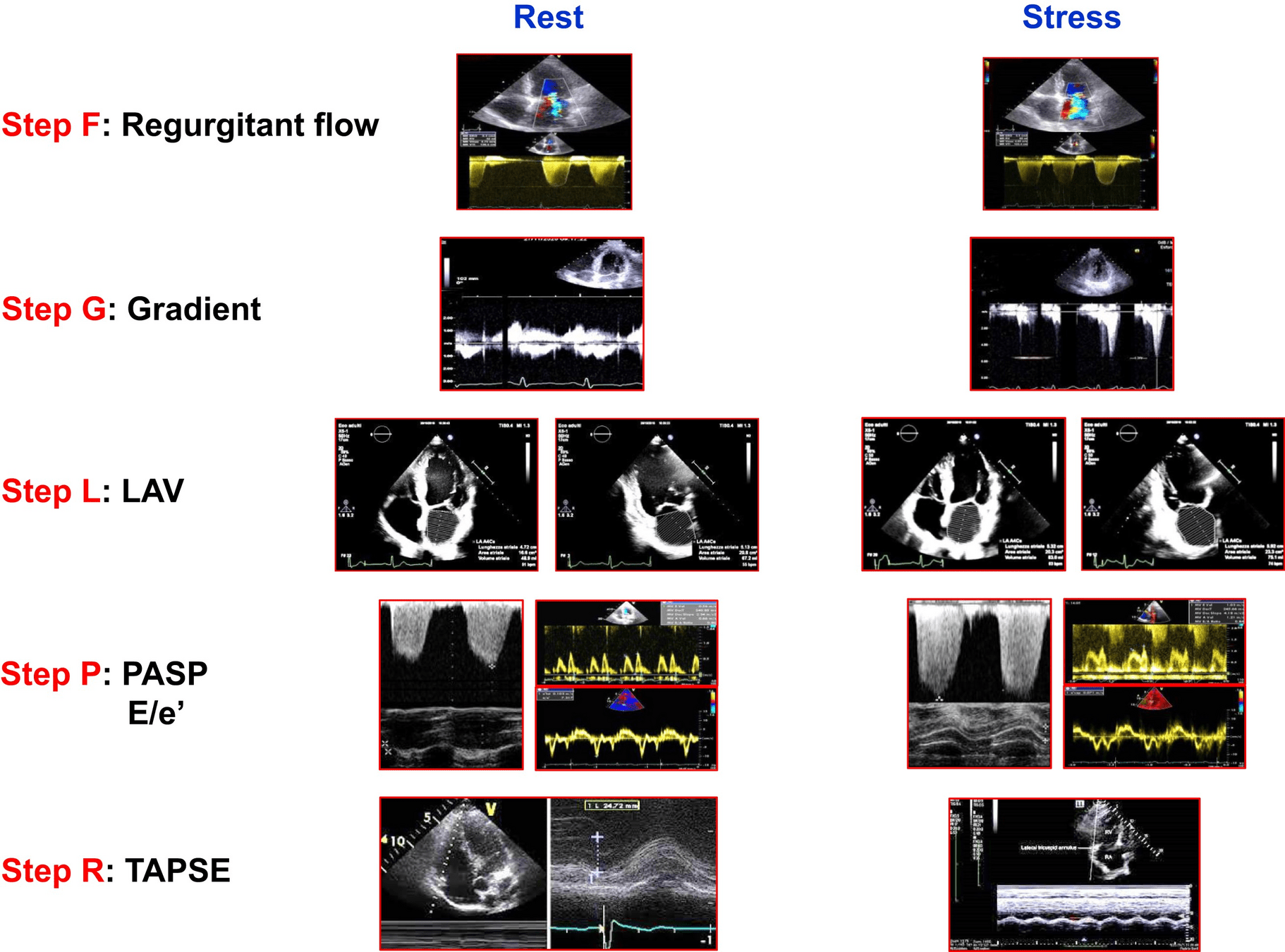
ABCDE + F (regurgitant flow) G (LVOT gradients) L (left atrial volume/function) P ( pulmonary and LV pressures) L (RV function)
ABCDE + F (regurgitant flow) G (LVOT gradients) L (left atrial volume/function) P ( pulmonary and LV pressures) L (RV function)
"The current shift toward using SE protocols with both known and novel parameters is a new frontier. It will be interesting to observe the impact of SE 2020 in shifting practice. There has been a reluctance to “go with the flow” on this side of the Atlantic, but perhaps this will change with clear demonstration of feasibility and incremental value of a multiparametric SE approach, especially in women, who could benefit greatly from a noninvasive, nonionizing assessment of myocardial microvascular integrity."
-Sharon L. Mulvagh (Editorial Comment)
By Atul Jaidka



