Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
| Atul Jaidka |
Normal Anatomy
will skip, covered recently
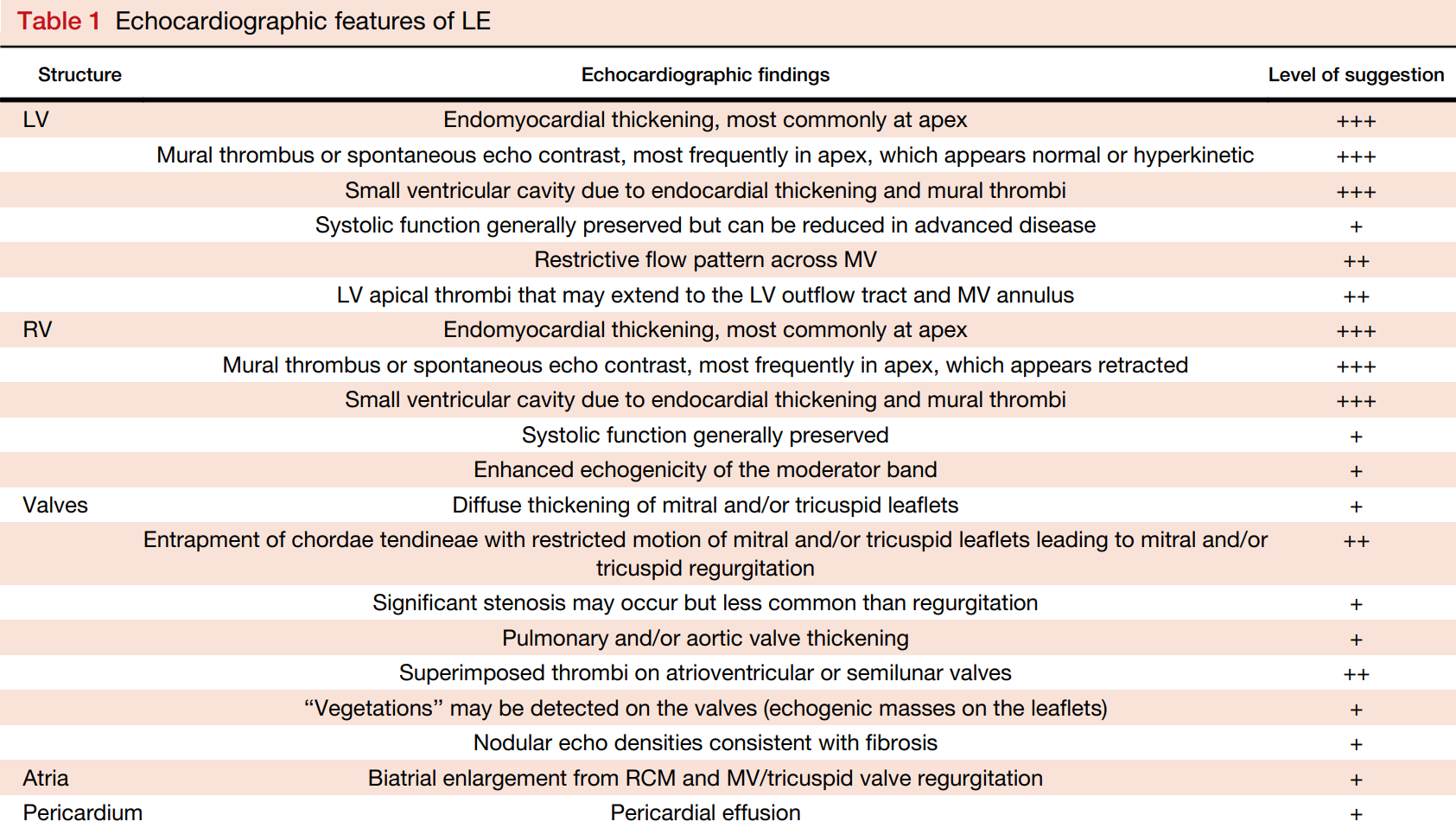
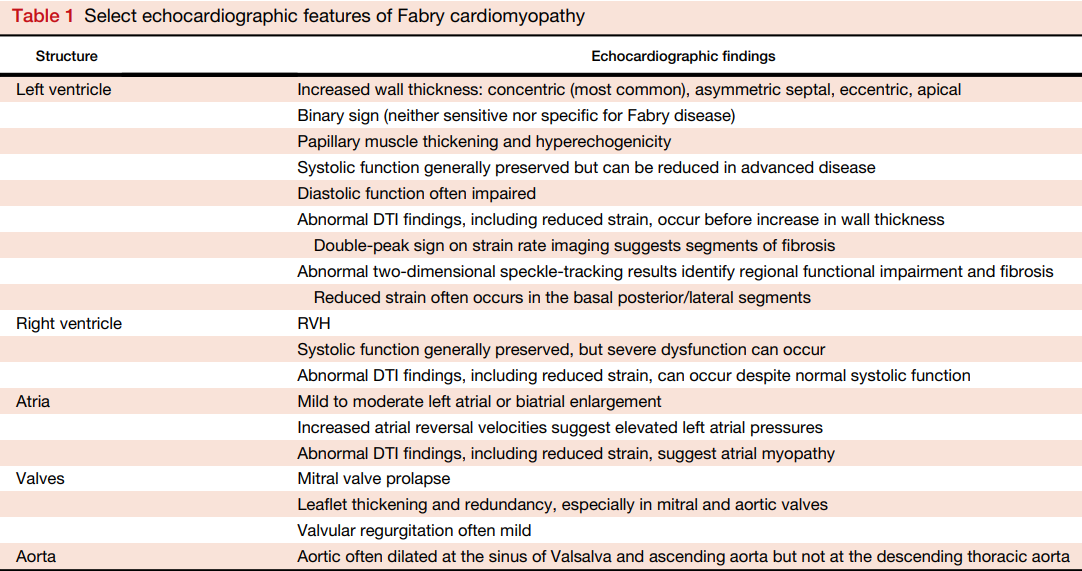
Features:
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731713001764?via%3Dihub
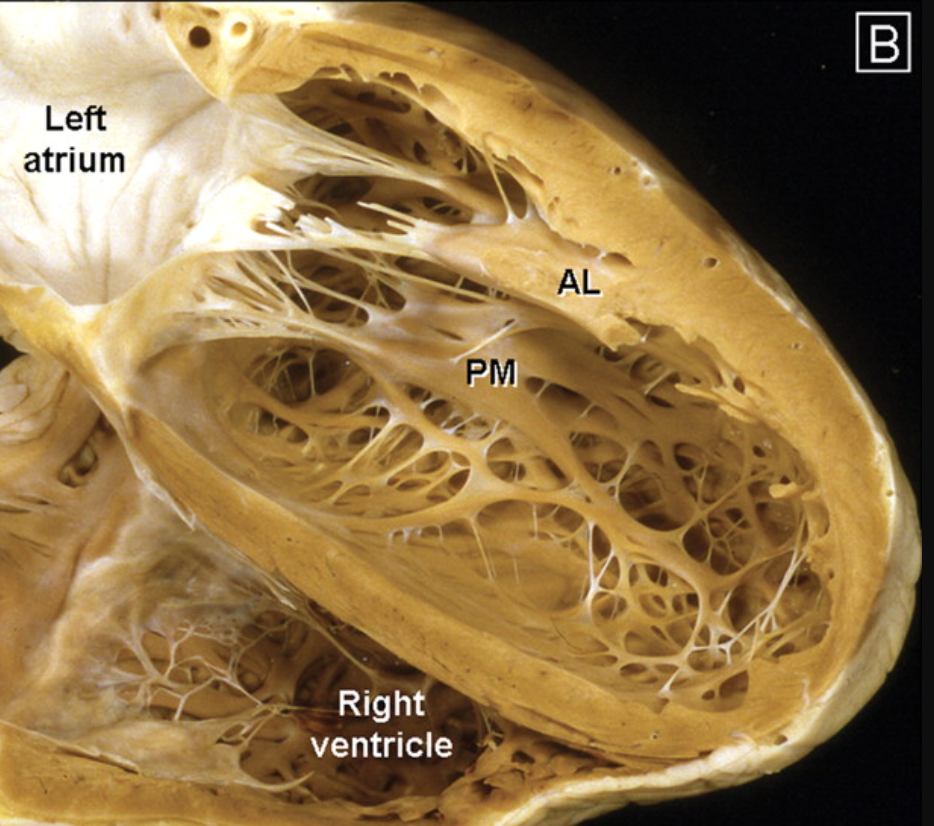
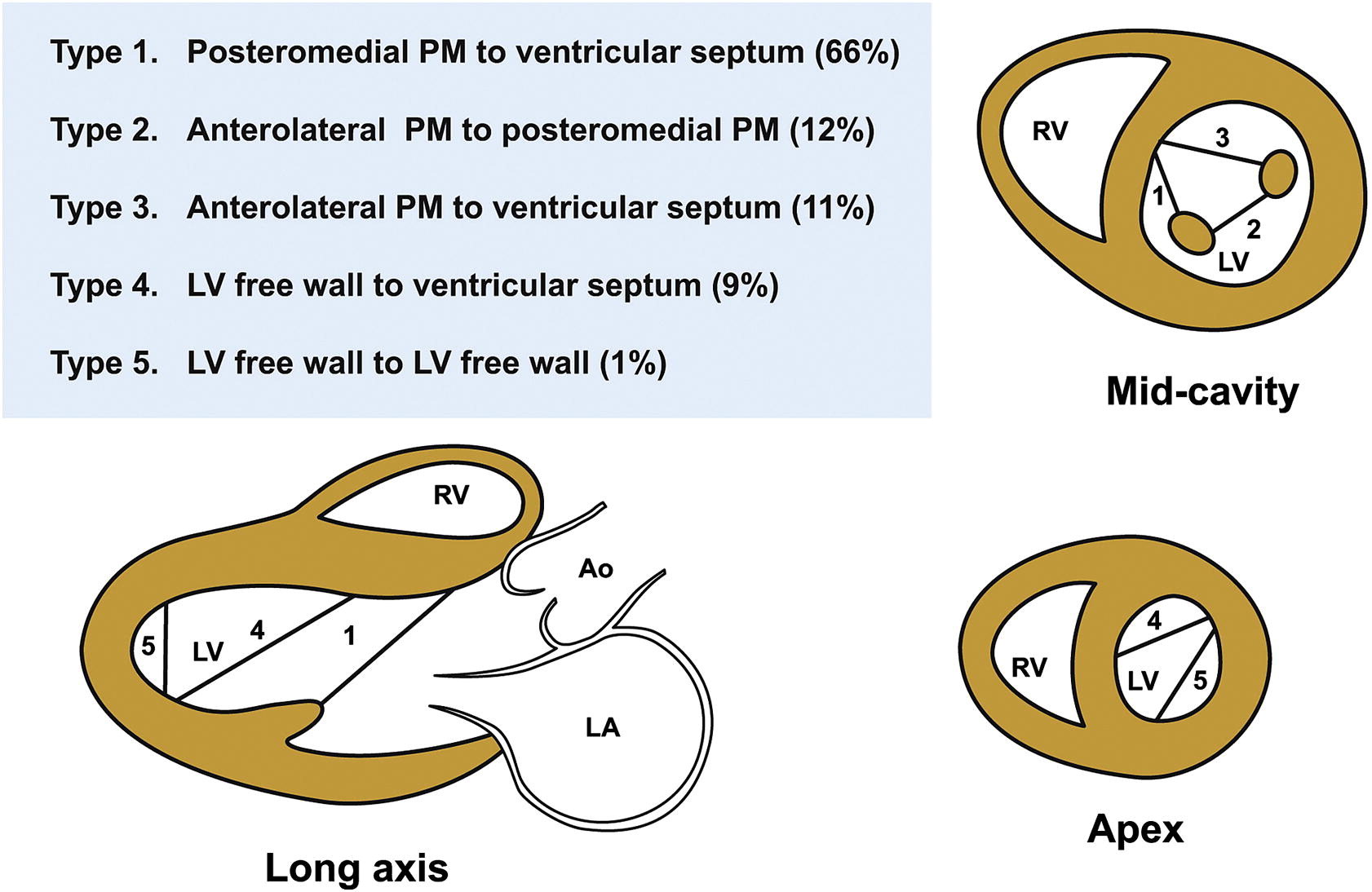
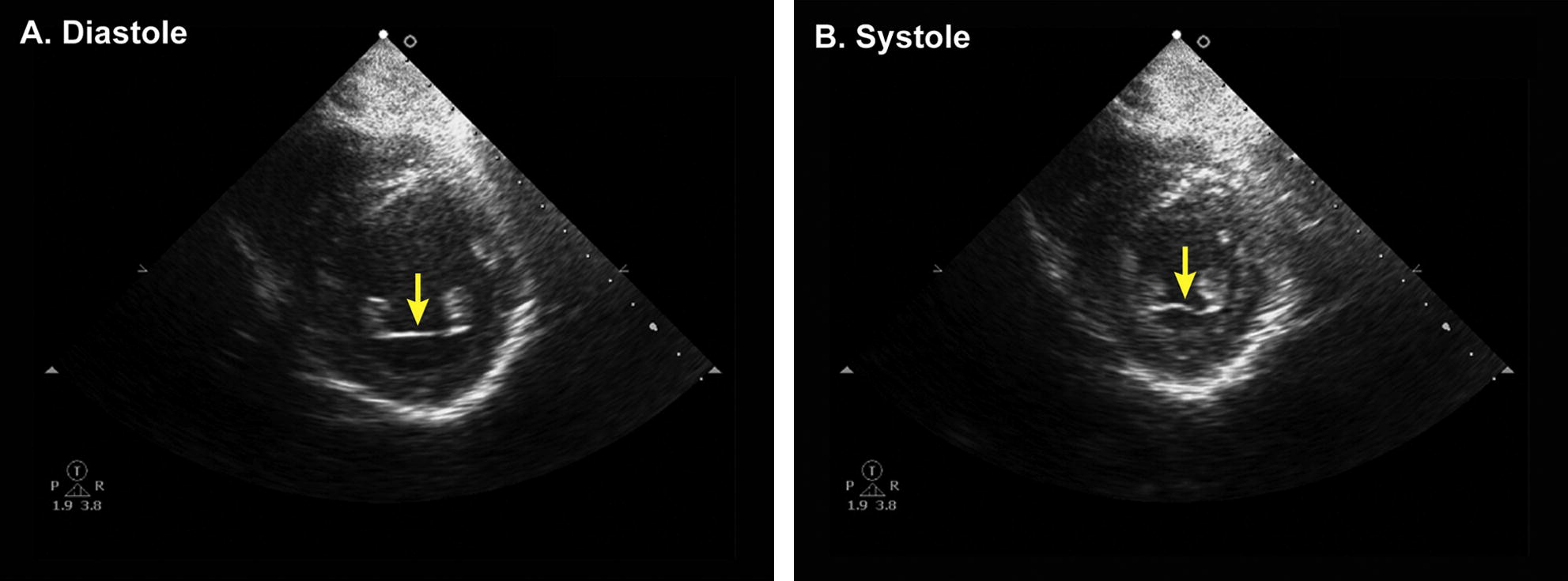
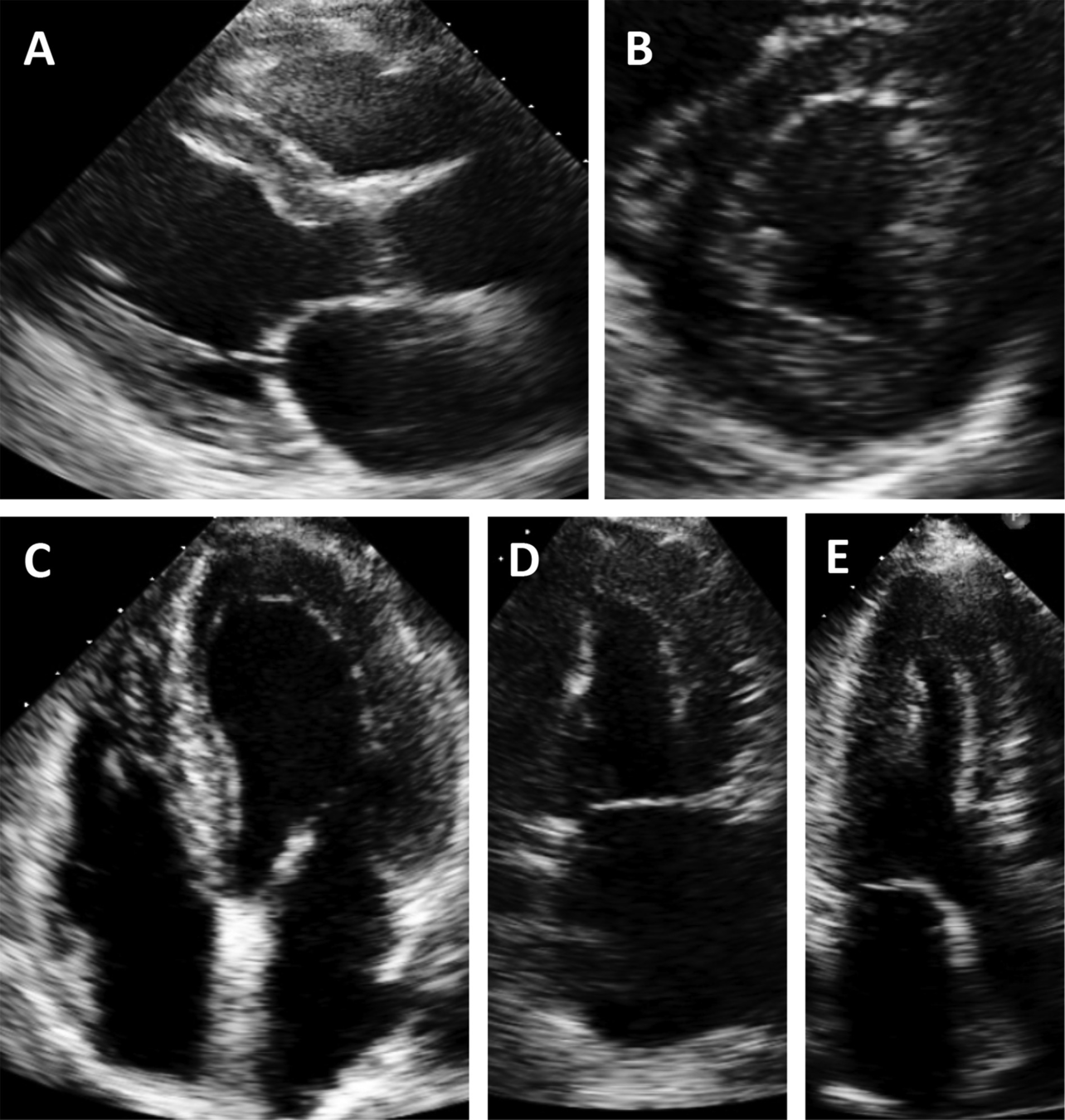
False Tendon
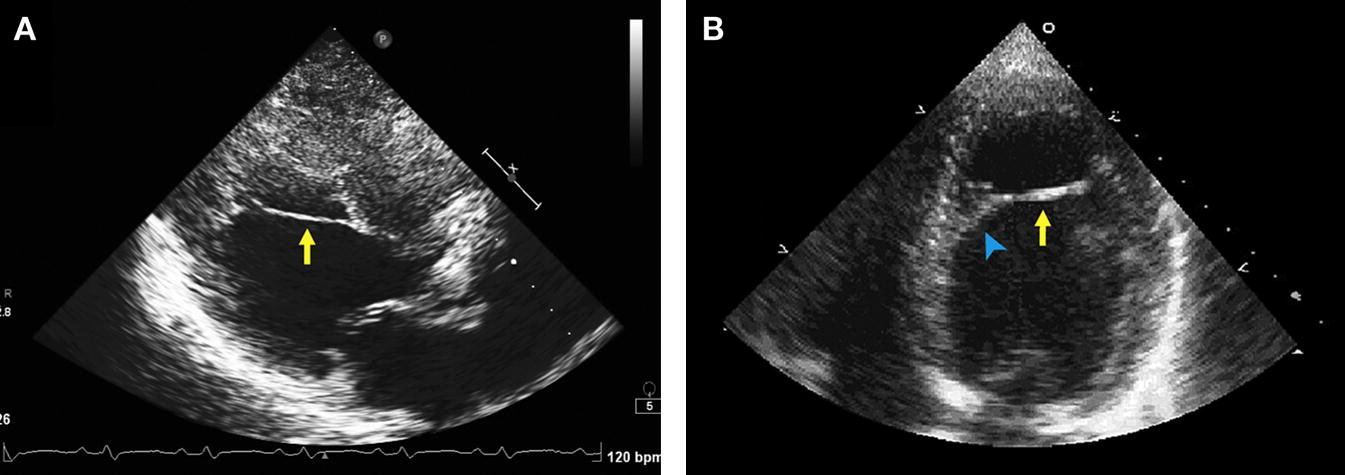
Muscular Band
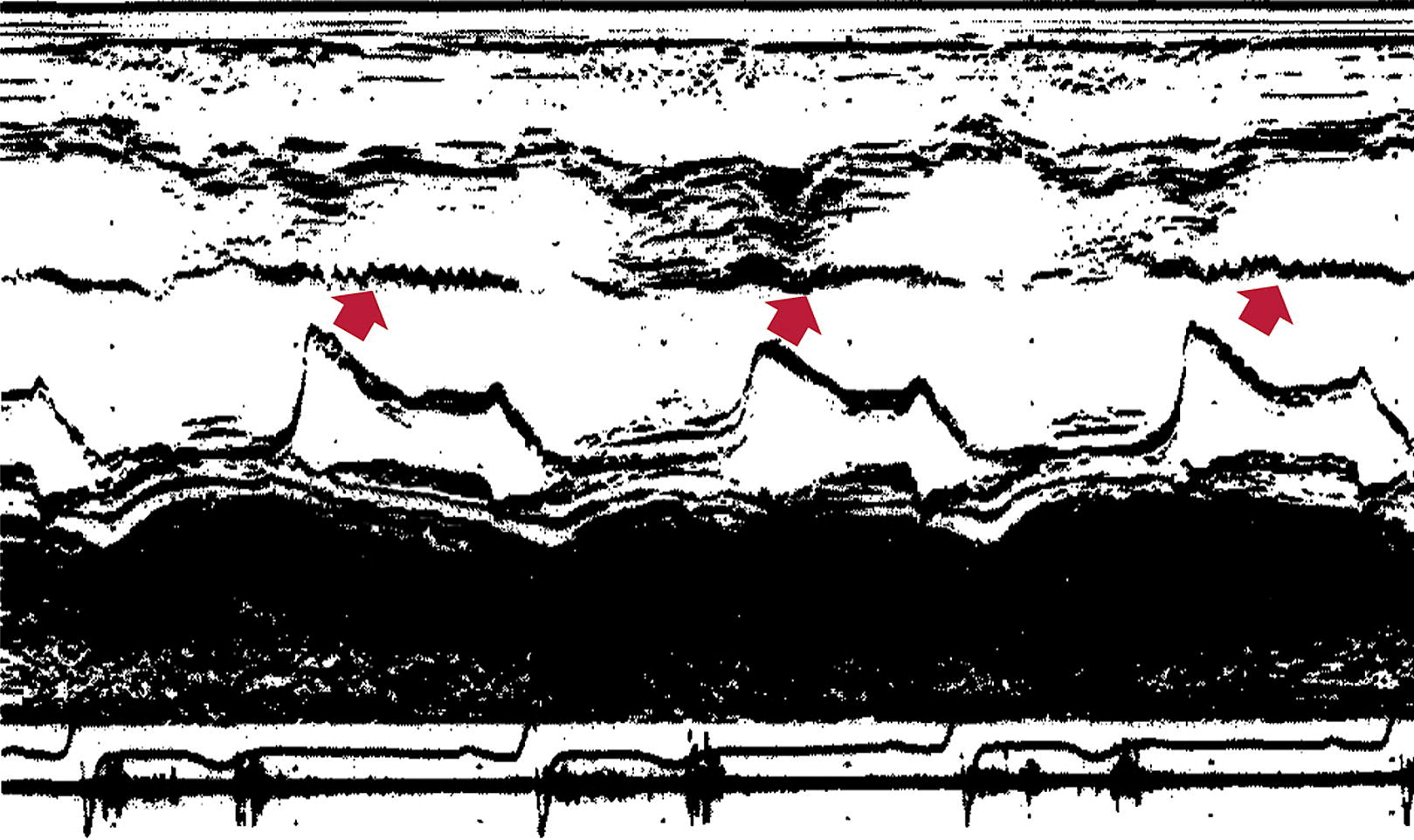
Papillary Muscle
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3816159/
https://www.sciencedirect.com/science/article/pii/S2468644120300931
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7520398/
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731720305940?via%3Dihub
Text
https://onlinelibrary.wiley.com/doi/epdf/10.1111/echo.14895
https://onlinelibrary-wiley-com.proxy1.lib.uwo.ca/doi/full/10.1111/echo.12900
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731718300415?via%3Dihub#bib20
https://www-sciencedirect-com.proxy1.lib.uwo.ca/science/article/pii/S0894731718300415?via%3Dihub#bib20
https://www-internationaljournalofcardiology-com.proxy1.lib.uwo.ca/article/S0167-5273(14)02384-5/fulltext
https://www-internationaljournalofcardiology-com.proxy1.lib.uwo.ca/article/S0167-5273(14)02384-5/fulltext
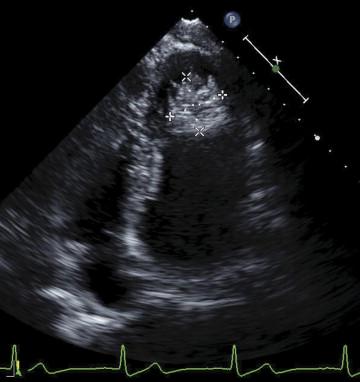
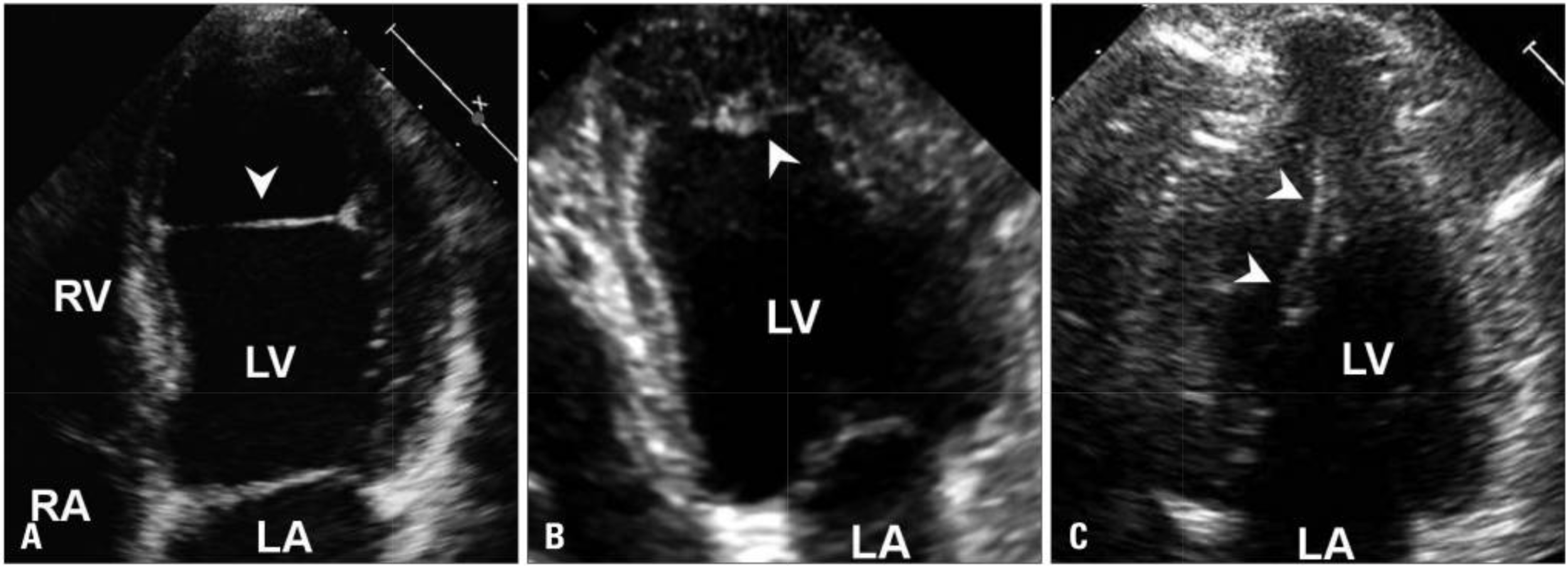
LV Thrombus post Anterior MI
By Atul Jaidka



