ADRENAL INSUFFICIENCY
Objectives
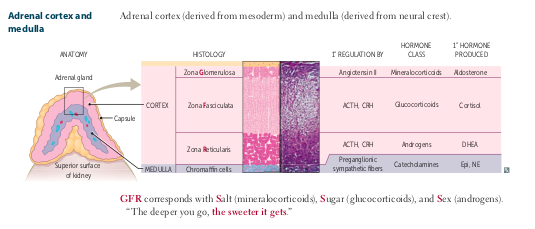
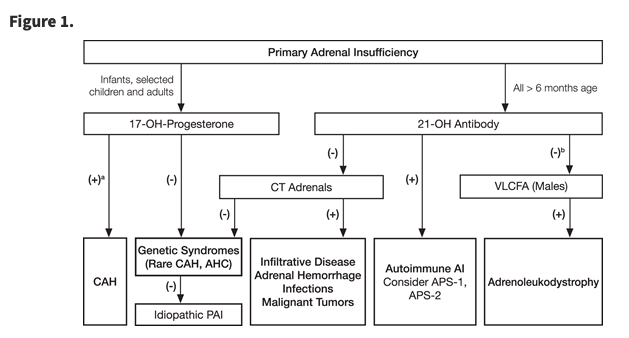
- Primary
- Secondary
- Tertiary
Helpful Resources
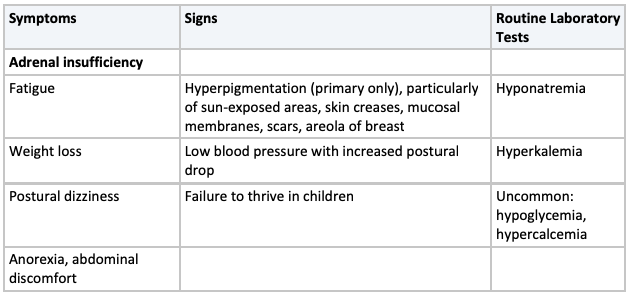
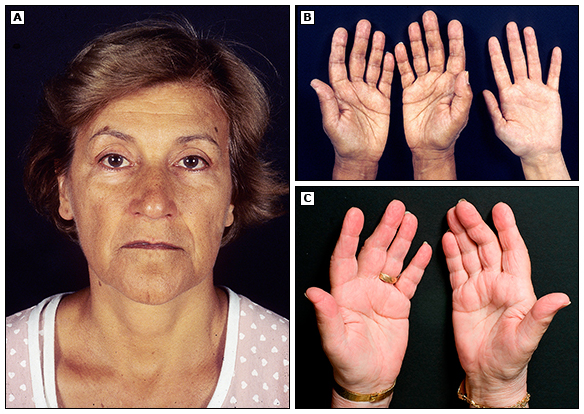
Adrenal Insufficiency
Adrenal Insufficiency
1) AM Screening Studies:
- Cortisol (<140 nmol or < 5 ug/ dL ~= AI)
-ACTH >2xULN
-Renin/Aldosterone
2) Corticotrophin stimulation test (250 ug; 30 or 60 min) *Best test*
-<500 nmol/L , <18 ug/dL =~ AI
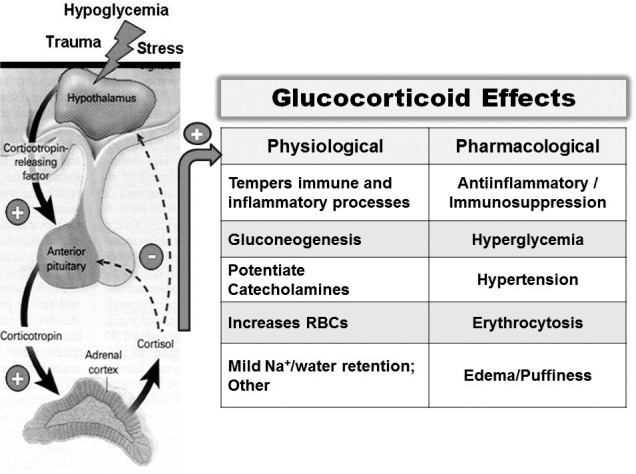
Management of 1' Adrenal Insufficiency
Replace missing hormones:
Glucocorticoid:
- Hydrocortisone 15-25 mg in 2-3 daily doses (biggest dose in the AM, then 2h post lunch) ORPrednisolone (2-5 mg/d)
Monitor:
Body weight
Postural BP
Energy Levels
Cushingoid features
Mineralocorticoid Replacement
- Fludrocortisone (50-100 ug)
- Other: increase dose in hot climates, avoid salt restriction
Monitor: Target: Plasma renin level w/in ULN
Salt cravings
Postural BP
Edema
Lytes
DHEA
(in symptomatic women)
Title Text
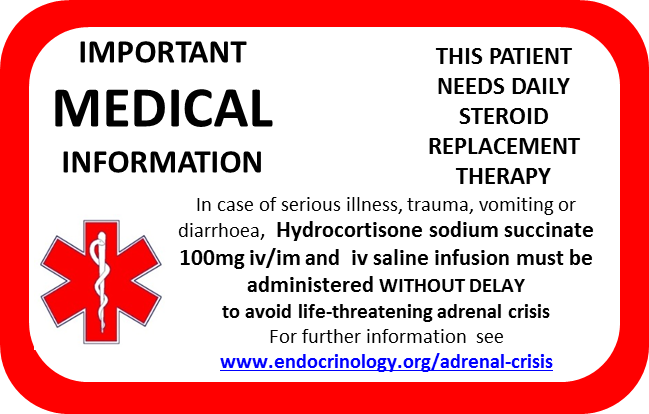
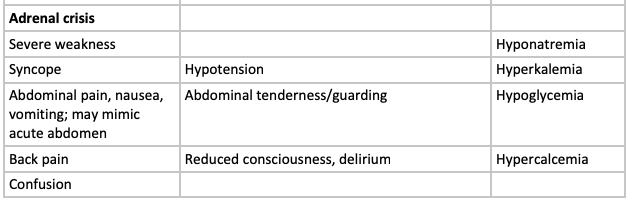
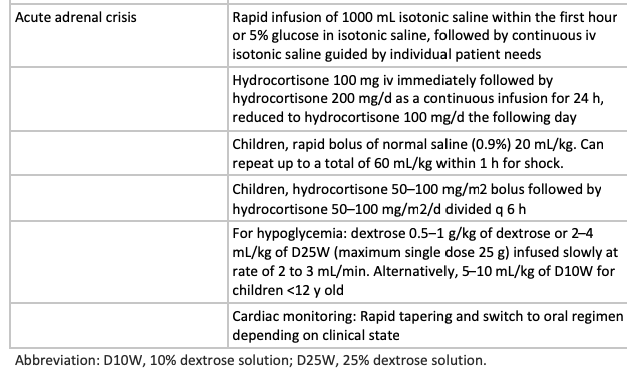
Management of Adrenal Crisis
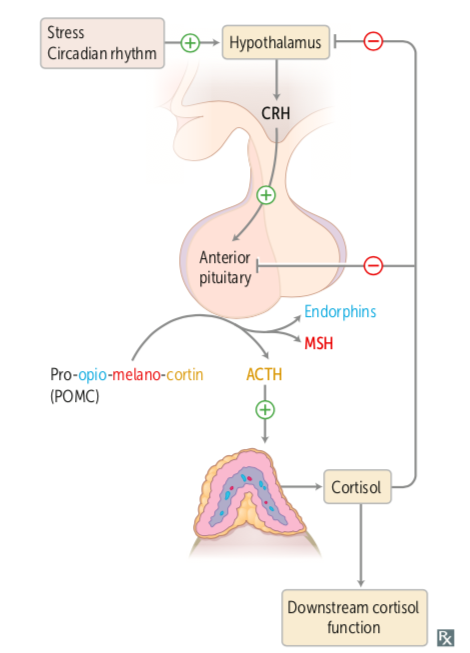
Secondary Adrenal Insufficiency
Limitation of ACTH signalling
Typically occur in concert with other abnormalities
- Loss of POMC gene
- Defect in the enzyme that cleaves ACTH from POMC
- Traumatic brain injury
- Drugs (progestins, opiates)
Tertiary
With-drawl of Cortisol
Common withdrawal
- Removal of ACTH or cortisol secreting tumour
- Suppression of HPA axis by exogenous steroids then discontinuation
- UNLIKELY: Oral steroids <3 wks at physiologic doses (prednisolone 2.5-5 mg/day)
- Is POSSIBLE to occur with any dose/duration
- TYPICALLY:
- 20 mg prednisone x >3 wks
- Anyone with cushingoid features
ADRENAL INSUFFICIENCY
By Seana Nelson



