Targeting Beyond the Tumor: Radiation's Evolving Role in Oncogene-Driven Lung Cancer
Jonathan Sackett
Prompt for Consistent Citations:
Please provide a citation for the following article in a compact format suitable for slides. Use the following structure:
- Include the first author's last name and initials (omit additional authors for brevity).
- Write the full title of the article, capitalizing only the first word and proper nouns.
- Italicize the journal name using
<i>tags.- Add year, volume (and issue if applicable), and page range.
- Include a clickable DOI or URL using
<a>tags withtarget="_blank".- Wrap the entire citation in a
<div>withcitation footnoteclasses for styling.Example:
html
Copy code
<div class="citation footnote"> AuthorLastName Initial(s). Title of the article. <i>Journal Name</i> Year;Volume(Issue):Page Range. <a href="DOI or URL" target="_blank">DOI or URL</a> </div>Use this format to provide the citation.

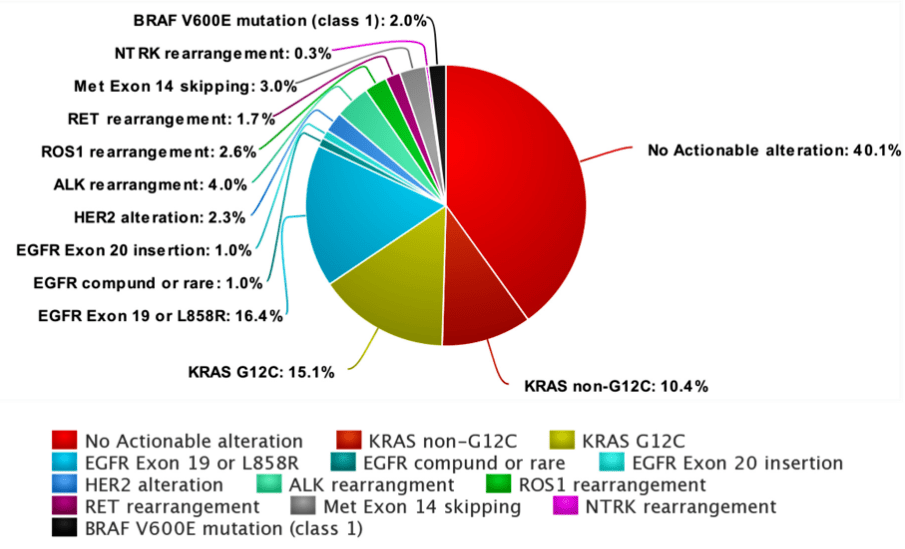
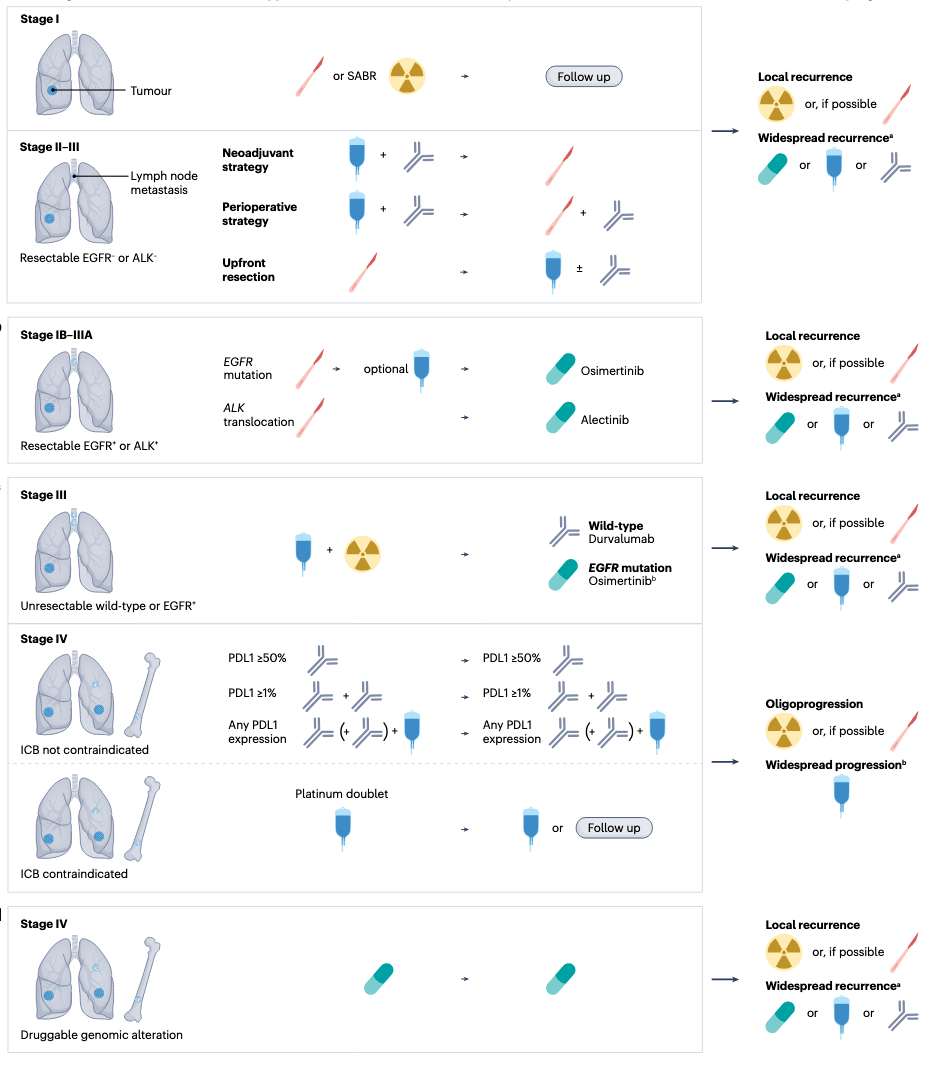
Hendriks LEL, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primers. 2024;10:71. https://doi.org/10.1038/s41572-024-00551-9
McMahon DJ. Is Immunotherapy Beneficial in Patients with Oncogene-Addicted Non-Small Cell Lung Cancers? A Narrative Review. Cancers 2024;16:527. https://doi.org/10.3390/cancers16030527
McMahon DJ. Is Immunotherapy Beneficial in Patients with Oncogene-Addicted Non-Small Cell Lung Cancers? A Narrative Review. Cancers 2024;16:527. https://doi.org/10.3390/cancers16030527
Evolution of Targeted Therapies in NSCLC
2003
Gefitinib
First EGFR TKI
2011
Crizotinib
First ALK/ROS1 TKI
2013
Erlotinib
EGFR TKI
Afatinib
EGFR TKI
2014
Alectinib
ALK TKI
Osimertinib
EGFR T790M
2017
Brigatinib
ALK TKI
Dabrafenib + Trametinib
BRAF V600E
2018
Dacomitinib
EGFR TKI
Lorlatinib
ALK TKI
Larotrectinib
NTRK fusion
2019
Entrectinib
ROS1/NTRK
2020
Pralsetinib
RET
Capmatinib
MET ex14
Selpercatinib
RET
2021
Sotorasib
First KRAS G12C
Mobocertinib
EGFR ex20
Amivantamab
EGFR ex20
Tepotinib
MET ex14
2022
Adagrasib
KRAS G12C
Friedlaender A. Oncogenic alterations in advanced NSCLC: a molecular super-highway. Biomarker Research 2024;12:24. https://doi.org/10.1186/s40364-024-00566-0



Hendriks LEL, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primers. 2024;10:71. https://doi.org/10.1038/s41572-024-00551-9
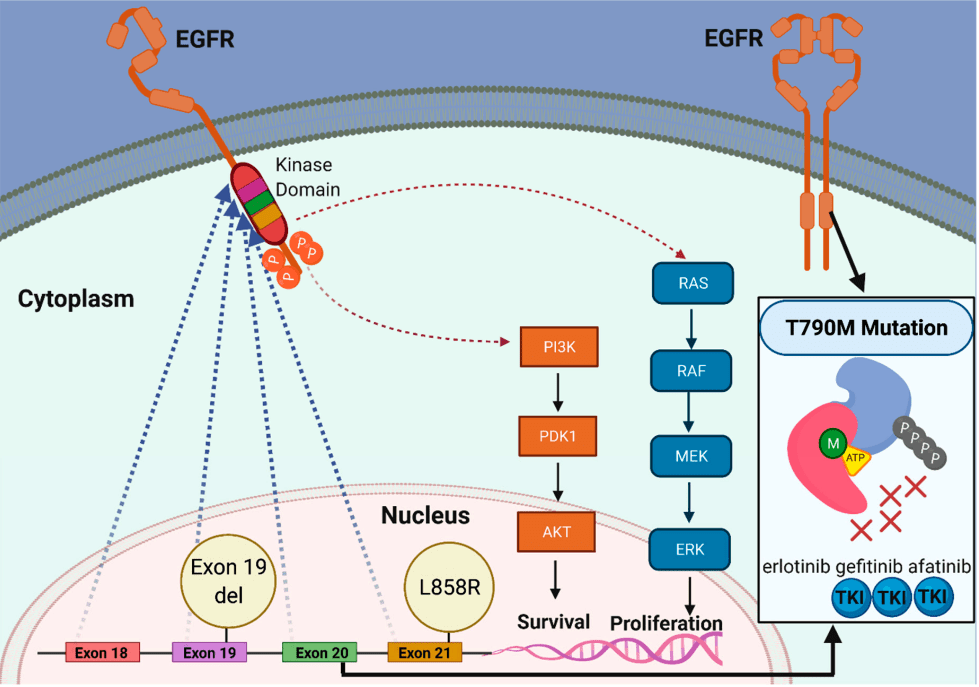
Meet the mutations
Exon 19 deletions, L858R mutations, and T790M
EGFR Mutations
Khaddour K. Targeting the Epidermal Growth Factor Receptor in EGFR-Mutated Lung Cancer: Current and Emerging Therapies. Cancers 2021;13(13):3164. https://doi.org/10.3390/cancers13133164
1st & 2nd Generations of EGFR TKIs
-
First-Generation
- Examples: Erlotinib, Gefitinib
- Mechanism: Reversible EGFR inhibitors
-
Key Points:
- Effective for activating mutations (e.g., exon 19, L858R)
- Limited against T790M mutation
- Poor CNS penetration
- Approval: Gefitinib (2003, IPASS), Erlotinib (2004, EURTAC)
-
Second-Generation
- Examples: Afatinib, Dacomitinib
- Mechanism: Irreversible EGFR/HER inhibitors
-
Key Points:
- Broader activity (e.g., G719X, S768I)
- Limited T790M activity
- Moderate CNS penetration
- Approval: Afatinib (2013, LUX-Lung 3/6), Dacomitinib (2018, ARCHER 1050)
Sources: IPASS, EURTAC, LUX-Lung 3/6, ARCHER 1050, FLAURA, AURA3 trials.
EURTAC
Erlotinib
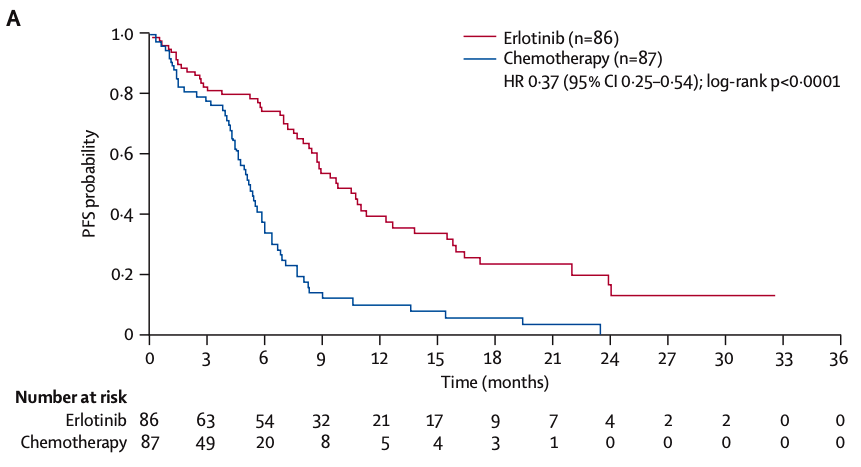
median PFS 9.7 mos vs 5.2 months
- Erlotinib: Continuous daily dosing (150 mg/day) until disease progression or intolerable toxicity.
- Chemotherapy: Four cycles of platinum-based chemotherapy unless progression or toxicity occurred earlier.
Rosell R. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive NSCLC (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol 2012;13(3):239-246. https://doi.org/10.1016/S1470-2045(11)70393-X
3rd Generations of EGFR TKIs
-
Third-Generation
- Examples: Osimertinib
- Mechanism: Irreversible, T790M-specific
-
Key Points:
- Effective for T790M and CNS metastases
- First-line for EGFR-mutated NSCLC
- Approval: Osimertinib (2017, FLAURA/AURA3)
-
Fourth-Generation
- Examples: BLU-945, Lazertinib
Sources: IPASS, EURTAC, LUX-Lung 3/6, ARCHER 1050, FLAURA, AURA3 trials.
FLAURA trial
Osimertinib
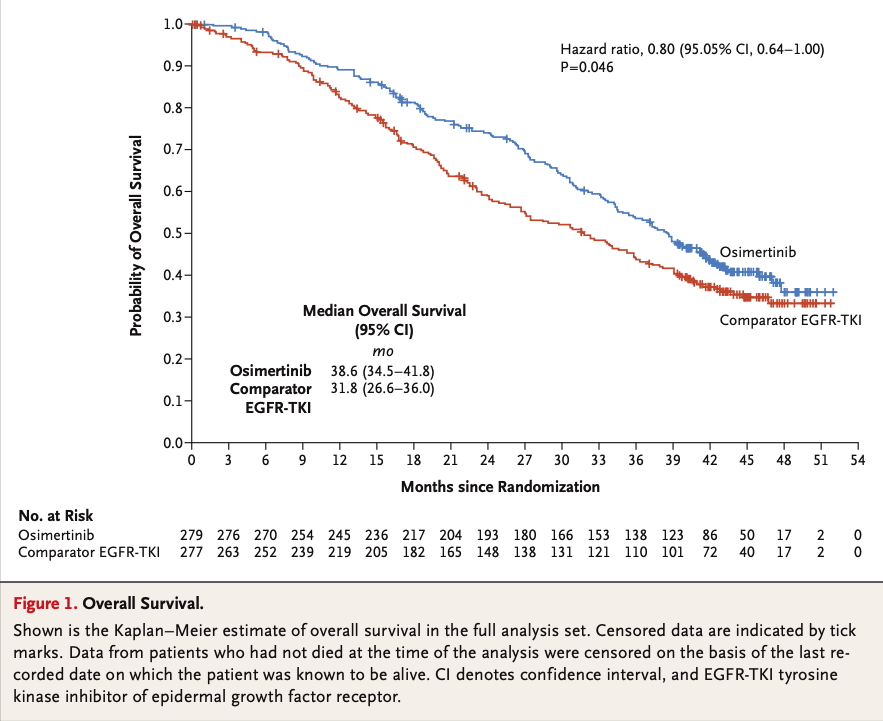
Ramalingam SS. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N Engl J Med 2020;382:41-50. https://doi.org/10.1056/NEJMoa1913662
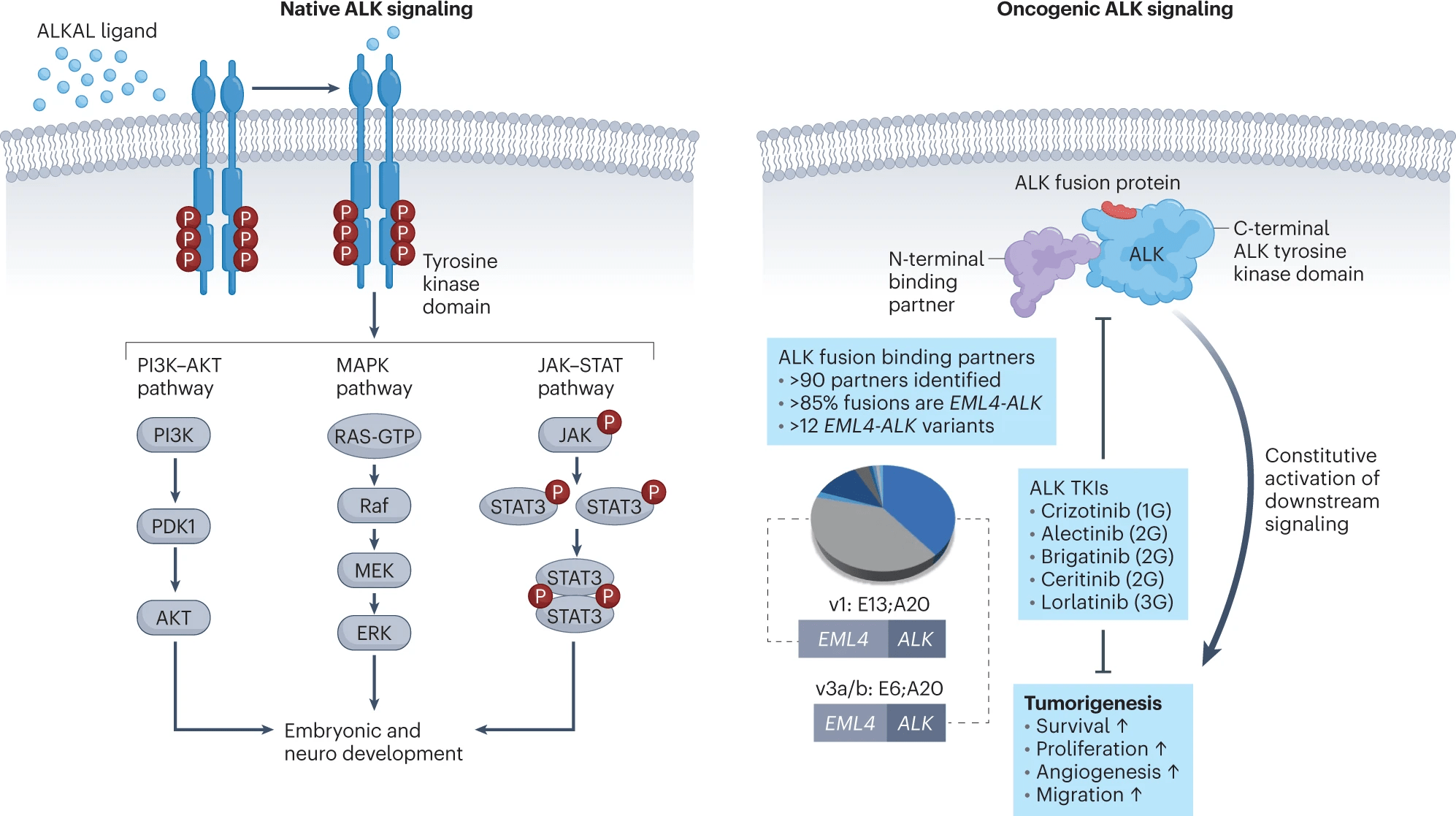
Schneider JL. ALK-positive lung cancer: a moving target. Nat Cancer 2023;4:330-343. https://doi.org/10.1038/s43018-023-00515-0
First-Generation ALK Inhibitors
- Example: Crizotinib
- Mechanism: Inhibits ALK, ROS1, and MET.
-
Key Points:
- Effective against ALK rearrangements (e.g., EML4-ALK).
- CNS Penetration: Limited, leading to high rates of CNS progression (PROFILE 1014 trial).
- Radiation Sensitivity: Enhances radiosensitivity by suppressing DNA damage repair mechanisms.
- Resistance: Mutations like L1196M limit long-term efficacy.
- Approval: 2011 (PROFILE trials).
Sources: PROFILE, ASCEND, ALEX, ALTA, and CROWN trials.
Second-Generation ALK Inhibitors
- Examples: Ceritinib, Alectinib, Brigatinib
- Mechanism: Overcomes crizotinib resistance and achieves superior CNS penetration.
-
Key Points:
- Effective against ALK resistance mutations (e.g., L1196M, G1269A).
- CNS Penetration: Significant improvements over crizotinib. Alectinib and Brigatinib achieve prolonged CNS control (ALEX and ALTA trials).
-
Approval:
- Ceritinib: 2014 (ASCEND trials).
- Alectinib: 2015 (ALEX trial).
- Brigatinib: 2017 (ALTA trial).
Sources: PROFILE, ASCEND, ALEX, ALTA, and CROWN trials.
Third-Generation ALK Inhibitors
- Example: Lorlatinib
- Mechanism: Targets ALK resistance mutations (e.g., G1202R) and CNS metastases.
-
Key Points:
- CNS Penetration: High blood-brain barrier permeability; intracranial response rate of ~82% (CROWN trial).
-
Radiation Considerations:
- Often delays need for SRS or WBRT.
- Recommended after failure of second-generation inhibitors.
- Approval: 2018 (CROWN trial).
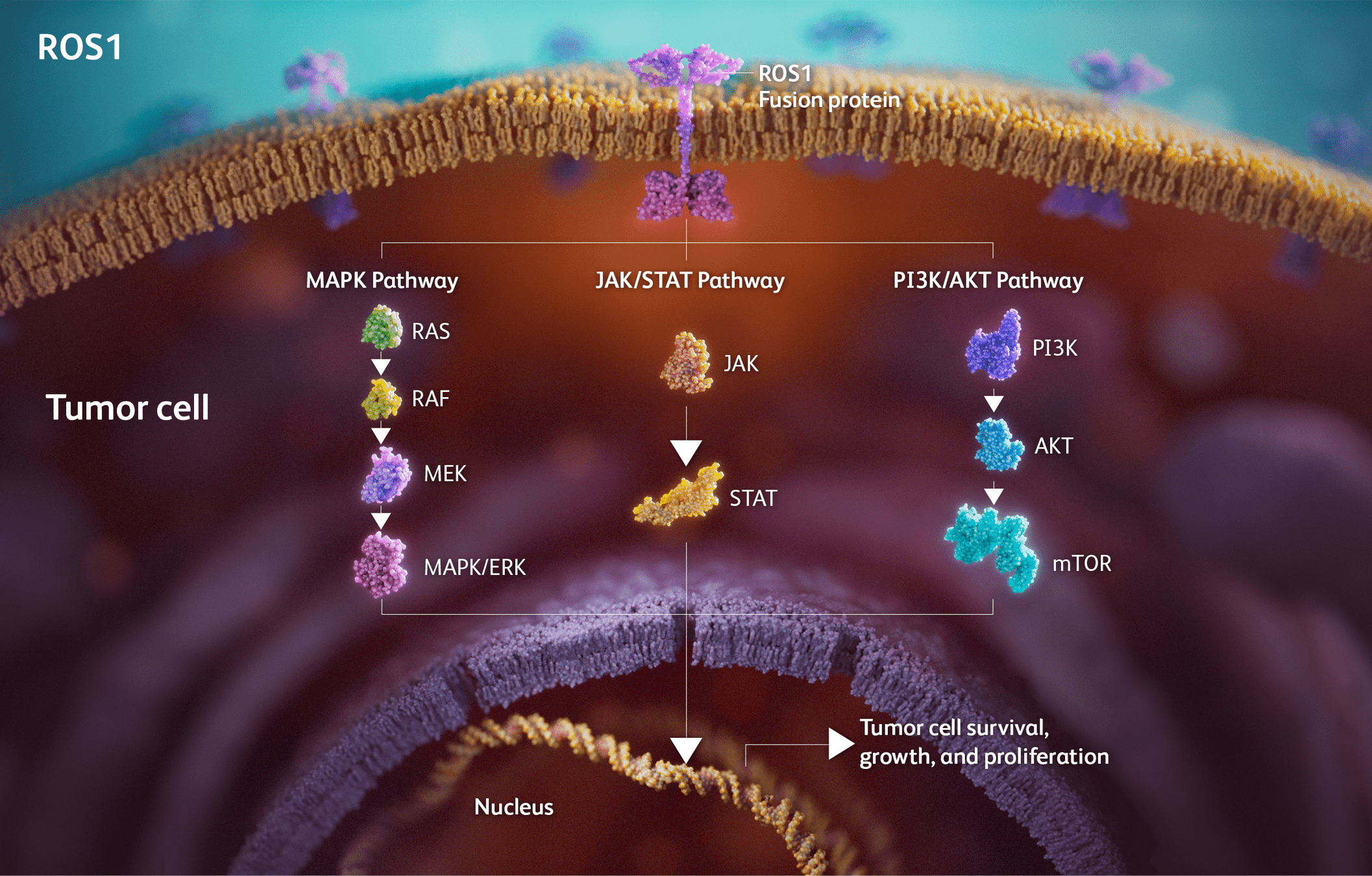
Drugs Targeting ROS1
- Examples: Crizotinib, Entrectinib, Lorlatinib, Repotrectinib.
- Mechanism: Inhibit ROS1 fusion-driven signaling to block tumor growth and progression.
-
Key Points:
- Crizotinib: First ROS1 inhibitor approved; limited CNS activity.
- Entrectinib: Significant CNS penetration, durable intracranial responses (STARTRK trials).
- Lorlatinib: Effective against crizotinib-resistant ROS1 mutations.
- Repotrectinib: Promising in both ROS1 TKI-naïve and pretreated patients (TRIDENT-1 trial).
-
Approval:
- Crizotinib: 2016 (PROFILE trials).
- Entrectinib: 2019 (STARTRK trials).
Sources: PROFILE, STARTRK, and TRIDENT-1 trials.
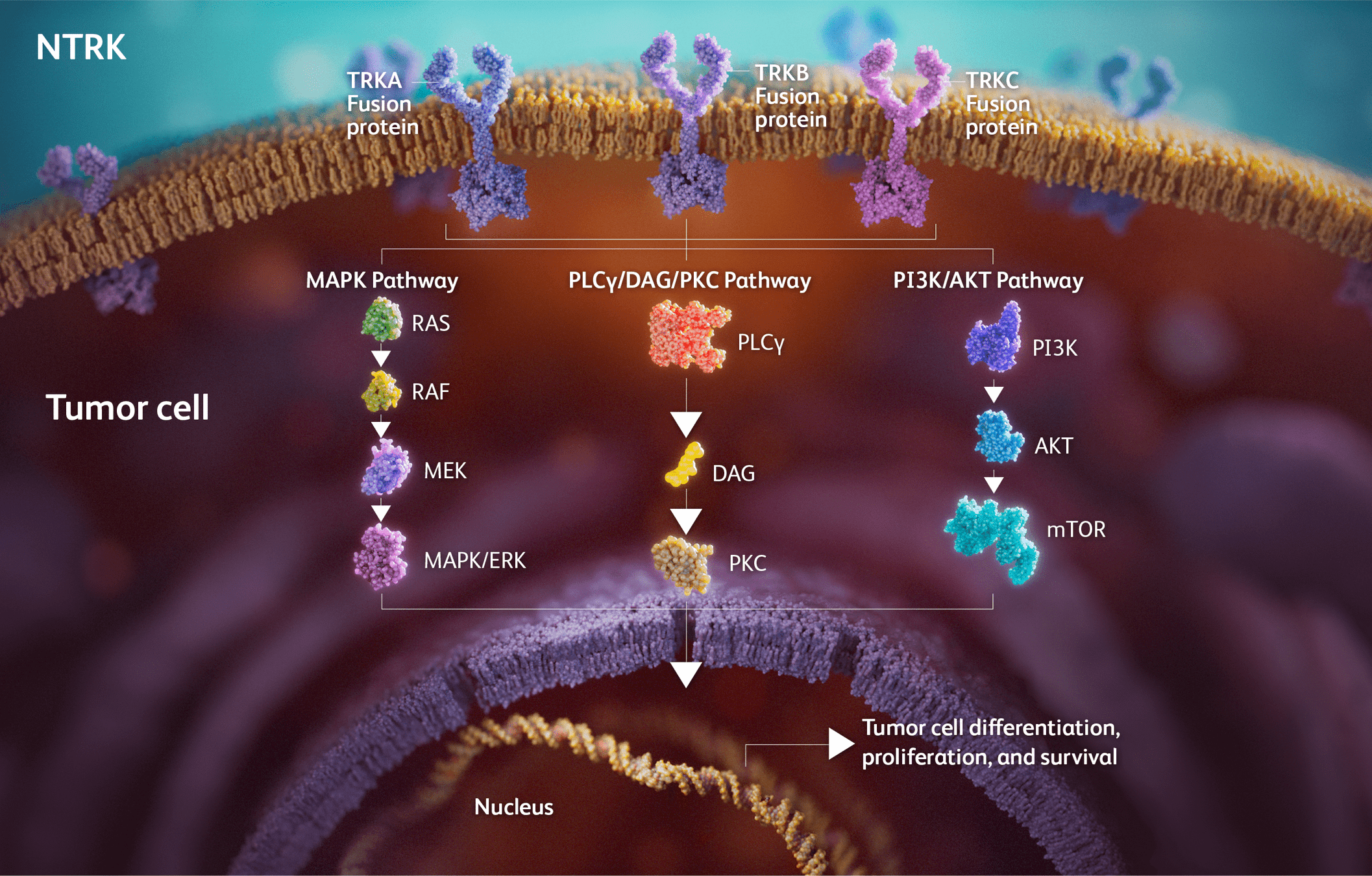
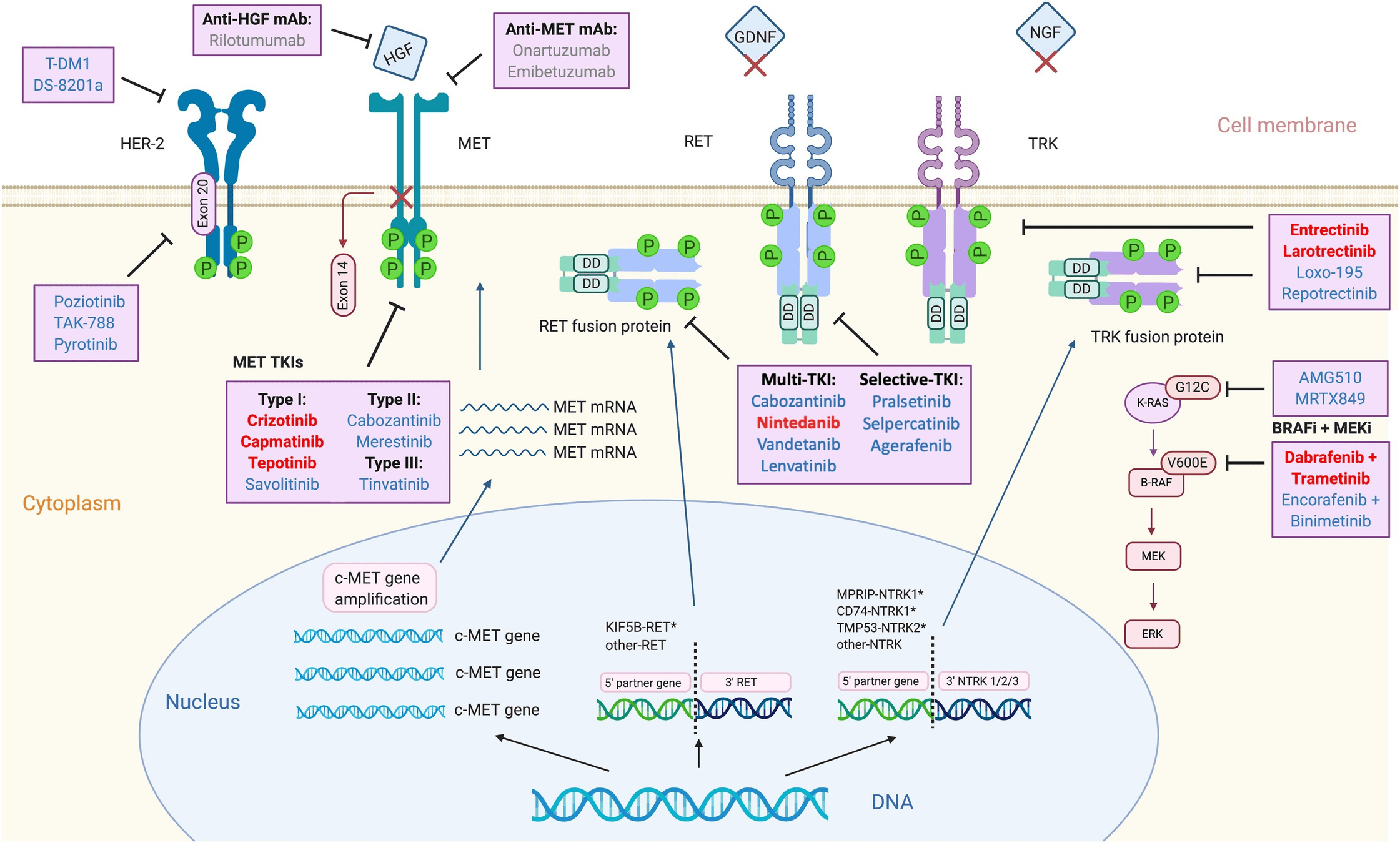
Drugs Targeting NTRK
- Examples: Larotrectinib, Entrectinib.
- Mechanism: Inhibit TRK fusions (NTRK1/2/3) to block tumor growth.
-
Key Points:
- Larotrectinib: High ORR (~75%) across multiple tumor types (NAVIGATE trial).
- Entrectinib: Durable responses in CNS-positive disease (STARTRK trials).
- Resistance: Secondary mutations (e.g., solvent front mutations) drive resistance to first-line TRK inhibitors.
-
Approval:
- Larotrectinib: 2018 (NAVIGATE, SCOUT trials).
- Entrectinib: 2019 (STARTRK trials).
Sources: NAVIGATE, SCOUT, and STARTRK trials.
STARTRK Trials: Design and Patient Population
Study Overview:
- Combined analysis of three trials:
- STARTRK-1 and ALKA-372-001: Phase I trials.
- STARTRK-2: Phase II global basket trial.
- Target Population: Adults with ROS1 fusion-positive, locally advanced or metastatic NSCLC.
Inclusion Criteria:
- ROS1 fusion–positive NSCLC (confirmed by NGS or local testing).
- Measurable disease (RECIST v1.1).
- ECOG performance status 0–2.
- Asymptomatic or pretreated CNS metastases allowed.
Exclusion Criteria:
- Extracranial progression after prior ROS1 TKI (except CNS-only progression).
- Significant comorbidities or unresolved toxicities.
Drilon A, et al. Long-term efficacy and safety of entrectinib in ROS1 fusion–positive NSCLC. JTO Clin Res Rep, 2022. https://doi.org/10.1016/j.jtocrr.2022.100332
STARTRK Trials: Methods
- Intervention: Oral entrectinib 600 mg/day until progression, unacceptable toxicity, or withdrawal.
-
Endpoints:
- Primary: Objective response rate (ORR) and duration of response (DoR) (assessed by blinded independent central review [BICR]).
- Secondary: Progression-free survival (PFS), overall survival (OS), and intracranial efficacy.
- Assessments: Imaging every 8 weeks and CNS-specific scans for patients with baseline CNS metastases.
- Safety Monitoring: Adverse events assessed per CTCAE v4.03.
Drilon A, et al. Long-term efficacy and safety of entrectinib in ROS1 fusion–positive NSCLC. JTO Clin Res Rep, 2022. https://doi.org/10.1016/j.jtocrr.2022.100332
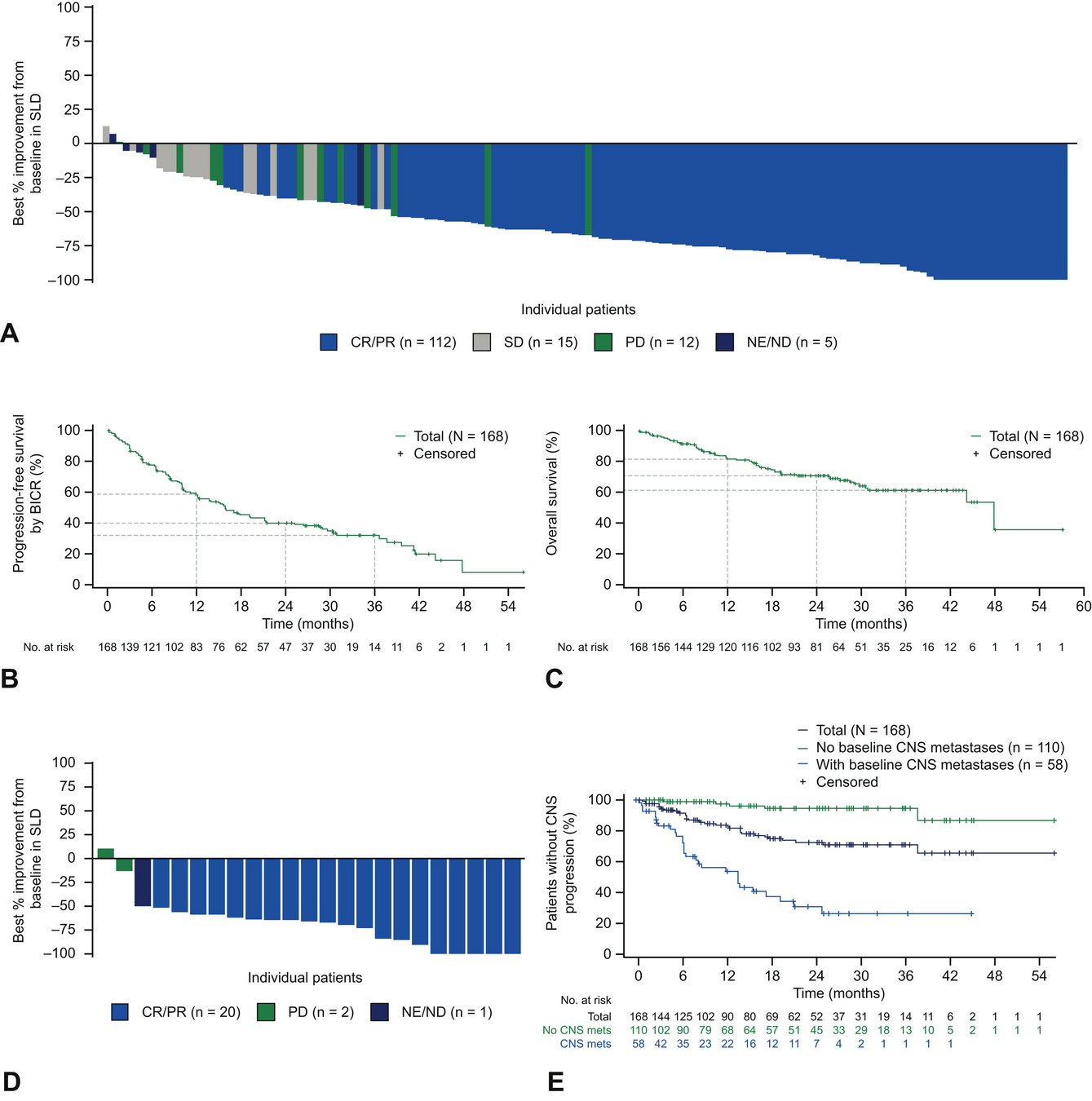
STARTRK Trials: Key Results
-
Overall Population (ROS1 TKI–Naïve):
- ORR: 68% (95% CI: 60.2–74.8).
- Median DoR: 20.5 months.
- Median PFS: 15.7 months; median OS: 47.8 months.
-
Patients with Baseline CNS Metastases:
- Intracranial ORR: 80% (95% CI: 59.3–93.2).
- Median intracranial DoR: 12.9 months.
- Median intracranial PFS: 8.8 months.
-
Post-Crizotinib Cohort:
- ORR: 11%; Median PFS: 4.7 months.
Drilon A, et al. Long-term efficacy and safety of entrectinib in ROS1 fusion–positive NSCLC. JTO Clin Res Rep, 2022. https://doi.org/10.1016/j.jtocrr.2022.100332
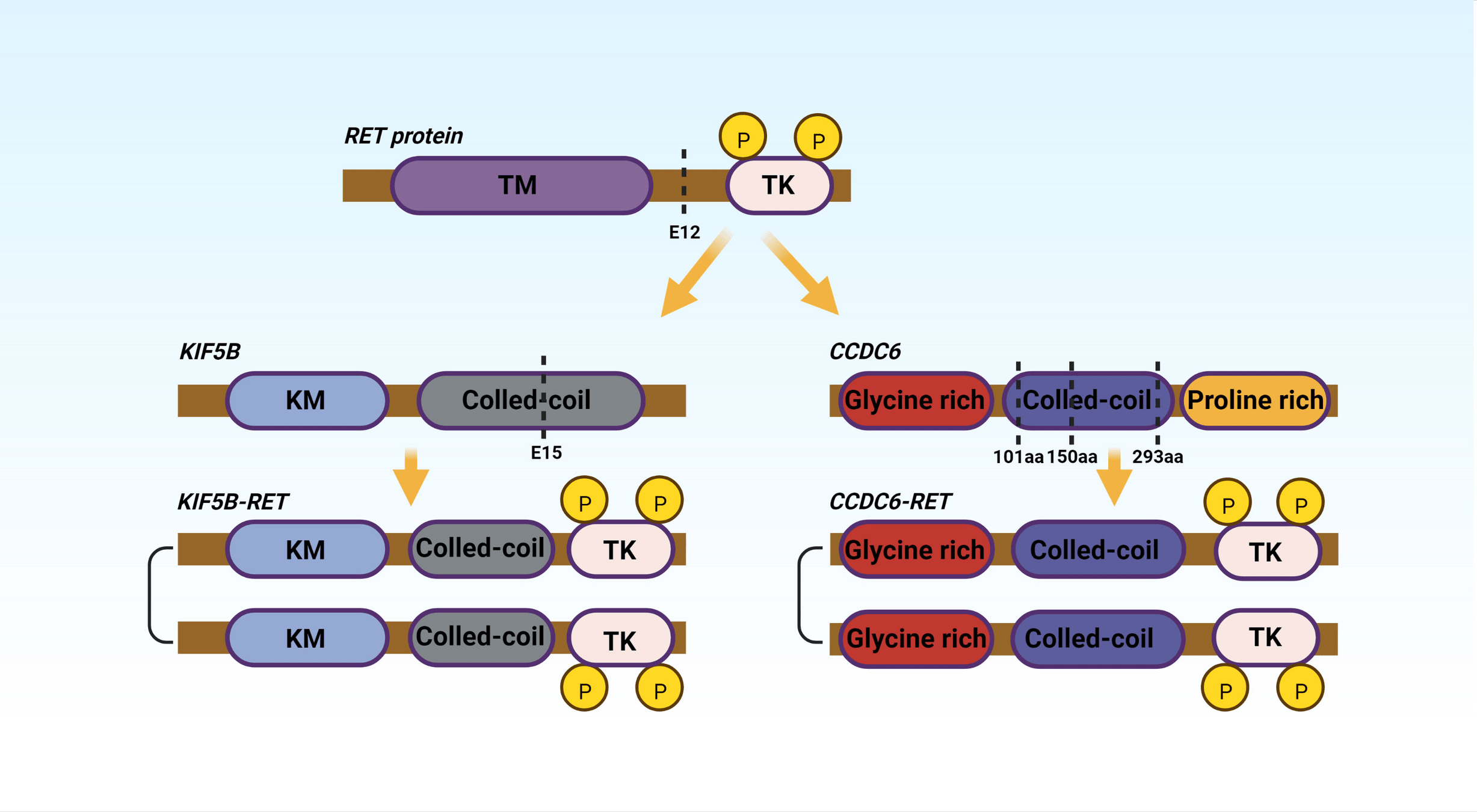
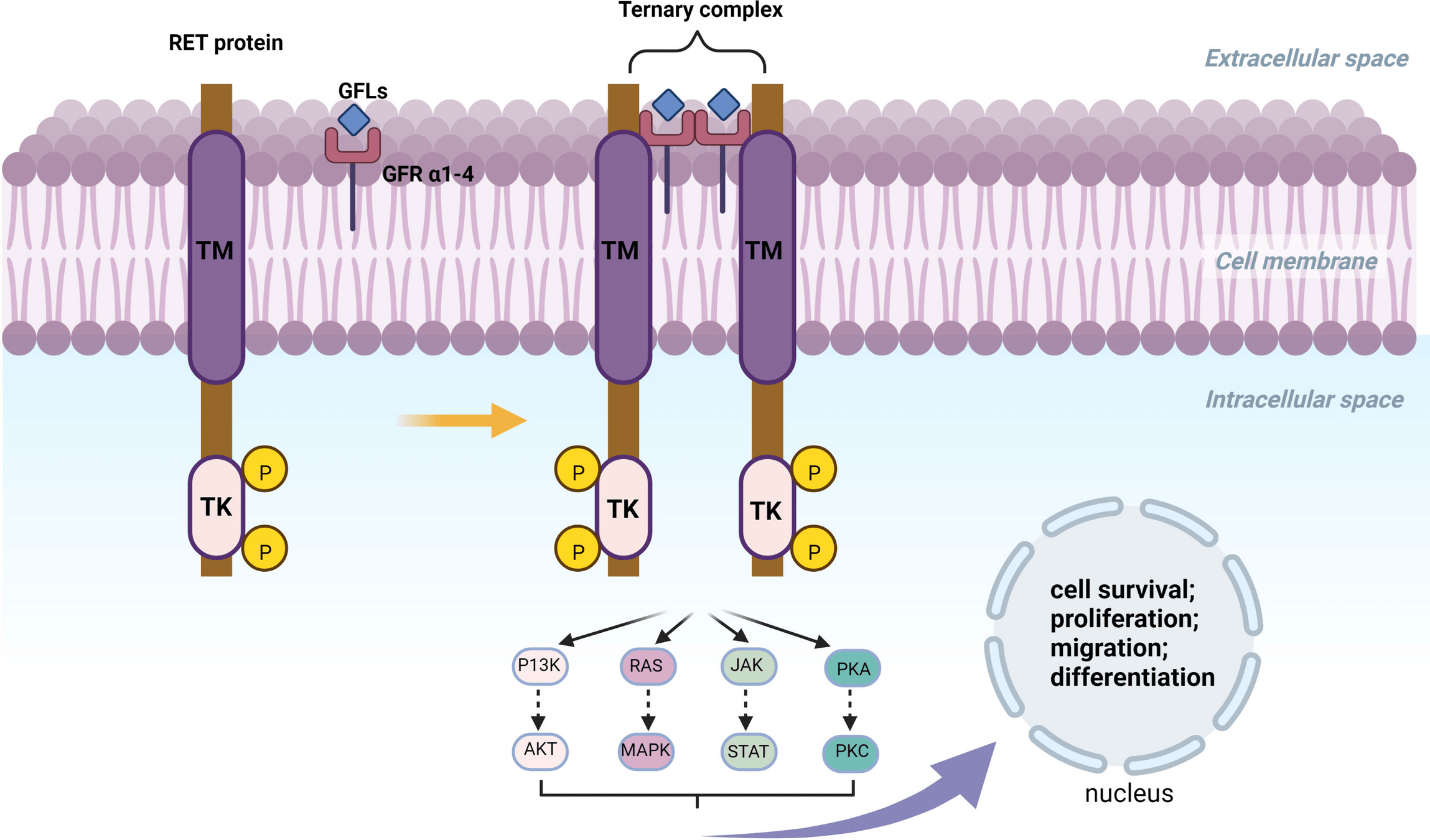
Drugs Targeting RET Fusions
- Examples: Selpercatinib, Pralsetinib.
- Mechanism: Inhibit RET fusion-driven signaling to block tumor growth and progression.
-
Key Points:
- Selpercatinib: High ORR (~85%) with durable responses (LIBRETTO trials).
- Pralsetinib: Efficacious in both RET fusion-positive NSCLC and thyroid cancers (ARROW trial).
- Well-tolerated with manageable toxicities (e.g., hypertension).
-
Approval:
- Selpercatinib: 2020 (LIBRETTO trials).
- Pralsetinib: 2020 (ARROW trial).
Sources: LIBRETTO and ARROW trials.
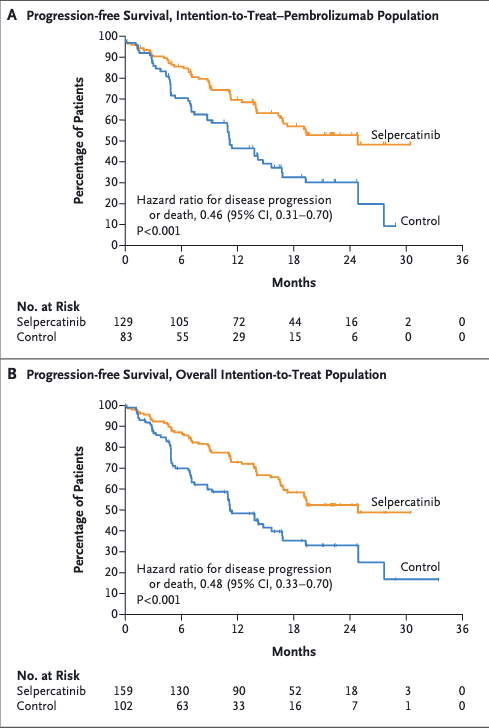
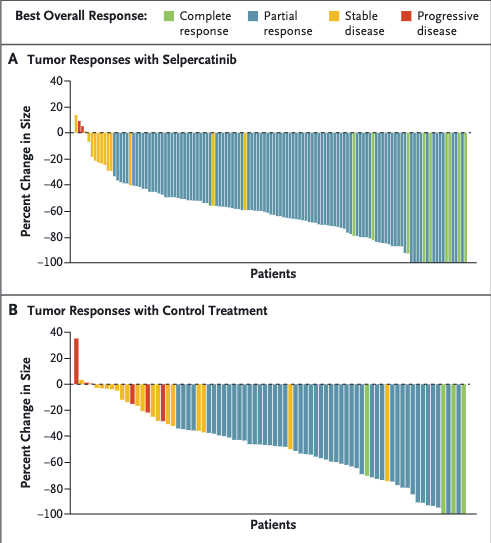
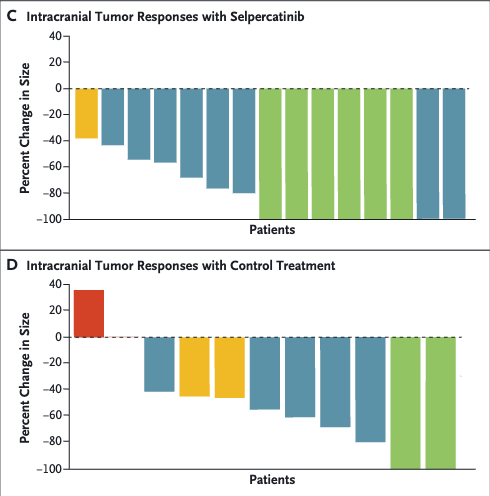
LIBRETTO trials
Selpercatinib

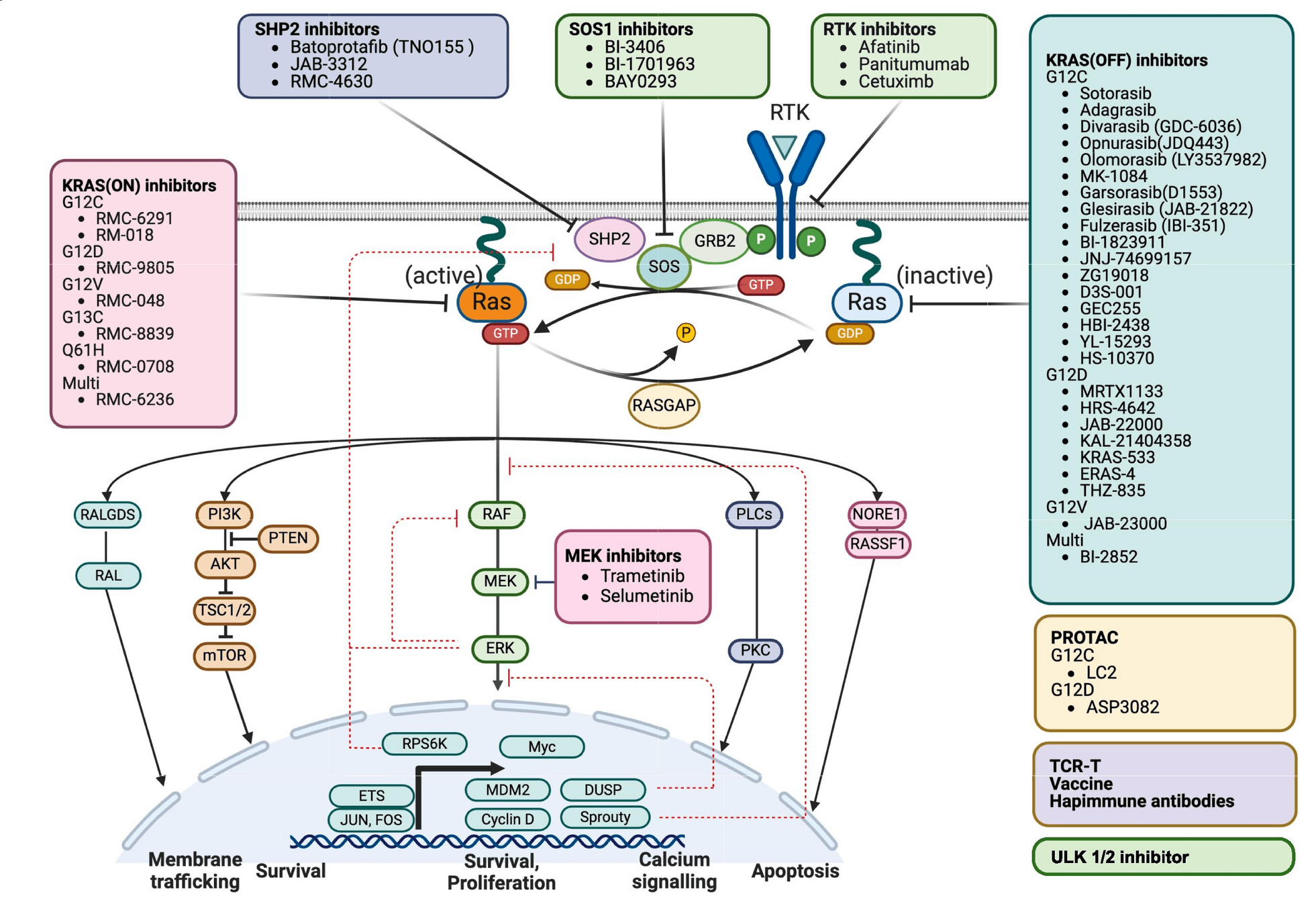
Drugs Targeting KRAS Mutations
- Examples: Sotorasib, Adagrasib.
- Mechanism: Inhibit KRAS G12C mutant protein, blocking downstream MAPK signaling.
-
Key Points:
- Sotorasib: First FDA-approved KRAS G12C inhibitor (CodeBreaK trials).
- Adagrasib: High CNS activity; promising in pretreated patients (KRYSTAL-1 trial).
-
Approval:
- Sotorasib: 2021 (CodeBreaK trials).
- Adagrasib: 2022 (KRYSTAL-1 trial).
Sources: CodeBreaK and KRYSTAL-1 trials.

Drugs Targeting MET Exon 14 Skipping
- Examples: Capmatinib, Tepotinib.
- Mechanism: Inhibit MET signaling to block tumor growth in MET exon 14 skipping mutations.
-
Key Points:
- Capmatinib: ORR ~40%, durable intracranial responses (GEOMETRY mono-1 trial).
- Tepotinib: High CNS activity and sustained efficacy (VISION trial).
-
Approval:
- Capmatinib: 2020 (GEOMETRY mono-1 trial).
- Tepotinib: 2021 (VISION trial).
Sources: GEOMETRY mono-1 and VISION trials.
The Role of TKIs in Early-Stage Disease
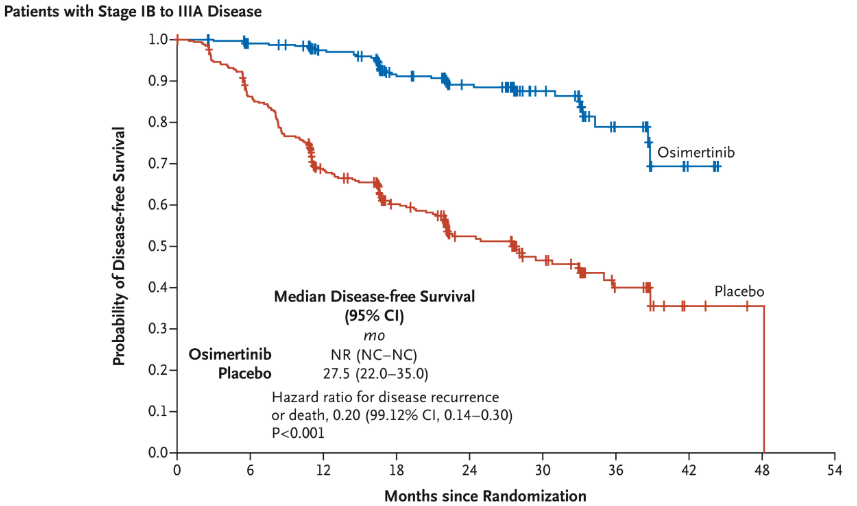
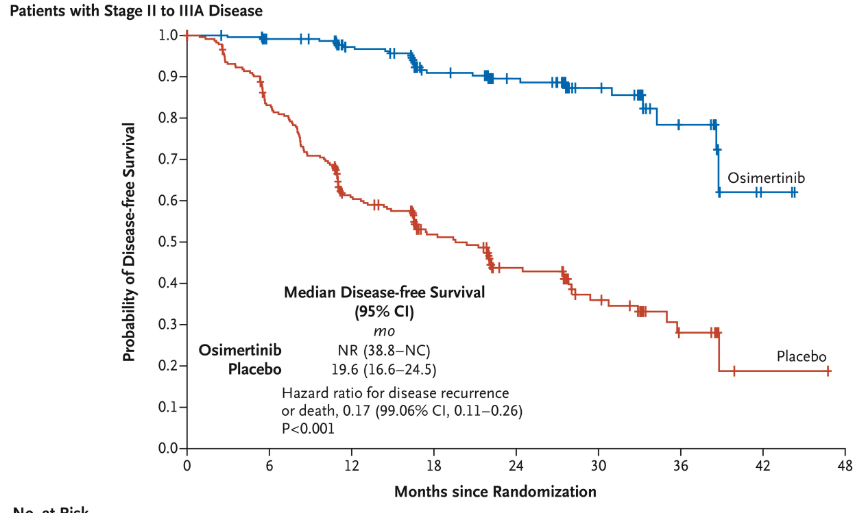
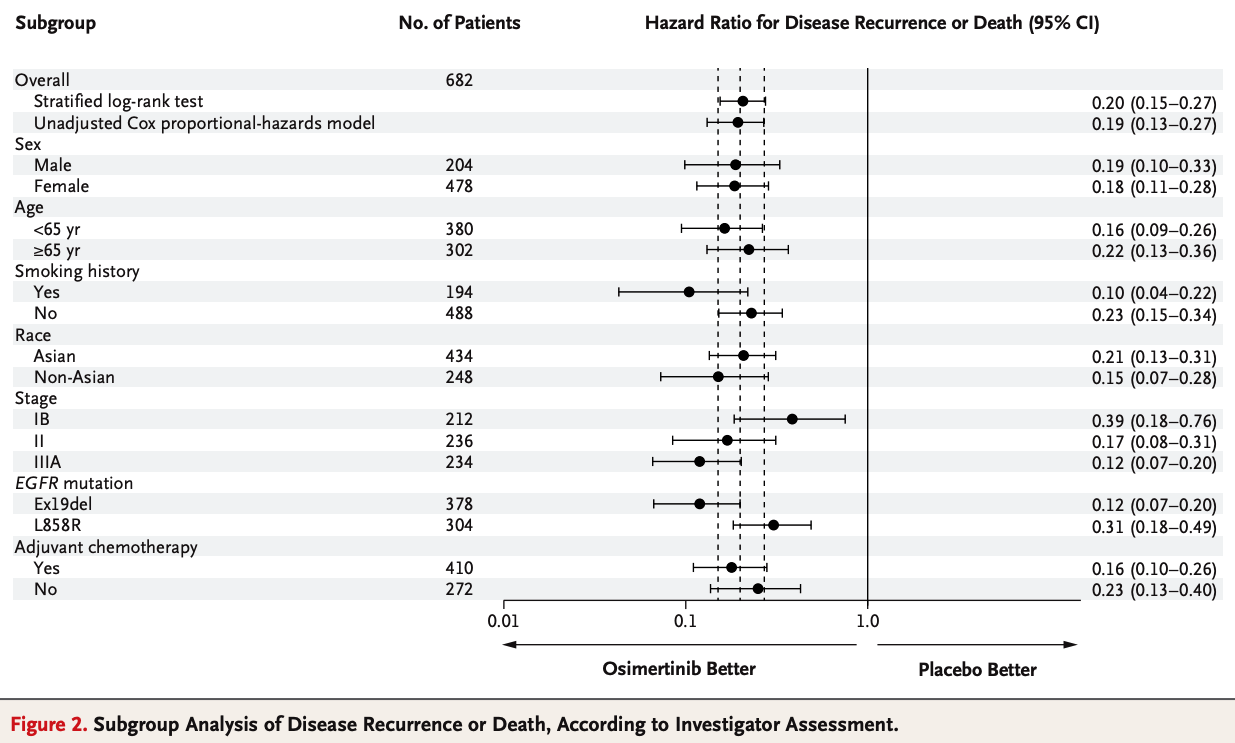
- Adjuvant Therapy: ADAURA trial demonstrated improved disease-free survival (DFS) with osimertinib in EGFR-mutated, resected NSCLC.
- Neoadjuvant Potential: Trials such as Blakely et al. suggest possible tumor reduction prior to surgery or radiation.
ADAURA Trial:
Inclusion Criteria:
- Stage IB-IIIA NSCLC with EGFR mutations (Exon 19 deletions or Exon 21 L858R).
- Complete tumor resection with or without adjuvant chemotherapy.
- Age ≥18 years with ECOG performance status ≤1.
Exclusion Criteria:
- Presence of unresectable or metastatic disease.
- Patients with prior EGFR TKI therapy or incomplete recovery post-surgery.
- Active, uncontrolled systemic illnesses.
Key Results:
- Disease-Free Survival (DFS): Median DFS not reached in osimertinib group vs. 19.6 months in placebo.
- Risk Reduction: 79% reduction in recurrence or death (HR = 0.21).
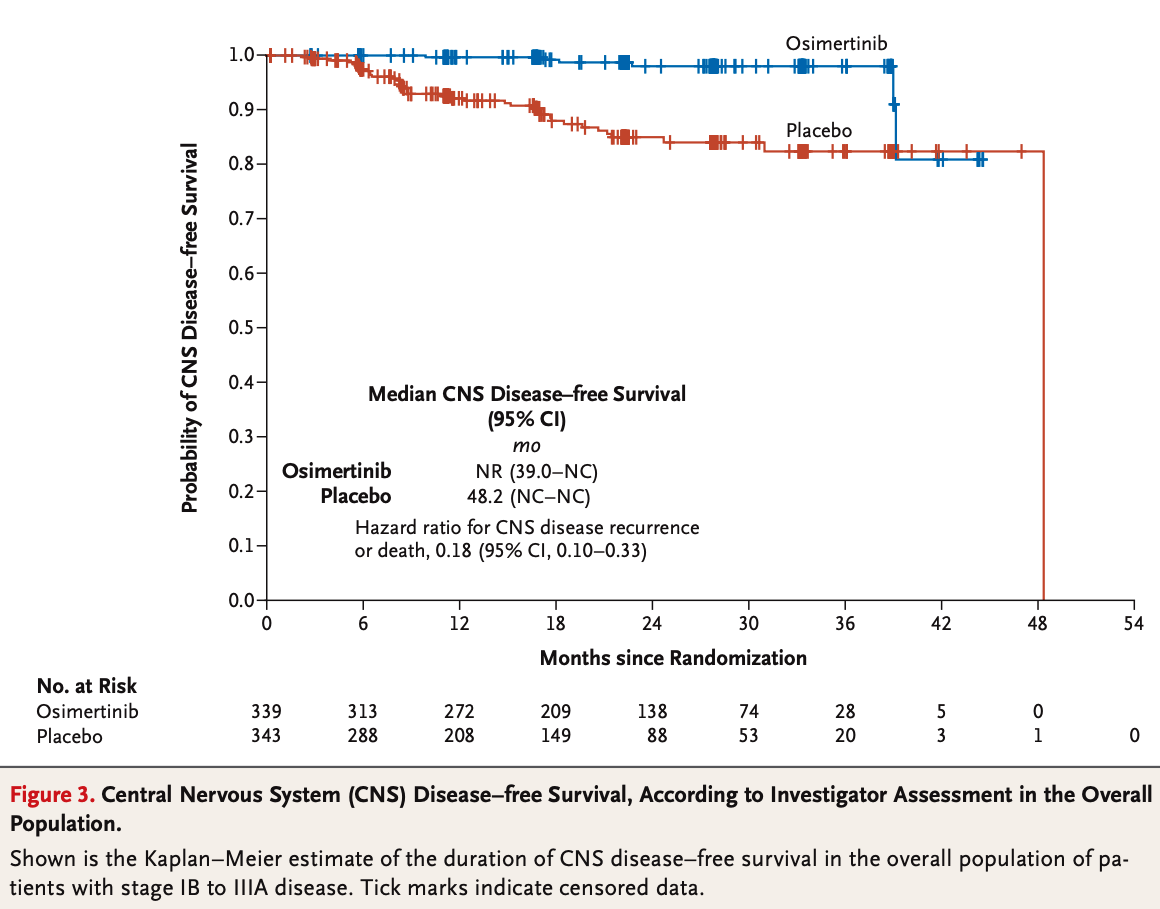
- Significant CNS Benefits: Reduced CNS recurrence in osimertinib group.
Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med 2020;383:1711-1723. https://doi.org/10.1056/NEJMoa2027071
ADAURA Trial: Methods and Patient Flow
Methods:
- Study Design: Randomized, double-blind, placebo-controlled, phase III trial.
- Population: Stage IB-IIIA EGFR-mutated NSCLC (Exon 19 deletions or L858R mutations).
-
Local Therapy Requirements:
- Patients underwent **complete surgical resection** of their primary tumor prior to enrollment.
- Adjuvant chemotherapy was allowed but not required, with regimens guided by institutional standards.
- Radiation therapy was not mandated but could be utilized as part of the institutional post-surgical care plan before trial enrollment.
- Intervention: Adjuvant osimertinib (80 mg daily) vs. placebo for up to 3 years
- Monitoring: Imaging every 12 weeks for 2 years, then every 24 weeks thereafter.
Patients with Stage IB-IIIA EGFR-Mutated NSCLC
Complete Surgical Resection (± Adjuvant Chemotherapy)
Randomization (1:1)
Arm A: Osimertinib (80 mg daily)
Adjuvant therapy for up to 3 years
Arm B: Placebo
Observation for up to 3 years
Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med, 2020;383:1711-1723. https://doi.org/10.1056/NEJMoa2027071
Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med 2020;383:1711-1723. https://doi.org/10.1056/NEJMoa2027071
Wu YL, Tsuboi M, He J, et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med 2020;383:1711-1723. https://doi.org/10.1056/NEJMoa2027071
Neoadjuvant TKIs: Reducing Tumor Burden
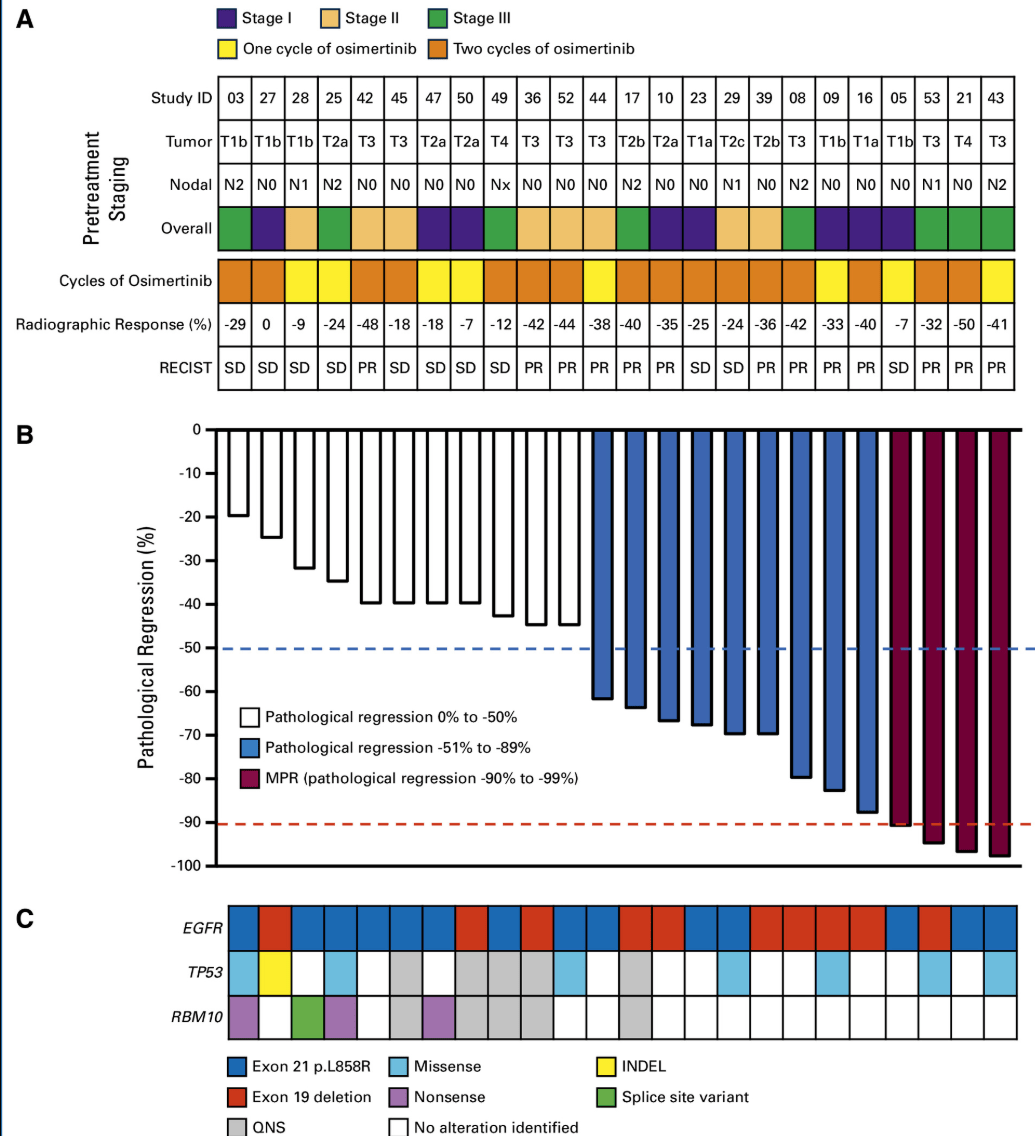
- Trial Design: Phase II trial evaluated neoadjuvant osimertinib in Stage II-IIIA EGFR-mutated NSCLC.
Inclusion Criteria:
- Stage IB-IIIA EGFR-mutated NSCLC.
- No prior systemic therapy or TKI use.
- Age ≥18 years with ECOG performance status ≤1.
Exclusion Criteria:
- Presence of unresectable or metastatic disease.
- Inability to tolerate TKIs or planned surgery.
- Active, uncontrolled systemic illnesses.
Key Results:
- Pathologic Complete Response (pCR): 0%.
- Major Pathologic Response: Observed in 15% of patients.
- Potential DFS Benefits: Extended progression-free survival with osimertinib.
Take away: Lack of pathologic complete responses (pCR) highlights need for combination strategies.
Blakely Trial: Methods and Patient Flow
Methods:
- Study Design: Phase II, single-arm trial evaluating neoadjuvant osimertinib for resectable EGFR-mutated NSCLC.
- Population: Stage II-IIIA EGFR-mutated NSCLC (Exon 19 deletions or L858R mutations).
-
Local Therapy Requirements:
- Patients must have resectable disease.
- Definitive surgical resection planned following neoadjuvant therapy.
- Adjuvant therapy was determined based on post-surgical outcomes.
- Intervention: Neoadjuvant osimertinib (80 mg daily) for 6-12 weeks prior to surgery.
-
Endpoints:
- Primary: Pathologic response rate, including complete and partial pathologic responses.
- Secondary: Radiographic response, disease-free survival (DFS), and overall survival (OS).
- Monitoring: Imaging at baseline, during treatment, and before surgery. Pathologic assessment post-resection.
Patients with Stage II-IIIA EGFR-Mutated NSCLC
Neoadjuvant Osimertinib (6-12 Weeks)
Definitive Surgical Resection
Adjuvant Therapy (Based on Pathology)
Blakely CM, et al. Neoadjuvant Osimertinib for Stage II-IIIA EGFR-Mutated NSCLC: A Phase II Study. J Clin Oncol, 2024;42:3105-3114. https://doi.org/10.1200/JCO.24.00071
The Role of TKIs in Locally Advanced NSCLC
-
Current NCCN Standard:
- Concurrent chemoradiotherapy (CCRT) is the preferred treatment for all patients with locally advanced NSCLC.
- Consolidation immunotherapy with durvalumab is the standard for patients without contraindications.
-
TKIs in EGFR/ALK-Positive NSCLC:
- Molecular profiling is strongly recommended, but targeted therapy with TKIs is not yet integrated into the concurrent chemoradiation paradigm.
- Emerging studies like LAURA are investigating the role of adjuvant osimertinib post-CCRT for EGFR-mutated NSCLC.
-
Future Directions:
- Trials are evaluating whether TKIs can replace or augment current standards such as durvalumab.
- Key challenge: Balancing systemic and local control with minimal toxicity.
NCCN Guidelines for NSCLC, 2023. Website
Antonia SJ et al., N Engl J Med, 2017. PACIFIC Trial
Peled Trial: Design and Patient Flow
Inclusion Criteria:
- Stage III EGFR-mutant NSCLC (Exon 19 deletion or L858R mutation).
- Performance status 0–1.
- Amenable to definitive chemoradiation or surgery.
Exclusion Criteria:
- EGFR TKI-resistant mutations (e.g., exon 20 insertion).
- Significant comorbidities (e.g., interstitial lung disease).
- Major surgery within 4 weeks before enrollment.
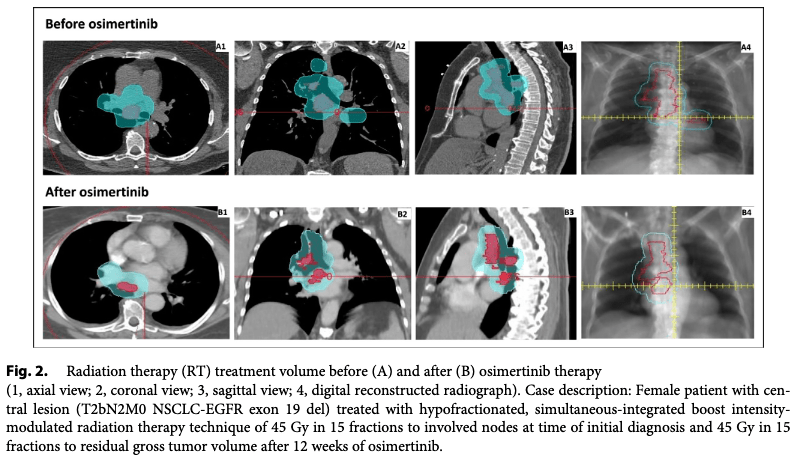
Timing of Radiation Therapy:
- Radiation therapy initiated after 12 weeks of neoadjuvant osimertinib for responders or stable disease.
- RT planning adapted to changes in tumor and nodal volume (based on GTV and PTV reduction).
- Patients with limited response received chemoradiation instead.
Patients with Stage III EGFR-Mutant NSCLC (Exon 19/L858R)
Neoadjuvant Osimertinib (12 Weeks)
Arm A: Response or Stable Disease
Definitive Radiation Therapy and/or Surgery
Arm B: Limited Response
Chemoradiation Therapy
Peled N, et al. Neoadjuvant Osimertinib Followed by Sequential Definitive Radiation Therapy and/or Surgery in Stage III EGFR-Mutant NSCLC. Int J Radiat Oncol Biol Phys, 2023. https://doi.org/10.1016/j.ijrobp.2023.03.042
Peled Trial: Methods and Protocols
- Intervention: Osimertinib 80 mg daily for 12 weeks.
- Endpoints Primary: Objective response rate (ORR) via RECIST v1.1.
- Secondary: Gross tumor volume (GTV) reduction, circulating tumor DNA (ctDNA) dynamics, and safety.
-
Definitive Therapy:
- RT and/or surgery based on post-osimertinib response. (60Gy/30fx or 45Gy/15fx)
- Patients with limited response received chemoradiation.
- Monitoring: PET-CT scans and ctDNA at baseline, 6 weeks, and 12 weeks.
Peled N, et al. Neoadjuvant Osimertinib Followed by Sequential Definitive Radiation Therapy and/or Surgery in Stage III EGFR-Mutant NSCLC. Int J Radiat Oncol Biol Phys, 2023. https://doi.org/10.1016/j.ijrobp.2023.03.042
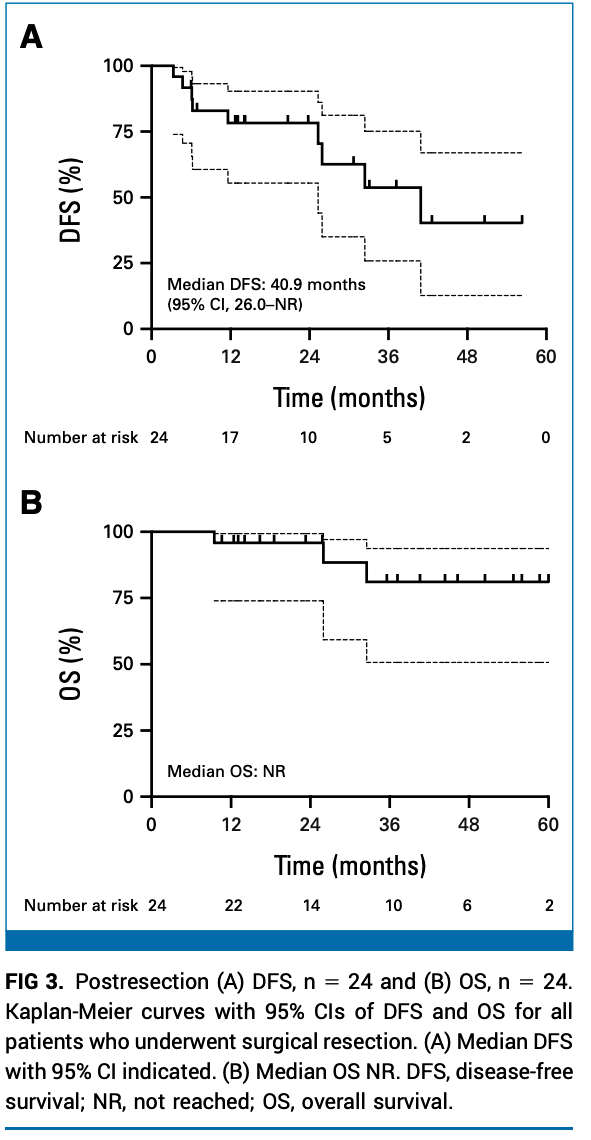
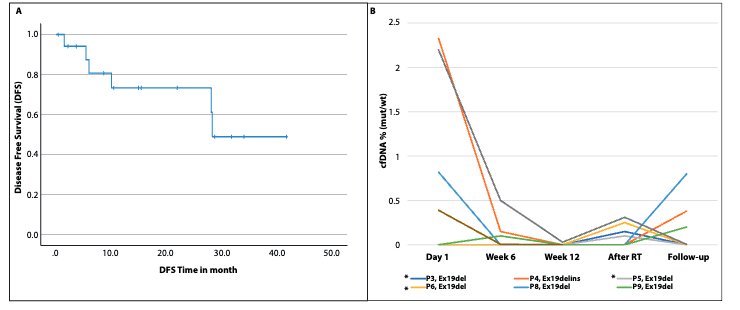
Peled Trial: Key Results
- ORR: 95.2% (17 partial responses, 2 complete responses).
-
Tumor Volume Reduction:
- Median GTV reduction: 48% (P = 0.02).
- Median PTV reduction: 31% (P = 0.01).
-
Surgical Outcomes:
- 3 patients underwent surgery; 1 achieved pathologic complete response.
-
ctDNA:
- Detected in 5 patients; 4 became negative during osimertinib therapy.
Peled N, et al. Neoadjuvant Osimertinib Followed by Sequential Definitive Radiation Therapy and/or Surgery in Stage III EGFR-Mutant NSCLC. Int J Radiat Oncol Biol Phys, 2023. https://doi.org/10.1016/j.ijrobp.2023.03.042
Critiques of the Peled Trial
-
Strengths:
- High ORR (95.2%) demonstrates osimertinib's efficacy as neoadjuvant therapy.
- Significant reduction in tumor volumes improved RT planning.
-
Limitations:
- Small sample size (N=24).
- No control arm to compare against standard chemoradiation or surgery outcomes.
-
Unanswered Questions:
- Long-term survival data are still limited.
- How to integrate osimertinib with existing treatments (e.g., durvalumab).
Peled N, et al. Neoadjuvant Osimertinib Followed by Sequential Definitive Radiation Therapy and/or Surgery in Stage III EGFR-Mutant NSCLC. Int J Radiat Oncol Biol Phys, 2023. https://doi.org/10.1016/j.ijrobp.2023.03.042
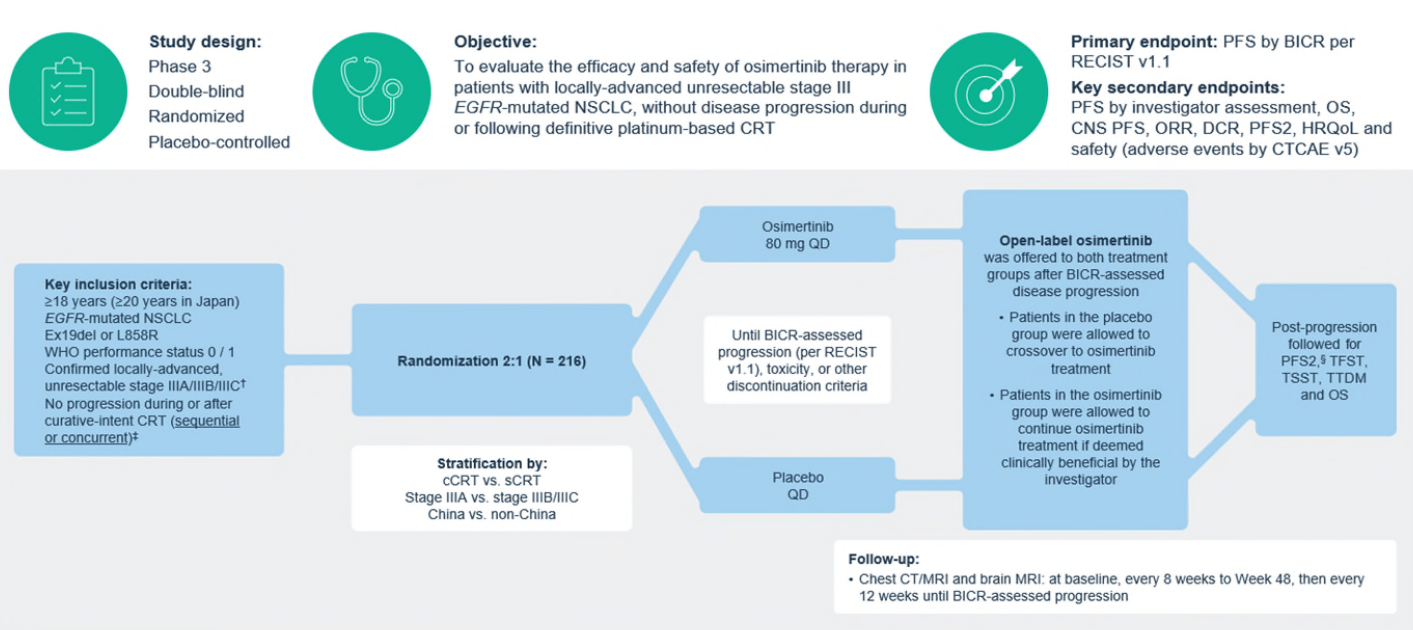
LAURA Trial: Design and Enrollment
Inclusion Criteria:
- Unresectable stage III NSCLC with EGFR exon 19 deletions or exon 21 L858R mutation.
- Completed platinum-based chemoradiotherapy (concurrent or sequential).
- No progression during or after definitive chemoradiotherapy.
- WHO performance status 0-1.
Exclusion Criteria:
- History of interstitial lung disease or unresolved grade ≥2 adverse effects post-chemoradiotherapy.
- Symptomatic pneumonitis after chemoradiotherapy.
- Patients with mutations other than EGFR exon 19 or exon 21.
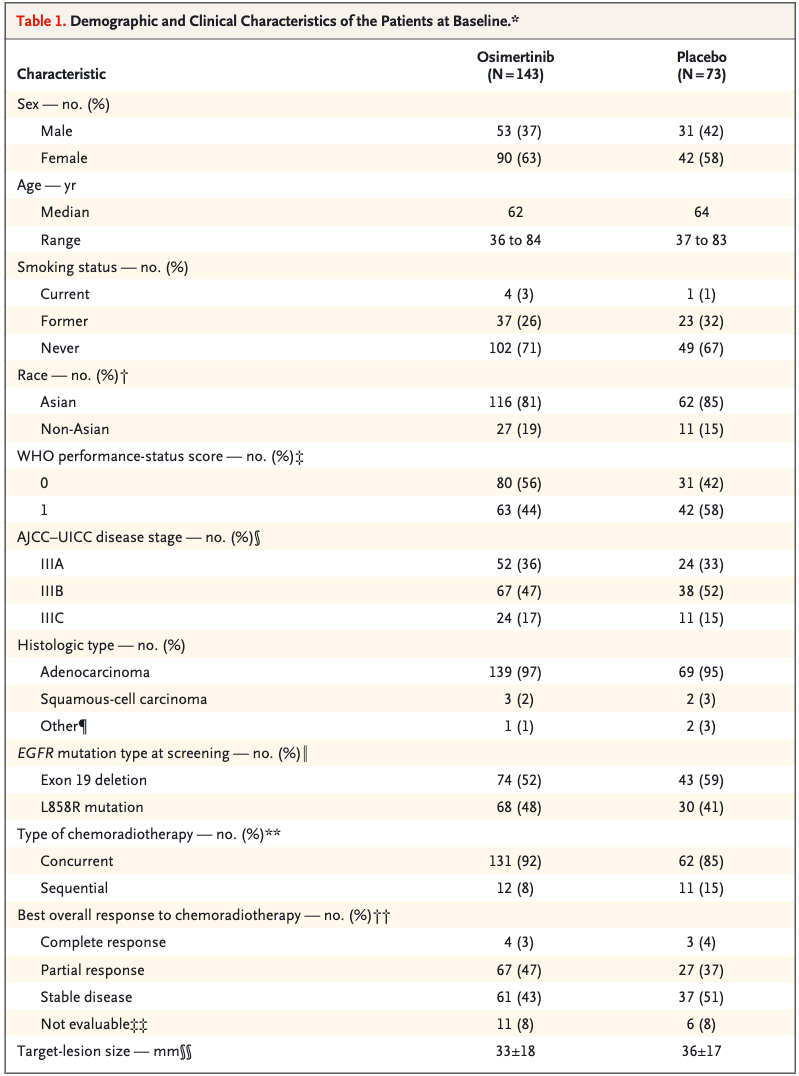
Patient Characteristics:
- Total patients: 216 randomized (143 osimertinib, 73 placebo).
- Most received **concurrent chemoradiotherapy**: 92% (osimertinib), 85% (placebo).
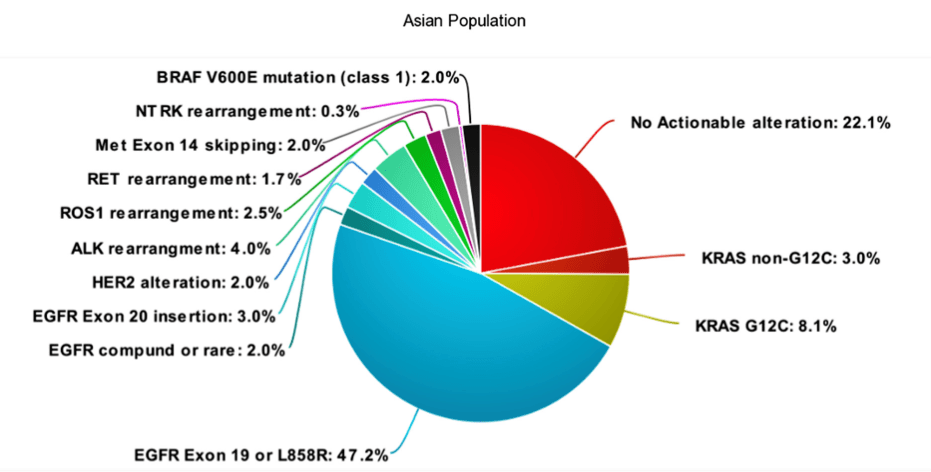
- Majority were Asian (81% osimertinib, 85% placebo).
- Performance status of 0: 56% (osimertinib) vs. 42% (placebo).
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
LAURA Trial: Design and Patient Flow
Patients with unresectable stage III EGFR-mutated NSCLC
Randomization (2:1)
Arm A: Osimertinib (80 mg daily)
Until Disease Progression
Arm B: Placebo
Until Disease Progression
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
Timing of TKI Initiation in LAURA Trial
- Timing: TKI started within 6 weeks of completing chemoradiotherapy.
- Concurrent Chemoradiotherapy: 92% of osimertinib and 85% of placebo patients received concurrent therapy.
- Sequential Chemoradiotherapy: Smaller proportion: 8% (osimertinib) vs. 15% (placebo).
- Post-Treatment Monitoring: Regular imaging every 8 weeks (up to 48 weeks) and every 12 weeks thereafter.
Impact of Timing:
- Patients initiating osimertinib immediately after chemoradiotherapy achieved significant CNS progression-free survival benefits.
- No subgroup differences identified between concurrent and sequential chemoradiotherapy timing.
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
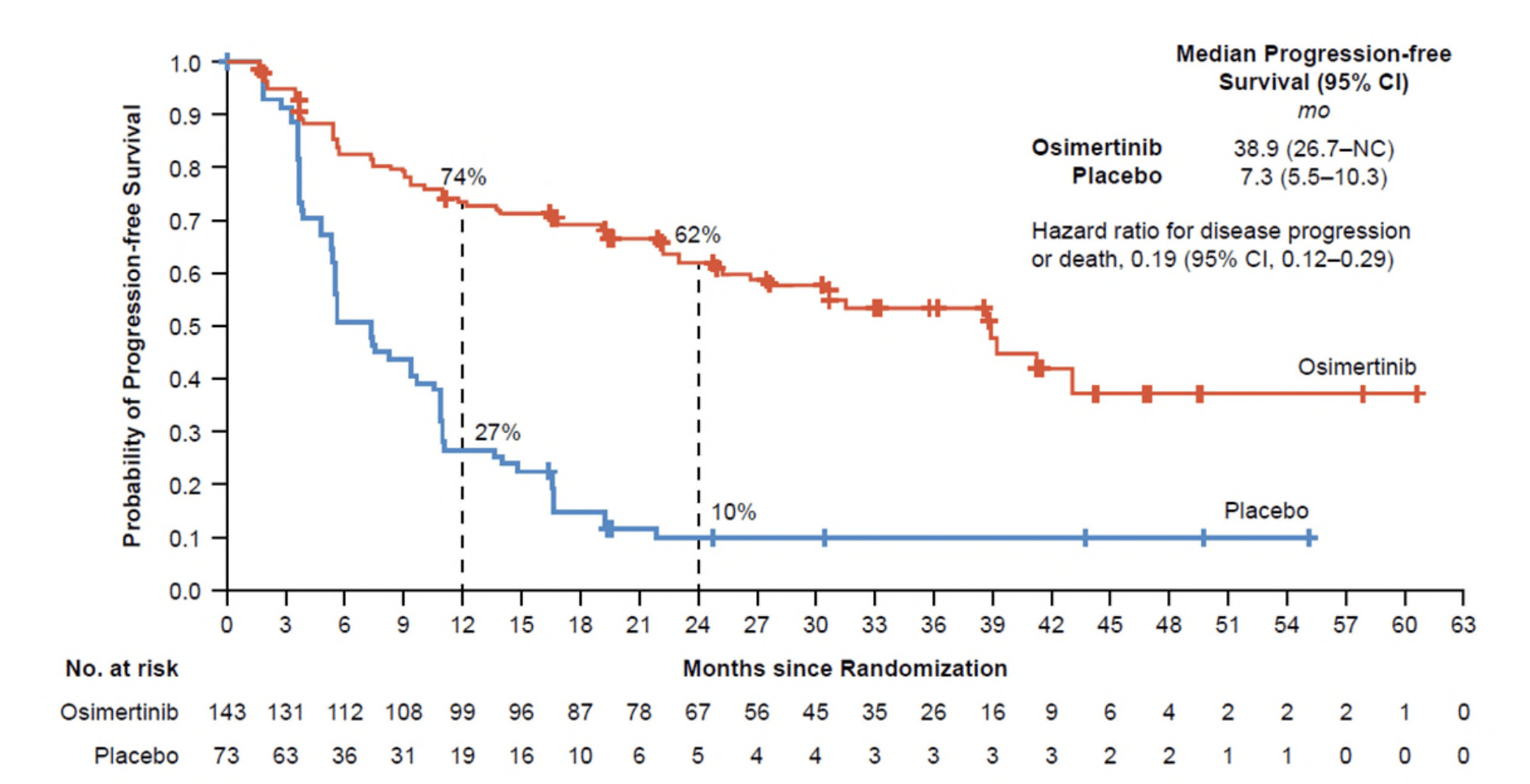
LAURA Trial: Key Results
- PFS: Median 39.1 months (osimertinib) vs. 5.6 months (placebo); HR 0.16 (P<0.001).
- CNS Progression: New brain metastases: 8% (osimertinib) vs. 29% (placebo).
- Safety: Grade ≥3 adverse events: 35% (osimertinib) vs. 12% (placebo).
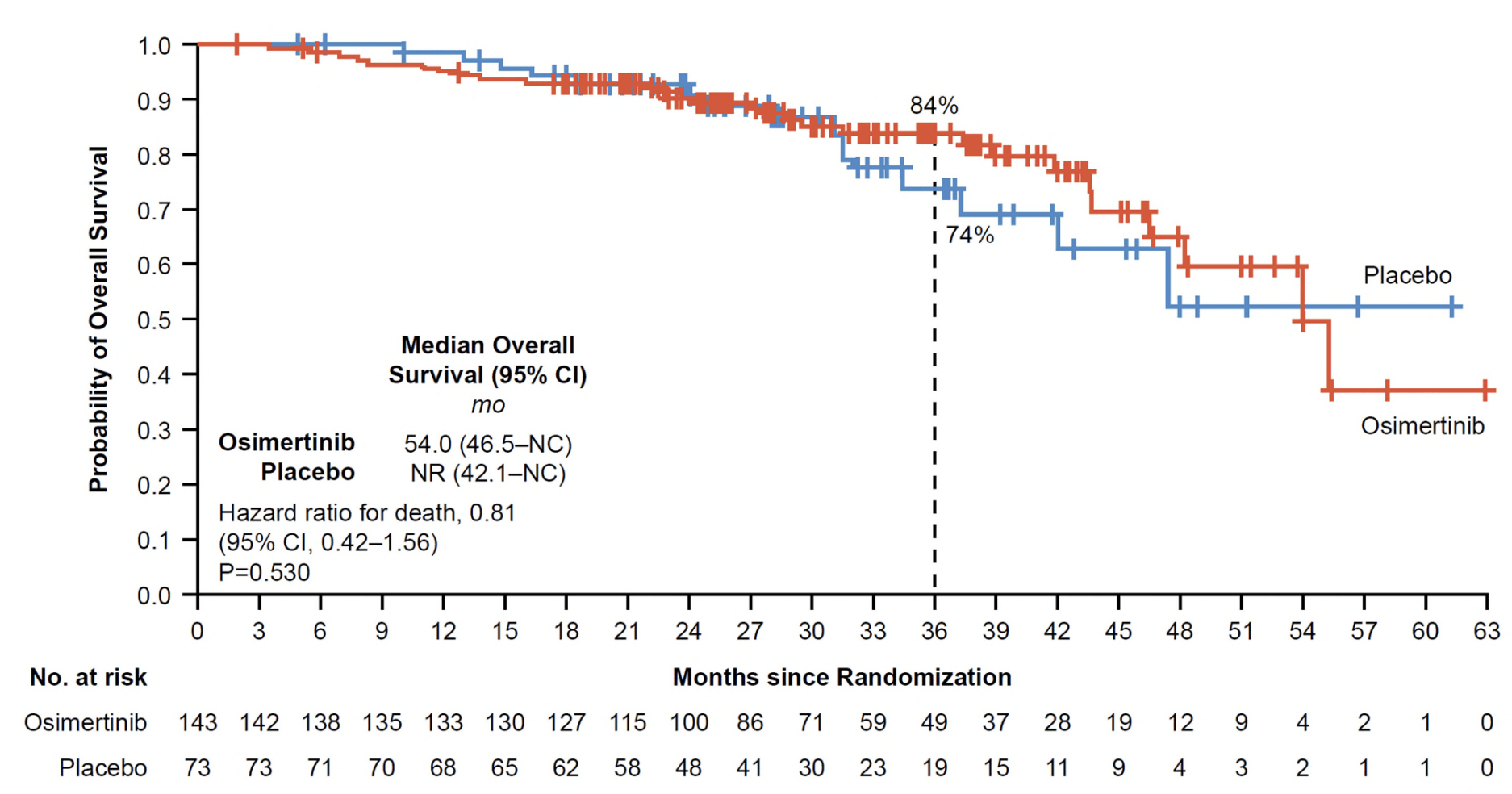
- OS (Interim): 84% (osimertinib) vs. 74% (placebo) at 36 months (HR 0.81, P=0.53).
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
LAURA Trial: Key Results
- PFS: Median 39.1 months (osimertinib) vs. 5.6 months (placebo); HR 0.16 (P<0.001).
- CNS Progression: New brain metastases: 8% (osimertinib) vs. 29% (placebo).
- Safety: Grade ≥3 adverse events: 35% (osimertinib) vs. 12% (placebo).
- OS (Interim): 84% (osimertinib) vs. 74% (placebo) at 36 months (HR 0.81, P=0.53).
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
LAURA Trial: Key Results
- PFS: Median 39.1 months (osimertinib) vs. 5.6 months (placebo); HR 0.16 (P<0.001).
- CNS Progression: New brain metastases: 8% (osimertinib) vs. 29% (placebo).
- Safety: Grade ≥3 adverse events: 35% (osimertinib) vs. 12% (placebo).
- OS (Interim): 84% (osimertinib) vs. 74% (placebo) at 36 months (HR 0.81, P=0.53).
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
LAURA Trial: Toxicities
Radiation Pneumonitis
-
Incidence:
- Osimertinib: 48%
- Placebo: 38%
-
Severity:
- Most cases were Grade 1–2.
- Grade 3: 2% (osimertinib) vs. 0% (placebo).
- No Grade 4 or 5 events were reported.
- Statistical Significance: Difference in incidence was not statistically significant.
Interstitial Lung Disease (ILD)
-
Incidence:
- Osimertinib: 8%
- Placebo: 1%
-
Severity:
- Most cases were Grade 1–2.
- Attributed primarily to pneumonitis.
- Statistical Significance: Not specified, but clinically relevant difference noted.
Management:
- Most radiation pneumonitis and ILD cases resolved with supportive care.
- Guidelines allowed continuation of osimertinib for mild to moderate symptoms.
Lu S, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024. https://doi.org/10.1056/NEJMoa2402614
Critiques of the LAURA Trial
-
Unanswered Questions:
- Is osimertinib superior to durvalumab for this population?
- What is the optimal duration of osimertinib therapy?
-
Applicability Concerns:
- Heavy Asian patient representation; results may not generalize globally.
- Exclusion of patients with unresolved post-chemoradiotherapy toxicities.
-
Strengths:
- Robust CNS control and extended PFS benefit.
- Well-designed phase III trial with placebo control.
Lu S, Kato T, Dong X, et al. Osimertinib After Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N Engl J Med, 2024.
TKIs and Radiotherapy in Oligometastatic NSCLC
- Established Role: TKIs remain standard for oncogene-driven NSCLC (EGFR, ALK, ROS1 mutations).
-
Focus: Synergistic integration of TKIs and radiotherapy:
- Upfront Radiotherapy: Prolonged survival demonstrated in trials combining SBRT with systemic TKIs.
- Oligoprogression: Radiotherapy targets isolated progression sites while TKIs continue to control systemic disease.
-
Key Trials:
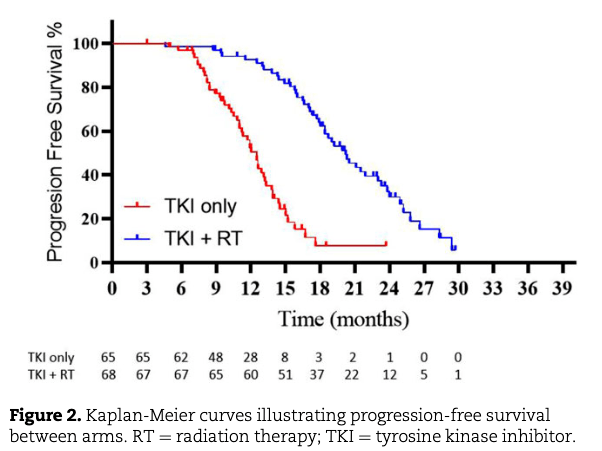
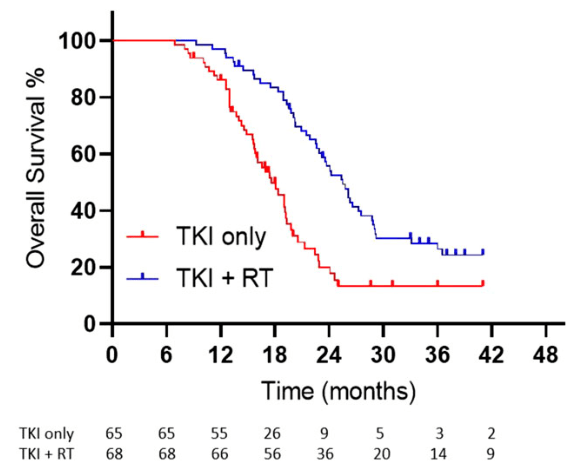
- SINDAS Trial: EGFR-mutant NSCLC, OS benefit with upfront SBRT + TKIs (25.5 vs. 17.4 months).
- Peled et al., 2023: Investigated SBRT with osimertinib in EGFR+ oligometastatic NSCLC
- NORTHSTAR Trial: Evaluating consolidative SBRT with osimertinib in EGFR-mutant NSCLC
Wang et al., J Natl Cancer Inst, 2022. SINDAS Trial
Peled et al., 2023. SBRT + Osimertinib
NORTHSTAR Study, ClinicalTrials.gov. NCT03410043
SINDAS Trial: Study Design and Patient Flow
Inclusion Criteria:
- EGFR-mutated NSCLC (Exon 19 deletions or L858R mutations).
- 1-5 synchronous oligometastases (confirmed by imaging).
- No prior therapy for metastatic disease.
- ECOG performance status ≤1.
Exclusion Criteria:
- Brain metastases.
- Concurrent severe illnesses or contraindications to radiotherapy.
Enrolled Population:
- 73% of metastases were bone lesions.
- Median age: 60 years; more patients in the RT+TKI arm had >2 metastases.
Timing of Radiation Therapy:
- Radiotherapy delivered upfront to primary tumor, involved nodes, and oligometastases (25-40 Gy in 1-5 fractions).
- Radiotherapy occurred **prior to TKI initiation** in patients with synchronous metastases.
- No radiotherapy was allowed in the TKI-alone arm until disease progression.
Wang XS, Bai YF, Verma V, et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With or Without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. JNCI, 2022. https://doi.org/10.1093/jnci/djac015
SINDAS Trial: Trial Design and Patient Flow
Patients with EGFR+ NSCLC (1-5 oligometastases)
Randomization
Arm A: TKI Alone
Palliative RT Allowed Only at Progression
Arm B: TKI + Upfront RT
25-40 Gy in 5 Fractions to All Sites
Methods:
-
Radiotherapy: Delivered to all sites, including:
- Primary tumor and involved mediastinal lymph nodes.
- All oligometastatic sites (up to 5).
- Uniform Fractionation: 25-40 Gy in 5 fractions, including mediastinal nodes (unconventional for central structures).
- Techniques: SBRT, VMAT, or IMRT with constraints for adjacent organs (e.g., mean dose <16.5 Gy for trachea/bronchus).
Wang XS, Bai YF, Verma V, et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With or Without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. JNCI, 2022. https://doi.org/10.1093/jnci/djac015
SINDAS Trial: 5 Fx Dose Constraints
| Structure | Dose Constraint |
|---|---|
| Trachea/Bronchus | Mean dose ≤ 16.5 Gy |
| Heart | V30 ≤ 5 cc (Volume receiving ≥ 30 Gy) |
| Esophagus | V30 ≤ 5 cc |
| Spinal Cord | Maximum dose ≤ 30 Gy |
| Lungs | V20 ≤ 30% (Volume receiving ≥ 20 Gy) |
| Ribs | V30 ≤ 5 cc |
| Liver | Mean dose ≤ 28 Gy |
| Kidneys | Mean dose ≤ 20 Gy |
Wang XS, Bai YF, Verma V, et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With or Without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. JNCI, 2022. https://doi.org/10.1093/jnci/djac015
SINDAS Trial: Results
Key Results:
- TKIs Used: Gefitinib, Erlotinib, or Icotinib (Osimertinib not available).
- Median OS: 25.5 vs. 17.4 months (p < 0.001).
- Median PFS: 20.2 vs. 12.5 months (p < 0.001).
- Local Control (LC): 91% (RT+TKI) vs. 55% (TKI only).
- Toxicity: Grade 3-4 pneumonitis: 6% (RT+TKI), no grade 5 toxicity.
Wang XS, Bai YF, Verma V, et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With or Without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. JNCI, 2022. https://doi.org/10.1093/jnci/djac015
SINDAS Trial: Toxicities
Radiation Pneumonitis
-
Incidence:
- RT+TKI Group: 6% (Grade 3–4).
- TKI-Only Group: 0% (Grade 3–4).
-
Severity:
- Most cases were mild (Grade 1–2).
- No Grade 5 events were reported.
-
Management:
- Resolved with corticosteroids and supportive care.
Other Toxicities
-
Fatigue:
- Reported in both arms, with higher rates in RT+TKI group.
-
Dermatologic and GI Toxicities:
- Consistent with known profiles of first-generation TKIs (e.g., gefitinib, erlotinib).
- Rash and diarrhea were the most common.
-
Overall Safety:
- No significant increase in Grade ≥3 toxicities between arms.
- No treatment-related deaths reported.
Overall Toxicity Profile:
- Radiotherapy in combination with TKIs was generally well-tolerated.
- Low rates of severe toxicities suggest safety of this approach with appropriate management.
Wang XS, Bai YF, Verma V, et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With or Without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. JNCI, 2022. https://doi.org/10.1093/jnci/djac015
Critiques of the SINDAS Trial
- Outdated Systemic Therapy: Used first-generation TKIs (gefitinib, erlotinib, icotinib) instead of third-generation osimertinib, now the standard for EGFR-mutated NSCLC.
- Early Trial Closure: Lacked prespecified stopping criteria, raising concerns about long-term data robustness.
- Unconventional RT Protocol: Uniformly used 5-fraction RT for all sites, including mediastinal lymph nodes and primary tumor, which is not standard practice.
- Exclusion of Brain Metastases: Limited applicability in an era where CNS-penetrant TKIs (e.g., osimertinib) are standard.
- Inadequate Staging: PET imaging not uniformly used, potentially missing occult metastases.
- Timing of Radiotherapy: Optimal timing of RT (upfront vs. delayed) remains unanswered.
Wang XS, Bai YF, Verma V, et al. Randomized Trial of First-Line Tyrosine Kinase Inhibitor With or Without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated NSCLC. JNCI, 2022. https://doi.org/10.1093/jnci/djac015
Milano MT, Salama JK, Chmura SJ. Should We Target Oligometastatic EGFR-Mutated NSCLC With Radiotherapy Before Targeted Therapy? JNCI, 2023. https://doi.org/10.1093/jnci/djac016
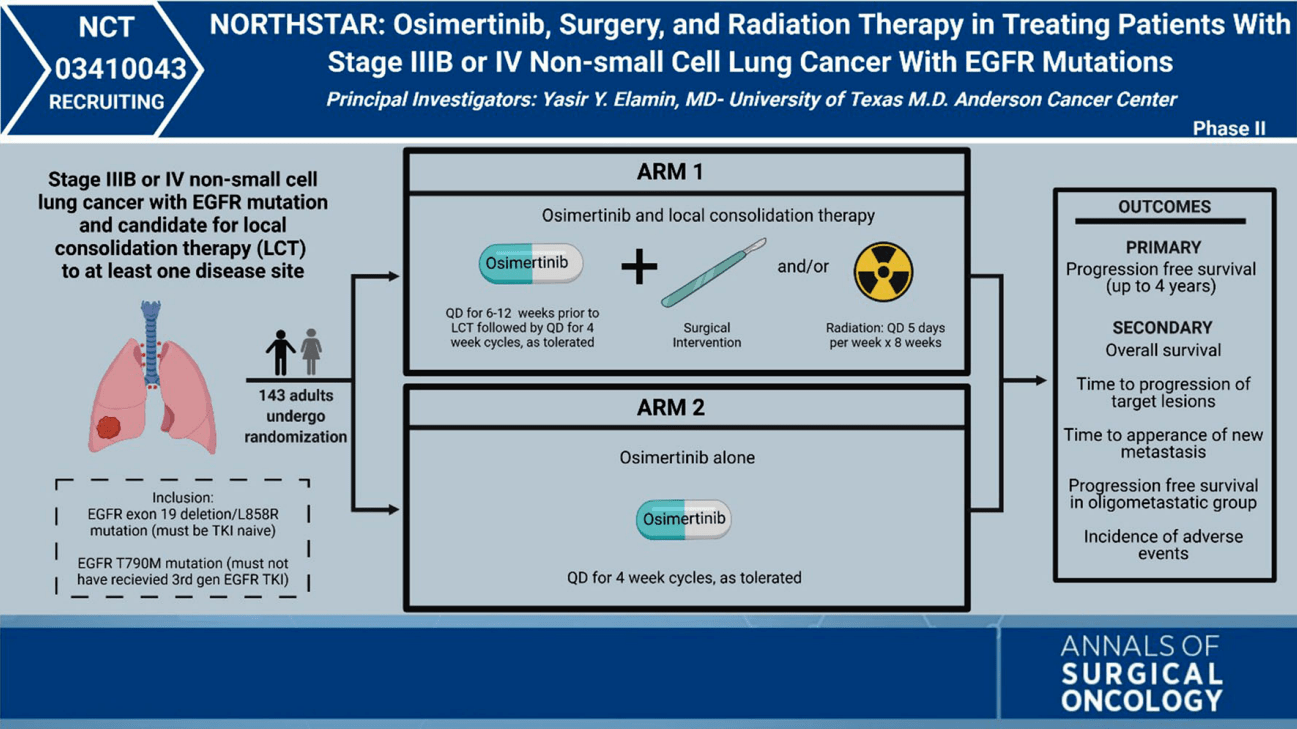
NORTHSTAR trial
NORTHSTAR Trial: Study Design and Patient Flow
Inclusion Criteria:
- Stage IIIB-IV EGFR-mutated NSCLC (Exon 19, L858R, or T790M mutations).
- Up to 3 metastases or TKI-naive/first-line osimertinib users.
- No progression after 6-12 weeks of induction osimertinib.
- ECOG performance status ≤1.
Exclusion Criteria:
- Prior osimertinib or third-generation EGFR TKIs.
- Symptomatic CNS metastases.
- Significant comorbidities (e.g., uncontrolled hypertension).
Enrolled Population:
- Induction osimertinib given to all patients for 6-12 weeks.
- Patients randomized to continue osimertinib alone or add consolidative RT (± surgery).
Timing of Radiation Therapy:
- RT delivered **after induction osimertinib** to target residual disease or consolidate response.
- Radiotherapy timing evaluated for toxicity and synergistic effects when combined with osimertinib.
- Designed for consolidative RT, not upfront therapy like in SINDAS.
NORTHSTAR Study Protocol, NCT03410043. ClinicalTrials.gov
Critiques of the NORTHSTAR Trial Design
Key Questions the Design Fails to Answer:
-
Timing of Radiotherapy:
- Does the benefit of consolidative RT differ from upfront RT as in the SINDAS trial?
- Should RT be delivered only after achieving systemic control with osimertinib?
-
Selection of Patients for RT:
- How should patients with oligoprogressive disease be stratified?
- Do patients with larger metastatic burdens benefit equally from consolidative RT?
Strengths and What It Solves:
- Inclusion of CNS Disease: The trial includes patients with limited brain metastases, addressing a key gap in prior studies like SINDAS.
- Modern Systemic Therapy: Incorporates osimertinib, a third-generation EGFR TKI with superior systemic and CNS efficacy.
- Focus on Consolidative RT: Evaluates RT in a setting that mirrors real-world practice, where systemic control is often achieved before considering RT.
- Improved RT Protocols: Standardizes RT techniques and fractionation schedules, improving reproducibility.
NORTHSTAR Study Protocol, NCT03410043. ClinicalTrials.gov
Milano MT, Salama JK, Chmura SJ. Should We Target Oligometastatic EGFR-Mutated NSCLC With Radiotherapy Before Targeted Therapy? JNCI, 2023. https://doi.org/10.1093/jnci/djac016
Comparative Analysis of Key Trials
| Trial | Population | Intervention | Key Outcomes | Toxicities |
|---|---|---|---|---|
| SINDAS | EGFR+ NSCLC, 1-5 oligometastases | RT (25-40 Gy in 5 Fx) + 1st Gen TKIs |
- OS: 25.5 vs. 17.4 months (p < 0.001) - Local control: 91% vs. 55% |
Grade 3-4 pneumonitis: 6% |
| LAURA | Stage III EGFR+ NSCLC | Osimertinib vs. Placebo |
- PFS: 39.1 vs. 5.6 months (HR: 0.16) - CNS progression: 8% vs. 29% |
- Pneumonitis: 48% vs. 38% - ILD: 8% vs. 1% |
| ADAURA | Stage IB-IIIA EGFR+ NSCLC | Adjuvant Osimertinib |
- DFS: HR 0.20 (99% CI: 0.14-0.30) - Significant CNS and systemic DFS benefits |
- No Grade 4/5 toxicities - Pneumonitis and rash observed |
| Blakely | Stage II-IIIA EGFR+ NSCLC | Neoadjuvant Osimertinib |
- ORR: ~50% - GTV/Pathologic response: No complete response - Median DFS: Promising but limited data |
- Rash and diarrhea observed - Mild pneumonitis reported |
| Peled | Stage III EGFR+ NSCLC | Neoadjuvant Osimertinib (12 weeks) |
- ORR: 95.2% - GTV reduction: 48% |
Mild pneumonitis reported |
Radiation vs TKIs for CNS Disease
-
When to Prioritize Radiation:
- Symptomatic metastases causing mass effect or impending herniation.
- Patients who progress intracranially on brain-penetrant TKIs.
-
When to Defer Radiation:
- Asymptomatic patients with high CNS penetrance of TKIs like osimertinib or alectinib.
- Patients with long-term systemic disease control on TKIs.
-
Clinical Evidence:
- Phase III studies demonstrate CNS activity with osimertinib and alectinib significantly reducing intracranial progression.
- Local therapy (SRS) improves intracranial control in conjunction with TKIs for large/multiple brain lesions.
CNS Penetration of Targeted Therapies in NSCLC
EGFR TKIs
ALK TKIs
ROS1 TKIs
Other TKIs
Limited (<5%)
Moderate (5-10%)
High (>10%)
Weller M. Central nervous system metastases in advanced non-small cell lung cancer: A review of the therapeutic landscape. Cancer Treat Rev, 2024;130:102807. https://doi.org/10.1016/j.ctrv.2024.102807
Radiation vs TKIs for CNS Disease
-
When to Prioritize Radiation:
- Symptomatic metastases causing mass effect or impending herniation.
- Patients who progress intracranially on brain-penetrant TKIs.
-
When to Defer Radiation:
- Asymptomatic patients with high CNS penetrance of TKIs like osimertinib or alectinib.
- Patients with long-term systemic disease control on TKIs.
-
Clinical Evidence:
- Phase III studies demonstrate CNS activity with osimertinib and alectinib significantly reducing intracranial progression.
- Local therapy (SRS) improves intracranial control in conjunction with TKIs for large/multiple brain lesions.
Mutation-Specific Failure Patterns
-
EGFR Mutations:
- Exon 19 deletions: Longer PFS and OS compared to Exon 21 L858R.
- Common CNS progression due to limited blood-brain barrier penetration by early TKIs.
- ALK Rearrangements: CNS failures dominate despite newer TKIs like lorlatinib.
- ROS1 Fusions: Less CNS failure compared to ALK or EGFR mutations, especially with entrectinib.
- KRAS G12C: Primarily systemic progression. Emerging combinatorial strategies under investigation.
Duration of Control Before Failure
- EGFR: Median PFS ~19 months with osimertinib; systemic failures dominate thereafter.
- ALK: Median PFS ~35 months with next-generation TKIs (e.g., alectinib).
- Post-Failure Strategies: Oligoprogression can be managed with local radiation while continuing systemic TKIs.
Patterns of Failure in Oncogene-Addicted NSCLC
-
Distant Failures:
- EGFR-mutated NSCLC: Predominantly systemic progression (e.g., T790M resistance). Median PFS with osimertinib ~19 months.
- ALK-positive NSCLC: CNS metastases dominate. Alectinib reduces CNS progression risk but doesn’t eliminate it.
- Local Failures: Typically observed in cases of oligoprogression or resistant residual disease.
Best Practices for Oncogene-Driven NSCLC
-
Comprehensive Molecular Testing:
- Test for EGFR, ALK, ROS1, RET, MET, NTRK, KRAS mutations.
- Incorporate liquid biopsies and ctDNA for real-time monitoring.
-
Integrating Radiation and Systemic Therapy:
- For oligometastatic disease, consider RT + TKIs (e.g., SINDAS trial).
- In locally advanced settings, can use concurrent RT (e.g., LAURA trial).
-
CNS Management:
- Use CNS-penetrant therapies (e.g., osimertinib, lorlatinib).
- Consider SRS over WBRT where appropriate.
-
Toxicity Management:
- Monitor and manage pneumonitis and ILD proactively.
- Adapt treatment plans to minimize adverse events.
-
Oligometastatic Disease:
- Continued role for SBRT to enhance local control in patients responding to TKIs.
- Potential synergy between RT and systemic therapies in CNS metastases management.
-
Locally Advanced Disease:
- Consolidative RT remains critical in patients with partial responses to systemic therapies.
- Exploration of concurrent TKI and RT to minimize disease recurrence.
-
Future Research Directions:
- Defining the optimal timing and sequencing of local and systemic therapies.
- Randomized trials to assess long-term survival benefits of RT in patients on modern TKIs.
Hendriks LEL, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primers. 2024;10:71. https://doi.org/10.1038/s41572-024-00551-9
The Future of Oncogene-Driven NSCLC
-
Combining Systemic Therapies:
- Exploring the synergistic potential of TKIs with immunotherapies, particularly in oligometastatic and locally advanced disease.
- Optimal sequencing and timing of immunotherapy alongside radiation and targeted therapies.
-
Refining Patient Selection:
- Biomarker-driven approaches to identify patients who benefit most from combination therapies.
- Real-time monitoring using liquid biopsies to adapt treatment strategies dynamically.
-
Understanding Resistance Mechanisms:
- Further study of resistance patterns to TKIs and immunotherapies.
- Integration of local therapies to manage resistance-driven recurrences.
Final Thoughts
The role of local therapies, like radiation, remains critical in managing oncogene-driven NSCLC, especially in oligometastatic and locally advanced settings. While combining TKIs, immunotherapy, and radiation is the future, radiation is still a cornerstone of treatment today.
Targeting Beyond the Tumor: Radiation's Evolving Role in Oncogene-Driven Lung Cancer
By RadMedSkiier
Targeting Beyond the Tumor: Radiation's Evolving Role in Oncogene-Driven Lung Cancer
Explore the exciting advancements in targeted therapies for oncogene-driven lung cancer, highlighting novel approaches and trial results that promise to redefine treatment strategies and improve patient outcomes. Discover what the future holds!




