Community and Stakeholder Engagement
Catherine W. Striley, Irvin PeDro Cohen, Hui Hu,
Thomas A. Pearson, Linda B. Cottler
External Advisory Committee Meeting
Oct 21, 2016
Innovation of UF Effort
- Engaging, serving and building trust with Florida communities, especially historically underrepresented populations, using a high touch, person-centered approach
- Contributing to the science of community engaged research
- Innovative methods contributing to science and research communities highlighted today:
- HealthStreet
- OCOH
TM
UF CTSI Stakeholder Demographics
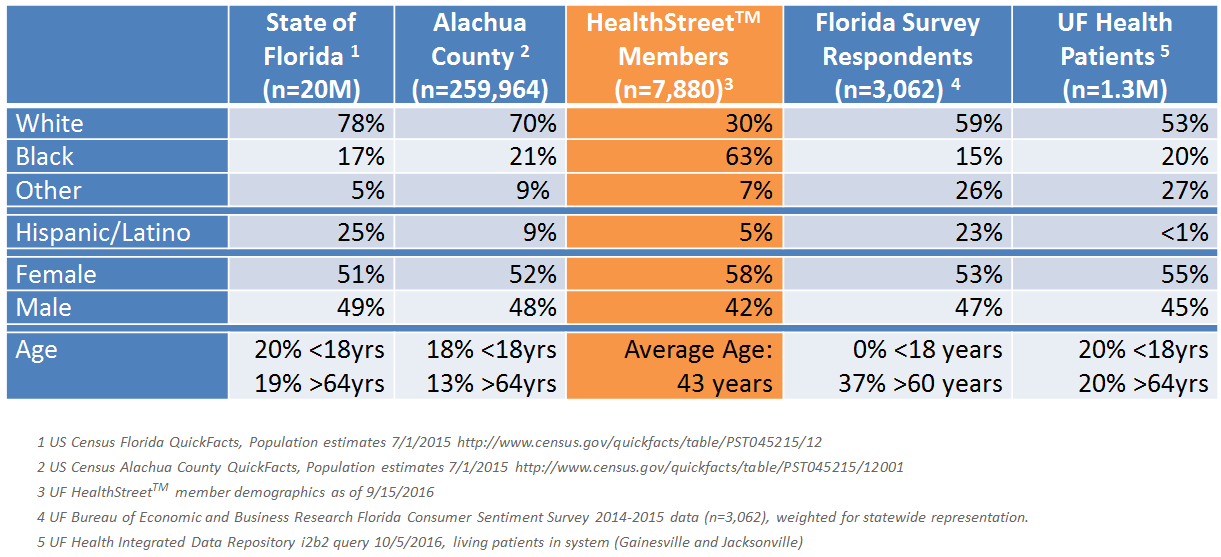
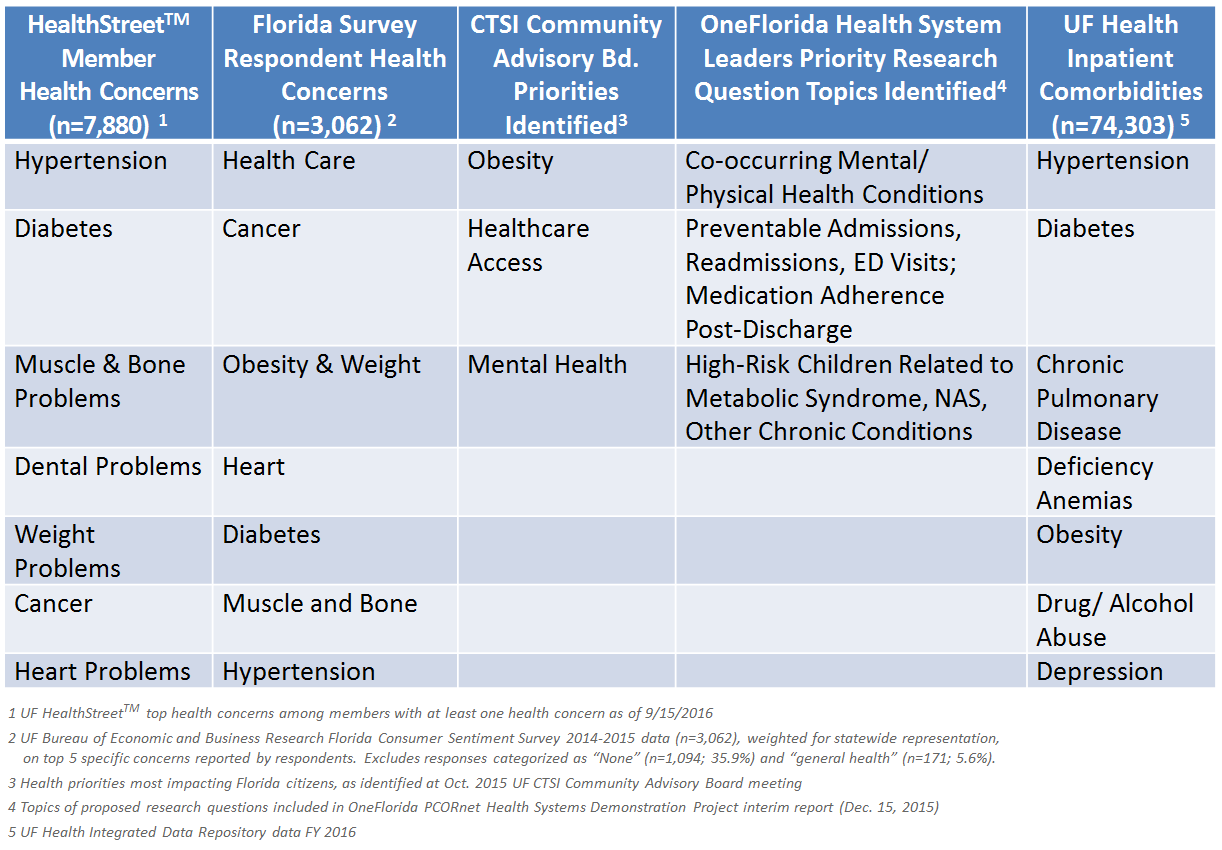
Community Health Concerns Engaging Multiple Stakeholders
2015 EAC Feedback
- Is there an opportunity to assess in more depth the value of HealthStreet to the CTSI, to the communities in which it works (social return on investment), and to research in general?
- How to move HealthStreet to subsequent stages of implementation?
- Can an approach to better integrate the community health needs into the strategic plans for the CTSI and UF Health be developed?
TM
TM




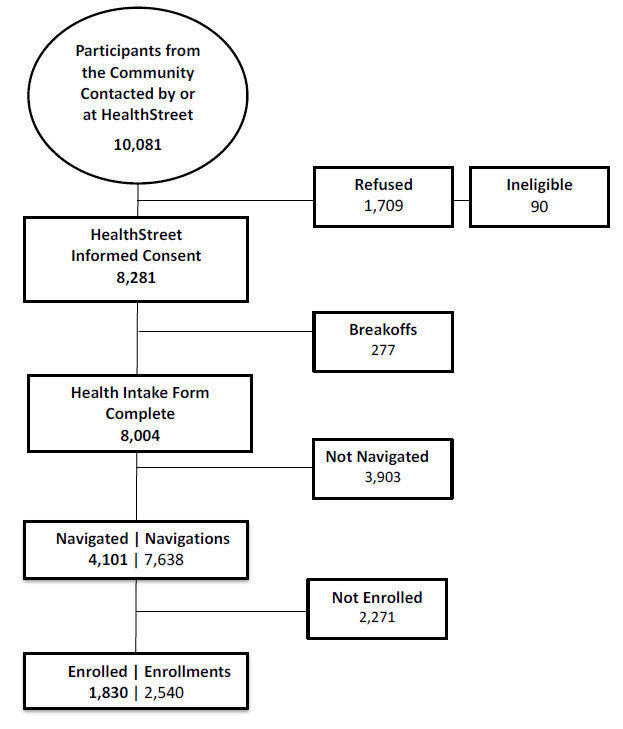
| Recruitment Yield (Completed Informed Consent/Total Contacted Excluding Ineligible) |
82.9% 8,281/9,991 |
| Navigation Yield (Navigated/Completed Health Intakes) |
51.2% 4,101/8,004 |
| Unadjusted Enrollment Yield (Enrolled/Completed Health Intakes) |
22.9% 1,830/8,004 |
| Adjusted Enrollment Yield (Enrolled/Navigated) |
44.6% 1,830/4,101 |
Effectiveness of the Community Navigation Model
Data last updated: 10/9/2016
$398 per enrollment
TM
TM
Making Research Matter
Introduction/Aim
- Racial and ethnic minorities are not likely to be enrolled in research
- Despite demonstrated willingness to participate - Where does the disconnect between community member desire for research participation and actual research participation come from?
Results
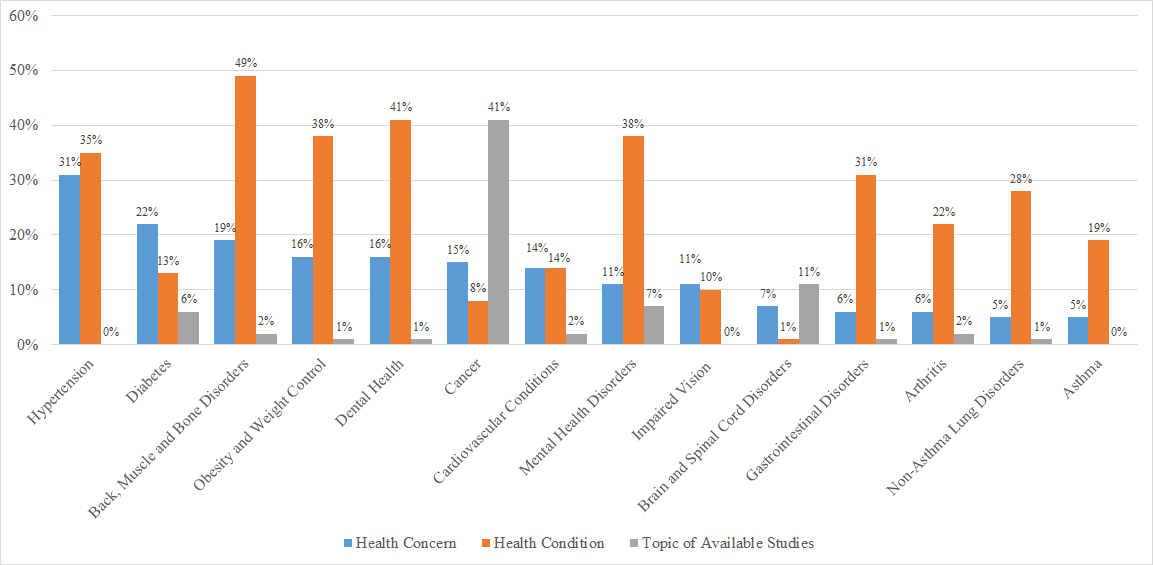
- Substantial discordance between community member health conditions/concerns and topics of available studies for them to participate in (see figure in next slide)
Discussion
- The health conditions and health concerns of the community provide a wide range of public health relevant topics
- Faculty research interests may not be aligned with community needs

Corbie-Smith G, Moody-Ayers S & Thrasher AD. Closing the circle between minority inclusion in research and health disparities. Arch. Intern. Med. 164, 1362–1364 (2004).
Fisher, J. A. & Kalbaugh, C. A. Challenging Assumptions About Minority Participation in US Clinical Research. Am. J. Public Health 101, 2217–2222 (2011).
Cottler, L. B. et al. Community Needs, Concerns, and Perceptions About Health Research: Findings From the Clinical and Translational Science Award Sentinel Network. Am. J. Public Health 103, 1685–1692 (2013).
Crooke H, Kwiatkowski E, Nelson DR, Cottler LB, Striley CW. Making Research Matter: Consequential Public Health as a Framework for Disparities in Enrollment into Health Research. Journal of Epidemiology and Community Health, under review.
Comparison of Health Concerns and Conditions from Community-recruited participants, and Available, Openly Recruiting Health Research Studies
(sorted in descending order of health concern prevalence)*
*Health Concern percentages calculated out of the number of HealthStreet members who provided at least one health concern as of March 2016 (n=6,724);
Health Condition percentages calculated out of the total HealthStreet member population with completed Health Intake Forms as of March 2016 (n=7,354);
Research Study topic percentages calculated out of all openly recruiting health research studies available to HealthStreet members as of March 2016 (n=90)
TM
TM
TM
Saturation Map of HealthStreet
TM
Neighborhood Deprivation Index (NDI)
NDI was generated based on block group-level SES Indicators from the 2010-2014 American Community Survey:
- Poverty: % HHs in poverty, % HHs earning <$30,000/year, % HHs with no vehicle
- Occupation: % males(females) in management or professional occupations
- Housing: % rented housing, % vacant housing, % renter/owner costs>50% income, median home values
- Employment: % unemployed, % males no longer in work force
- Education: % <high school education
- Racial composition: % non-Hispanic blacks
- Residential stability: % in same residence in the last year, % residents ≥65 years old
74% HealthStreet participants are from areas with high deprivation*
Messer, Lynne C., Barbara A. Laraia, Jay S. Kaufman, Janet Eyster, Claudia Holzman, Jennifer Culhane, Irma Elo, Jessica G. Burke, and Patricia O’campo. "The development of a standardized neighborhood deprivation index." Journal of Urban Health 83, no. 6 (2006): 1041-1062.
* Neighborhoods with NDI higher than the state median (-0.25)
TM
Effectiveness of the Community Navigation Model
Hot Spots
Cancer (7.8%)
Hypertension (35.0%)
Diabetes (13.2%)
Hot Spots
Obesity (38.3%)
Depression (26.8%)
Past Month Use of Prescription Opioids (13.7%)
HealthStreet Frequent ED Utilizers
- Characterized as ≥ 2 visits in the past 6-months
- Super-utilization is generally associated with:
- Age- young adults and seniors
- Females
- Racial/ethnic minorities
- Lower rates of employment
- Higher rates of poverty
- Less education
- Medicare or Medicaid coverage - Between 4.6 to 8.0% of ED users are super-utilizers
- These individuals account for between 21 to 28% of all visits - After controlling for age and gender, men with 3 – 5 chronic diseases had 6.33 AOR and women with 3 – 5 chronic diseases 3.49 AOR as those with no chronic diseases. Significant AORs remained after adjusting for age, gender, depression, marital status, employment status and food insecurity (4.98 AOR and 2.49 AOR respectively)
LaCalle E, Rabin E. Frequent users of emergency departments: the myths, the data, and the policy implications. Annals of emergency medicine. Jul 2010;56(1):42-48.
Vinton DT, Capp R, Rooks SP, Abbott JT, Ginde AA. Frequent users of US emergency departments: characteristics and opportunities for intervention. Emergency medicine journal : EMJ. Jan 28 2014.
Milani S, Crooke H, Cottler LB, Striley CW. Sex differences in frequent ED use among those with multimorbid chronic disease. American Journal of Emergency Medicine. In Press. Oct 2016; http://dx.doi.org/10.1016/j.ajem.2016.07.059
TM
Involvement of CAB in These Efforts
- Help the CTSI prioritize research to include special populations and address community health concerns
- Co-host one of HealthStreet's national Our Community, Our Health meetings (a national CTSA town hall CAB meeting)
- Multiple CTSA CABs partnering
- Idea initiated through the CTSA PACER group (Eder, Cottler co-chairs)
- Serve as a stakeholder for CTSI evaluation and strategic planning, including representation on the CTSI Steering Committee
Process of Developing Conscientious Constituents
Rather than a focus on patients who are adherent, we want to participate with people in a process of developing conscientious constituents
- Get to point where know what you know
- Own it
- Become your own currency
- Develop that currency around your conditions
- Find an equitable stake
-
Activate as a participant in a solution model
Sixth National Our Community, Our Health: May 2016
-
Topic: Mental Health Care
-
Partnering Institution: University of California Davis Center for Reducing Health Disparities
-
Featured Speakers: Charles Casey, Dr. Hendry Ton, Jessica Cruz, Dr. Sergio Gaxiola-Aguilar
-
Outcome: One of the first OCOH events to be hosted by another CTSA institution



Diverse populations
Outcomes that matter
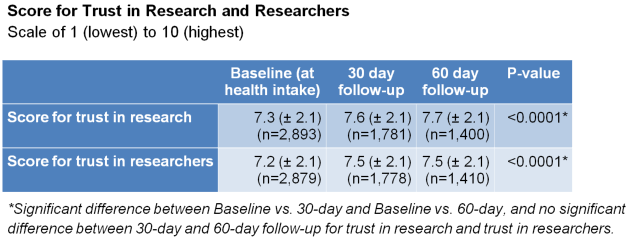
Increased trust in research enterprise
Cost effective enrollments
More voices heard
Person-centered, data-driven, service-oriented
Clinically integrated
Summary
Community and Stakeholder Engagement
By Hui Hu
Community and Stakeholder Engagement
External Advisory Committee Meeting, Oct 21, 2016



