Donor-recipient compatibility in HSCT
(Hematopoietic stem cell transplantation)

Guillaume DELEVOYE
Lab Meeting 15/01/19
PharmD thesis project
PH CABRERA Quentin & PH MOARS Catherine
You are unique

Are human parts interchangeable ?
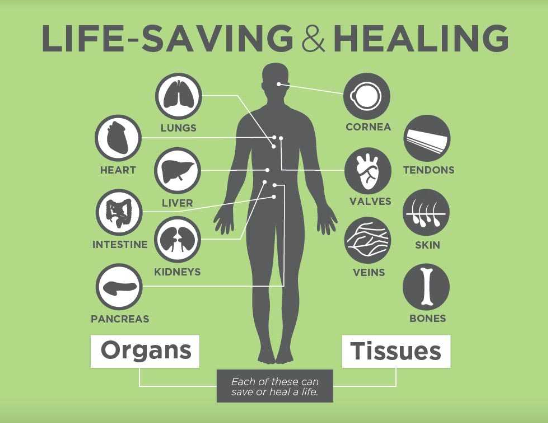
Blood 1667 | 1903
Lungs 1963
Liver 1963
Kidneys 1954
Heart 1967
Intestine 1988
Pancreas 1966
Cornea 1905
Tendons 1910
Valves 1960
Veins 1869
Skin 1869
Bone marrow 1956
>> Yes !...
This one is special
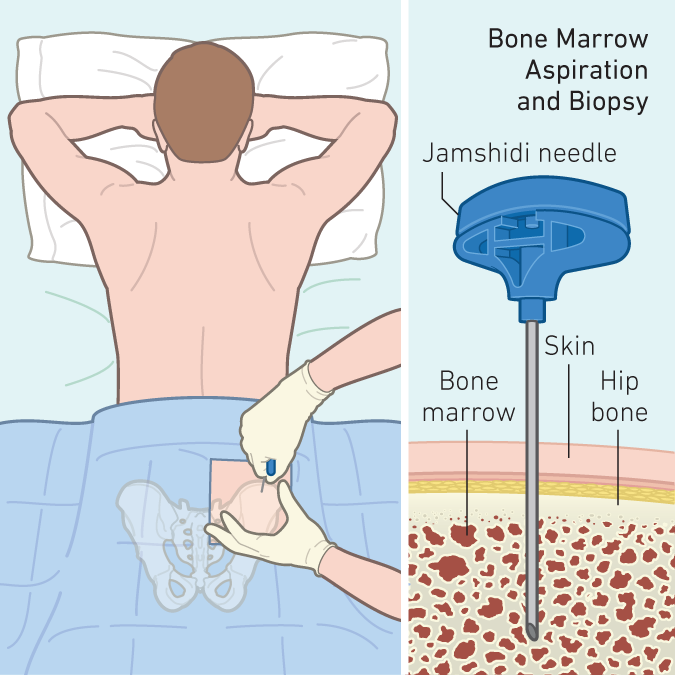
What are HSC in the bone marrow ?
(Hematopoietic Stem Cells)
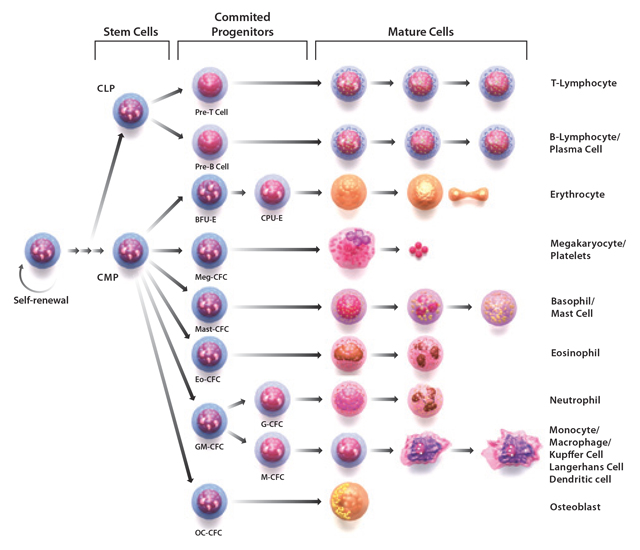
One cell rebuilds them all...
The whole immune system and all blood cells are built from HSC
When serious deregulation occurs
Death often follows
The immune system has almost no protection mechanism against itself: it's the last wall
HSCT
The main idea
1 ) Almost kill your patient by removing the immune system
2) Put back a new +/- similar immune system, hope it will work
3) Prey
While patient.is_alive or patient.is_sick:
The difference between HSCT and other transplantations
Every transplantation except HSCT
HSCT
Host Immune System (IS)
Attacks

Graft
Host' IS
Grafted IS
Host' organs
All weapons out
Immunosuppressant drugs
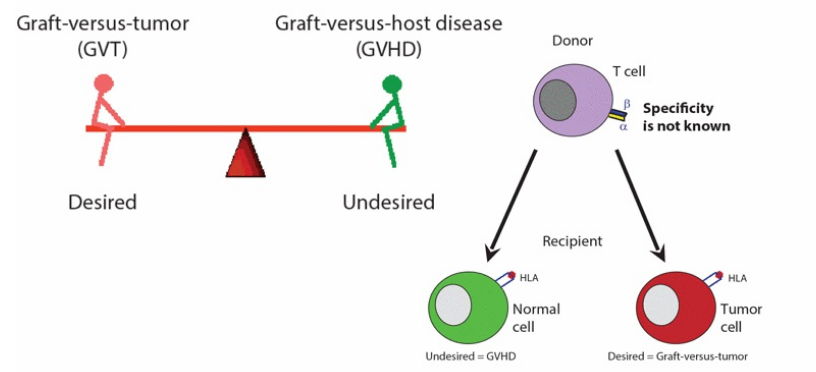
Tumorous behavior
GVT
GVHD
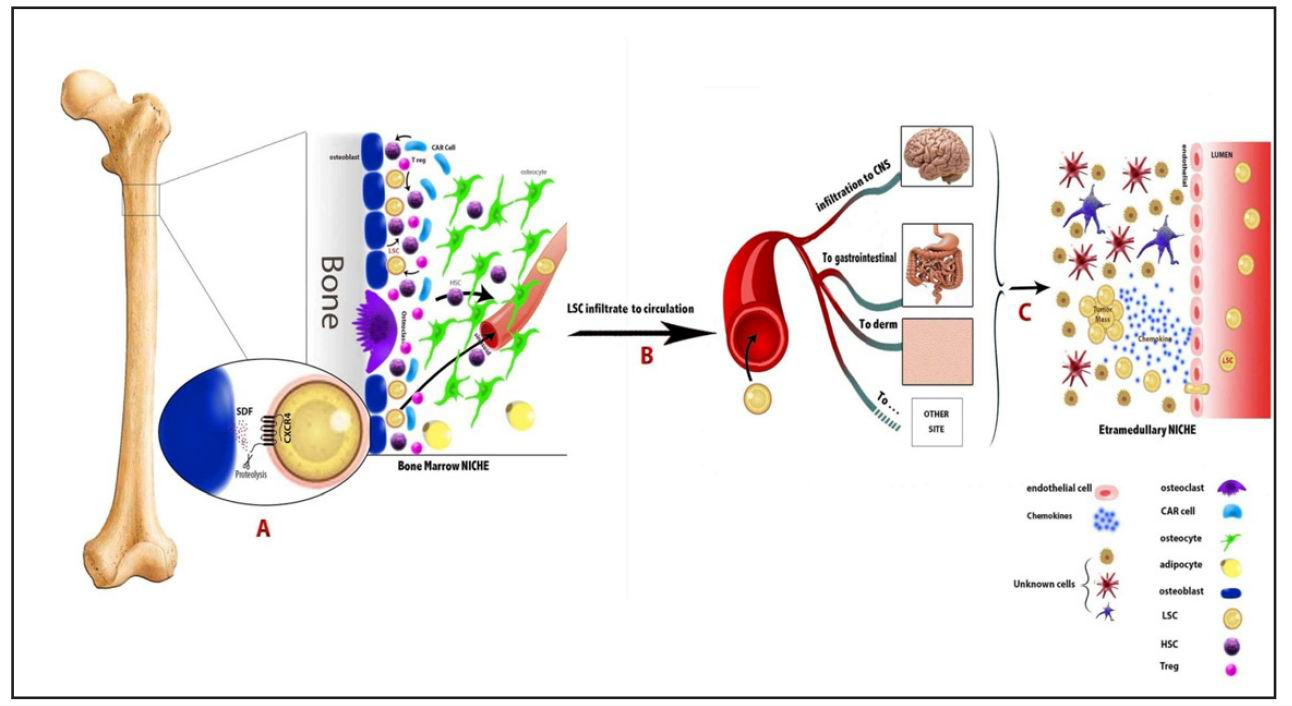
The whole process in one picture
Our project
We would like to build predictive models of compatibility for clinicians or researchers
And THIS is our PROJEEEEEEEEECT

DELEVOYE Guillaume
PH CABRERA Quentin & PH MOARS Catherine
What already exists
Relevant and numerous ML tools exist for almost all forms of grafts
Except in HSCT >> Too complex
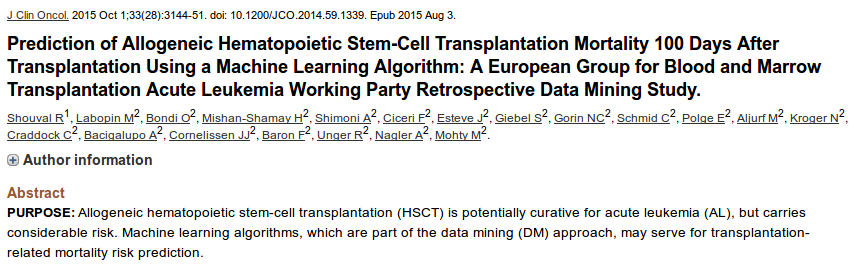
Just the 100 day overall mortality
Really a lot of censored data
Quick overview of what could be interesting to look at
Different outcomes for different indications
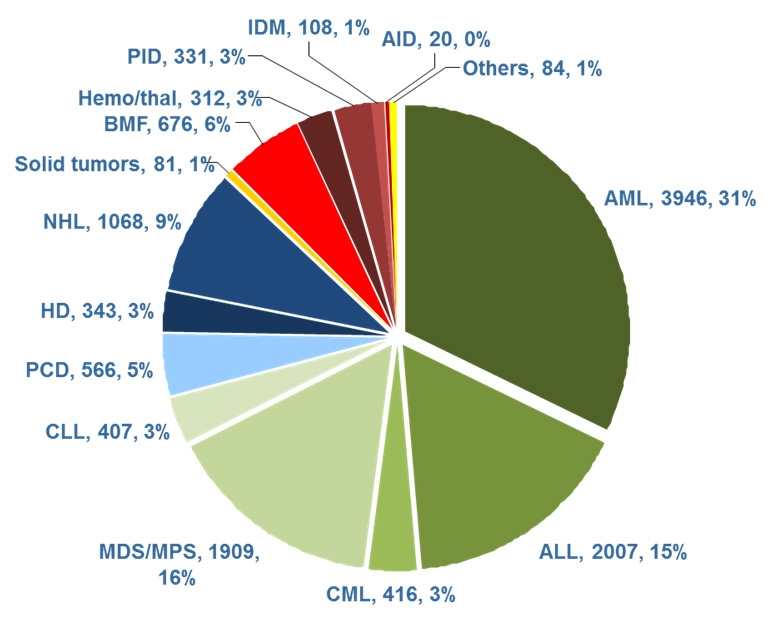
- GRFS 100
- Long terme relapse-free for tumoral pathologies
Quantify the impact of protocols
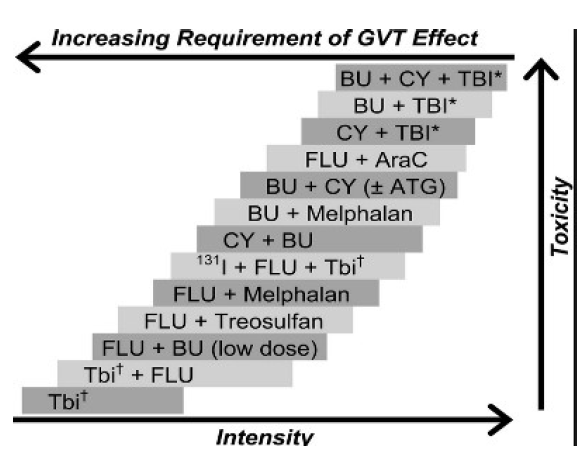
More than a hundreds of protocols:
- Total ablations
- Partial removals
- Sometimes patients already had 1 or 2 other transplants
Main idea:
It's barbarous
And it's a mess !!
Prediction of opportunistic infections
allo-HSCT requires to:
- Exterminate the previous immune system
- Use massive doses of immunosuppressants so that the graft doesn't attack the host
--> Patients are cured... And then often die from infections

Prediction of Graft versus host disease (GVHD)

Acute forms are lethal
... And chronic forms are also lethal
Dramatic incident
Really frequent
Prediction of Graft versus Tumor effect (GVTE)
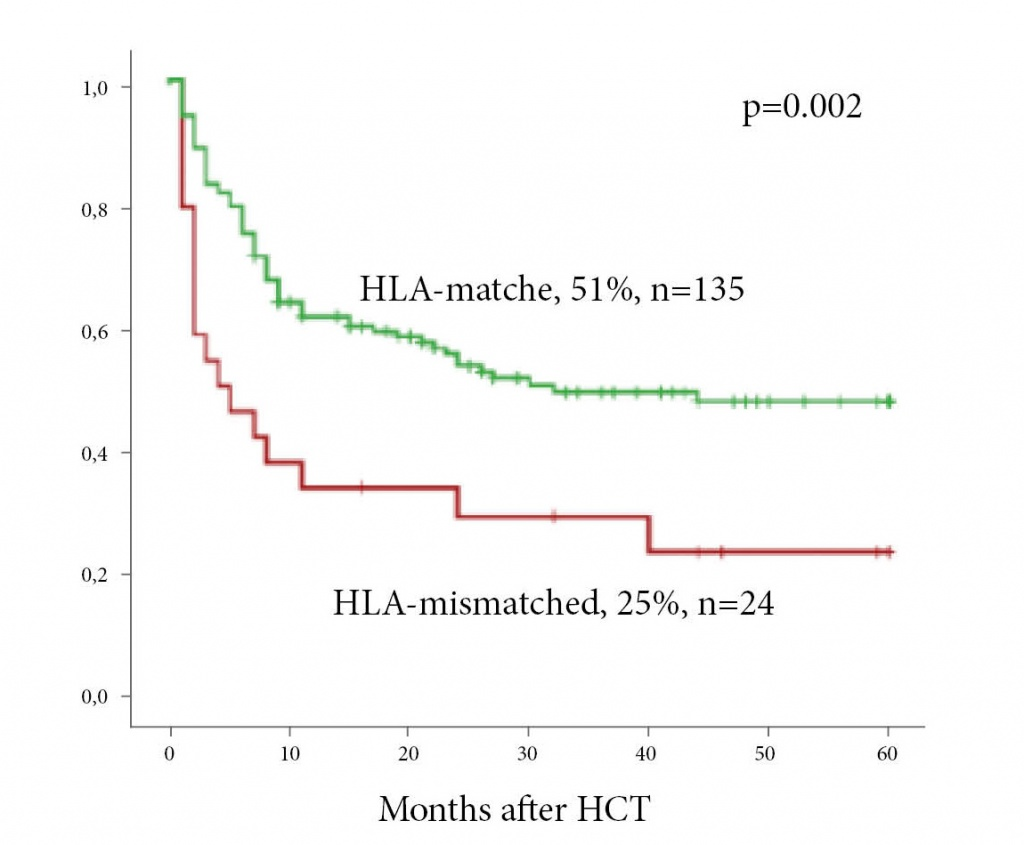
Allografts: HLA-system
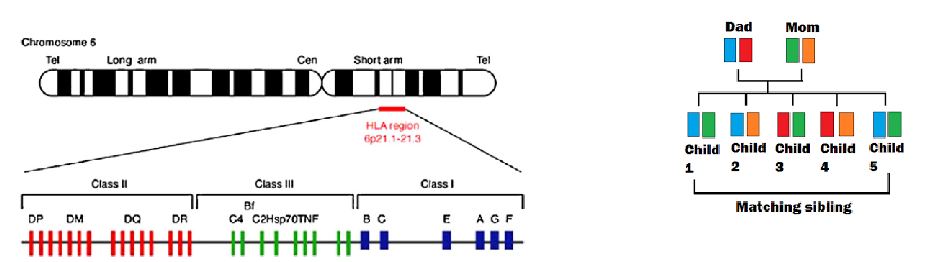
~25% of chances of full compatibility between siblings
- More possible combinations for a single human than there are humans beeins (~ 18 billions)
- Two people taken randomly = 1/10⁶ chances
- Strongly dependant of ethnies
- Strong biais in the databases
The main ideas
- Some 9/10 compatibility grafts show incredible results
- Some 10/10 compatibility grafts show poor results
We will be the first to ever work on HLA data
--> Determine if there are suboptimal and optimal HLA mismatches
The goal is to find good balances between:
- HLA Match VS Optimal mismatch
- GVHD vs GVT
- Immunosuppression VS infection risk
- Ablation VS Relapse risk
Oila oila
Thx :)
What makes you unique ?
Blood type
Genetic variants
DNA
Measurable attributes
Personal history
Personnality
Tastes
Health status
Almost everything is unique

Many unique things are still interchangeable

Autologous graft
With the patient's cells
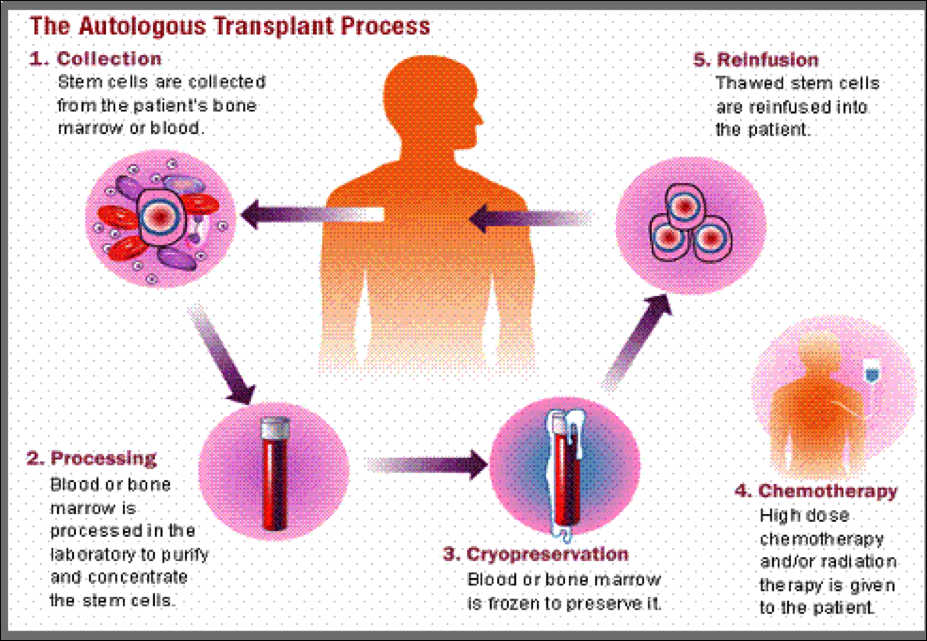
Even this simple case often fails
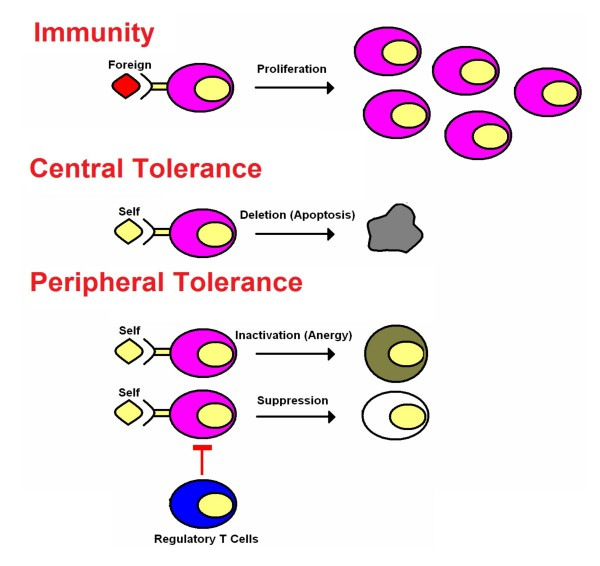
Immune system (IS)
- The immune tolerance is an ACTIVE phenomena
- Every cells shows "self-antigens" to proof it belongs to the self
Anything that cannot express those self-antigens shall be shot down
- Auto-reactive cells get destroyed during the "training" process
Auto-immunity and tolerance
PharmD Thesis
By biocompibens



