Review of Mitral Stenosis
Seana Nelson
Cardiology Resident

Mitral Stenosis- Objectives
- Etiologies
- Determining severity
- Use of exercise test
- Management
Etiologies
Rheumatic Heart disease
- Doming of the anterior mitral valve leaflet that is concave towards the atrium in diastole
- Early finding: posterior leaflet tethering leading to immobility
- Commissural fusion
- Chordal shortening and fusion
- Leaflet thickening
- Later in disease course: superimposed calcification
"Hockey stick deformity"
"Dog leg deformity"
Degenerative mitral stenosis
Annular calcification
Associated with hypertension, atherosclerosis
+/- aortic stenosis
Causes few hemodynamic consequences- more likely to cause MR (than MS)
Other differential of mitral stenosis
- Congenital MS
- Inflammatory diseases (SLE)
- Infiltrative disease
- Carcinoid heart
- Drug-induced valve disease
These characteristically have leaflet thickening and restriction. Commissures are rarely fused.
Assessing mitral stenosis
Indices of stenosis severity
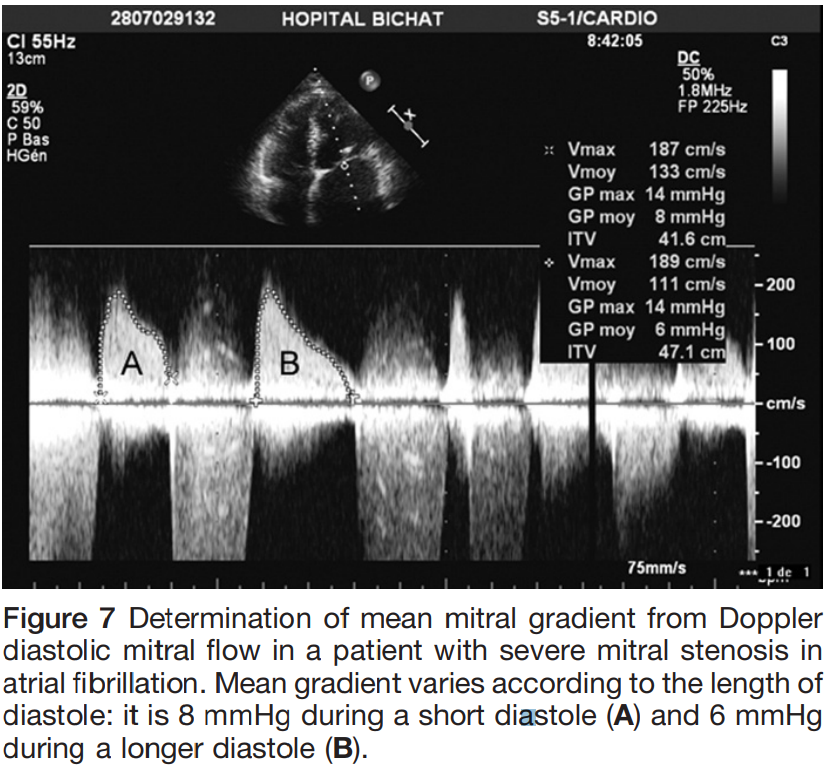
Pressure gradient
- Estimation of the diastolic pressure gradient is derived from the transmitral velocity curve by CWD
- Heart rate should be reported
- For patients with atrial fibrillation, the mean gradient should be calculated as the average of 5 R-R intervals
- Maximal and mean gradients are calculated by tracing Doppler of the diastolic mitral flow
- Dependent on mitral valve area, heart rate, cardiac output and associated MR
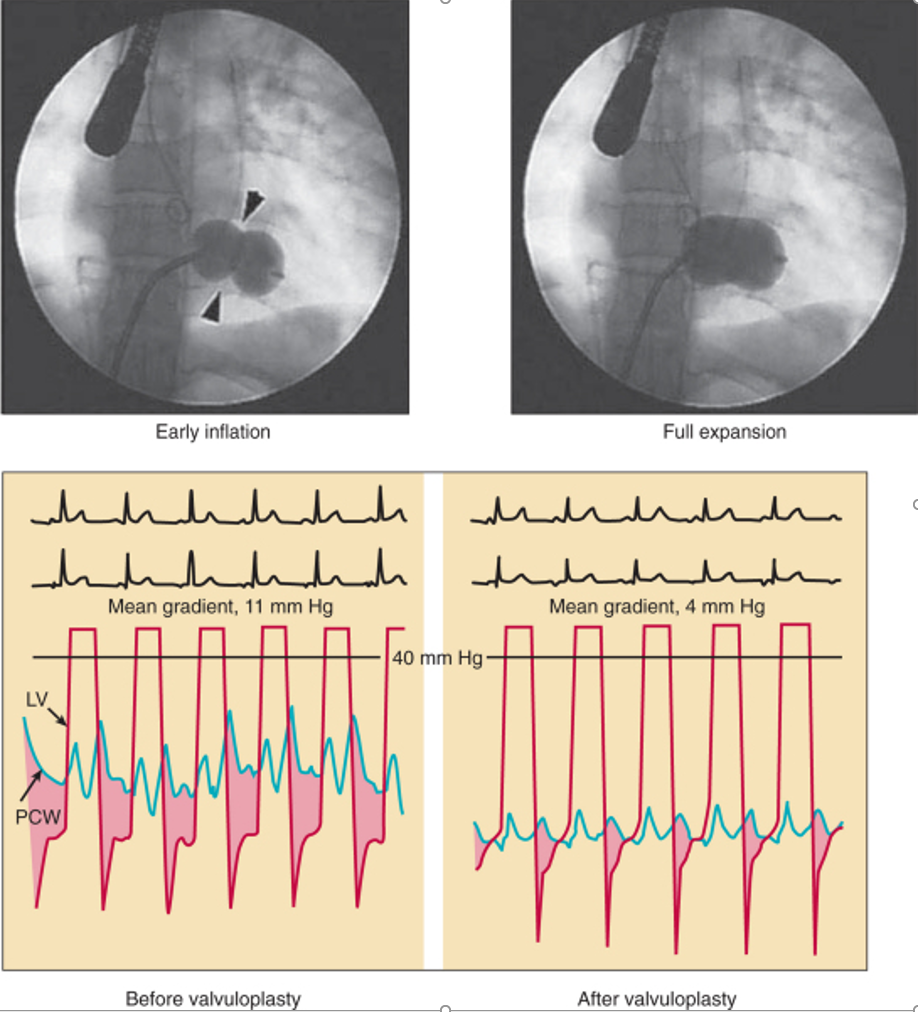
- Has significance following balloon mitral commissurotomy
Pressure gradient
Journal of the American Society of Echocardiography January 2009
MVA Planimetry
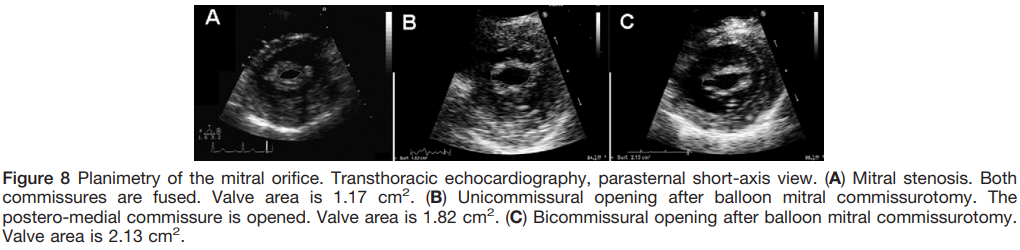
- Direct measurement of the mitral valve orifice at the level of the mitral leaflet tips, including open commissures, from parasternal short-axis view
- It should be perpendicular to the plane of the orifice and have an elliptical shape
- Measured in mid-diastole
- Reference measurement of MVA
Journal of the American Society of Echocardiography January 2009
MVA Planimetry - Challenges
- Dependent on good acoustic window
- Severe valve calcification affects the accurate delineation of the leaflet tips: seen especially in degenerative mitral stenosis.
- Determining the correct angle can be challenging
- 3D-guided biplane imaging can improve this

- Technically challenging
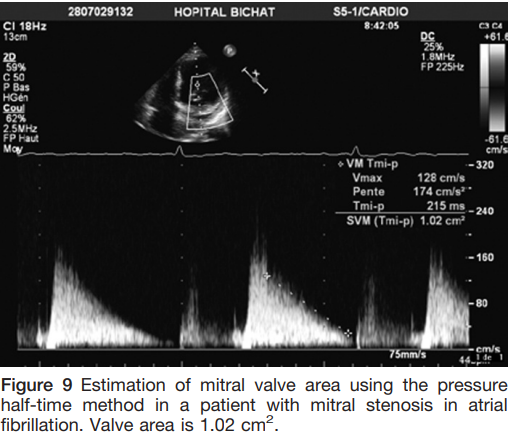
MVA Pressure half-time
- Time interval (in ms) between maximal mitral gradient in early diastole and the time-point when the gradient is half the maximal initial value
- The decline of the velocity of diastolic transmitral blood flow = inversely proportional to valve area
- MVA = 220 ⁄ T1⁄2
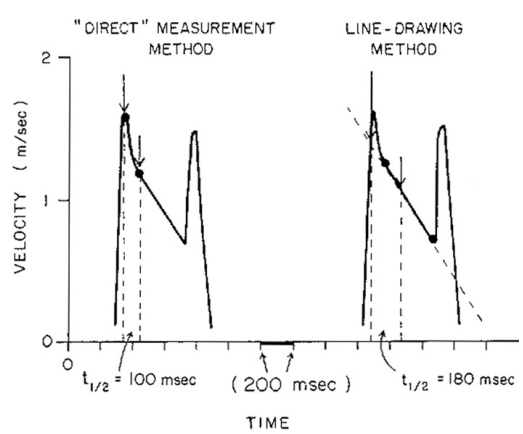
- Performed by tracing the deceleration slope of the E-wave on Doppler spectral display
- Avoid use in degenerative MS
Journal of the American Society of Echocardiography January 2009
Short T1/2
- Low left atrial compliance
- Atrial septal defect
- Severe AR
- Decreased LV compliance
Long T1/2
- Impaired LV relaxation
- Increased LV pressure
MVA Pressure half-time - challenges
- Challenges with bimodal slopes: deceleration slope should be taken from mid-diastole
- If the deceleration shape is concave then it should not be traced
- In atrial fibrillation avoid tracing short diastoles
Journal of the American Society of Echocardiography January 2009
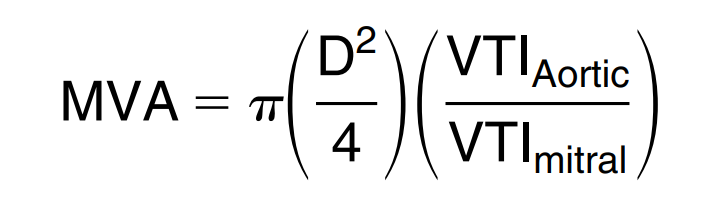
Continuity equation
- Accuracy and reproducibility is limited by the number of calculations, increasing the impact of errors of measurements
- Can not be used in:
- AF
- MR
- AR
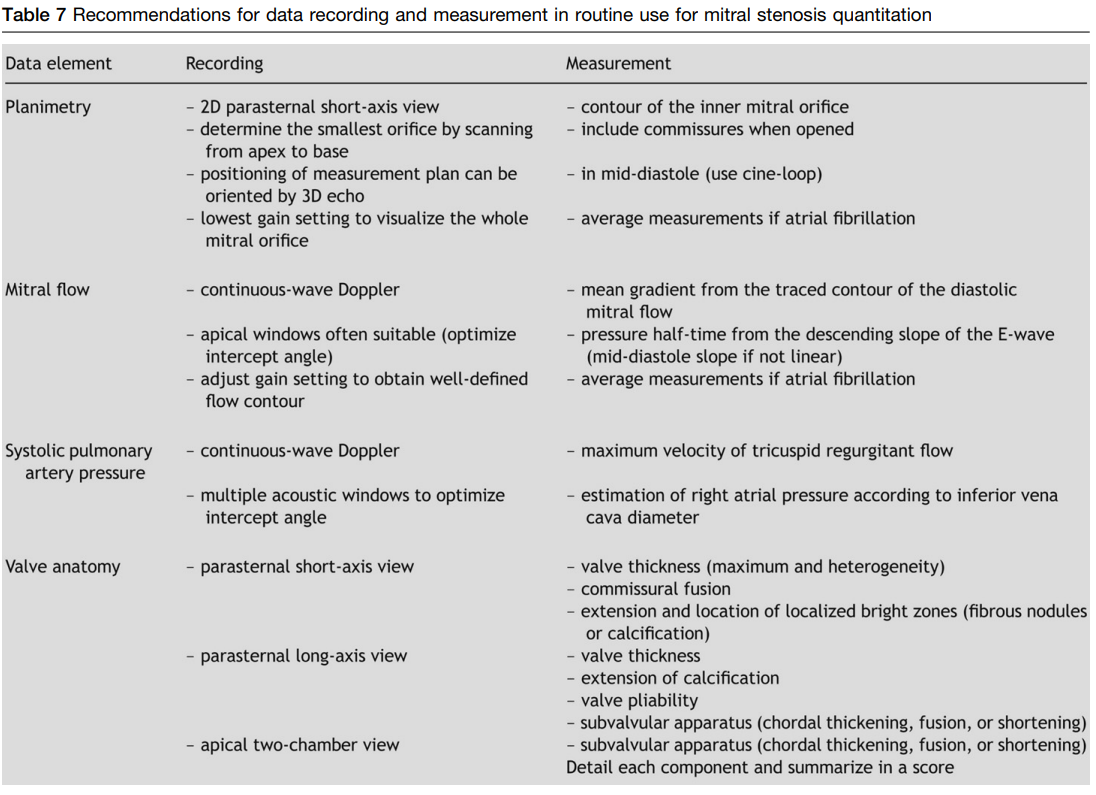
Valve anatomy -parasternal short-axis
- Commissural fusion can be assessed at the same level as planimetry
- Difficult to visualize with severe anatomy
- Best viewed with 3D echocardiography
- Complete fusion = severe MS
- Lack of commissural fusion does not exclude significant MS
- Comment on homogeneity of valve area
Valve anatomy -parasternal long axis view
- Leaflet thickening and mobility
- Chordal shortening and thickening
Journal of the American Society of Echocardiography January 2009
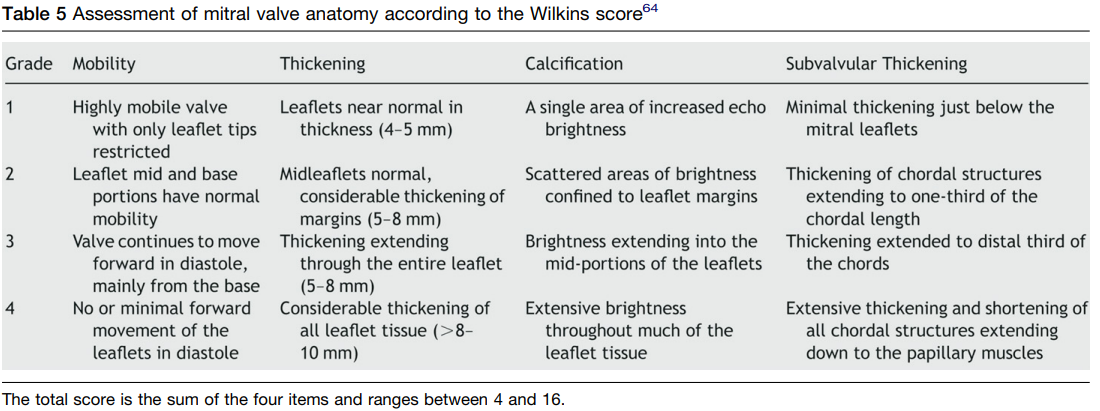
Wilkins score 11
Journal of the American Society of Echocardiography January 2009
Associated anatomy
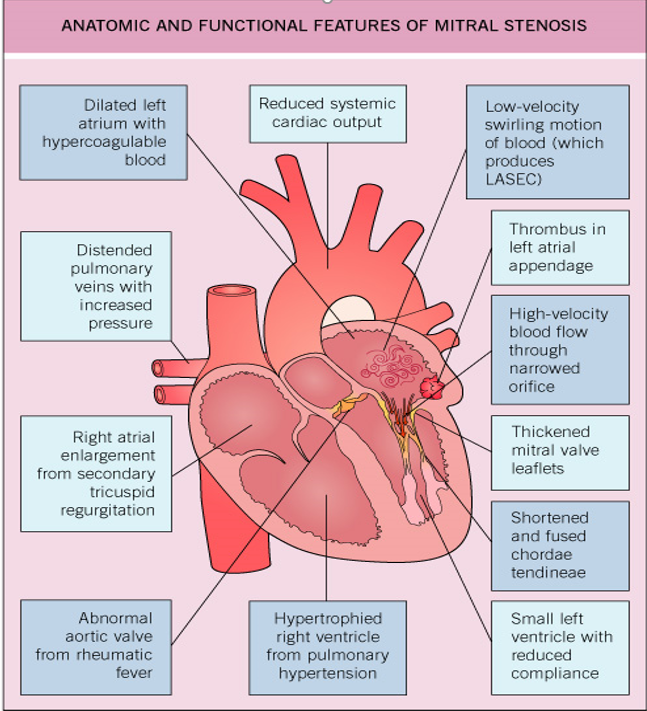
2004 Elsevier Lt- Cardiology 2E, edited by Crawford, DiMarco and Paulus. All rights reserved.
Associated anatomy
- Mitral regurgitation is defined by quantitative and semi-quantitative methods
- Aortic stenosis: severity may be underestimated because of reduced stroke volume
- Aortic regurgitation: severe AR - T(1/2) for MVA is not valid
- Tricuspid valve - involvement of rheumatic process
Stress Echo
Stress Echo
- Useful in patients whose symptoms are not congruent with the severity of MS
- Semi-supine exercise echocardiography preferred: allows monitoring of gradient and pulmonary pressures at each workload
- Dobutamine stress echo can in be used
Rest (HR 64 bpm)
Peak (HR 134 bpm)
Grading Mitral Stenosis
Journal of the American Society of Echocardiography January 2009
Grading of mitral stenosis
- Mean gradient
- Valve area by planimetry and T1/2
- If discrepancy: planimetry is preferred
- Associated MR - particularly when moderate-severe
- Consequences of MS - LA size, systolic pulmonary pressures
- Anatomy of the valve: impairment of leaflets, subvalvular apparatus, degree of commissural fussion
Interventions for Mitral stenosis
Stages of mitral stenosis
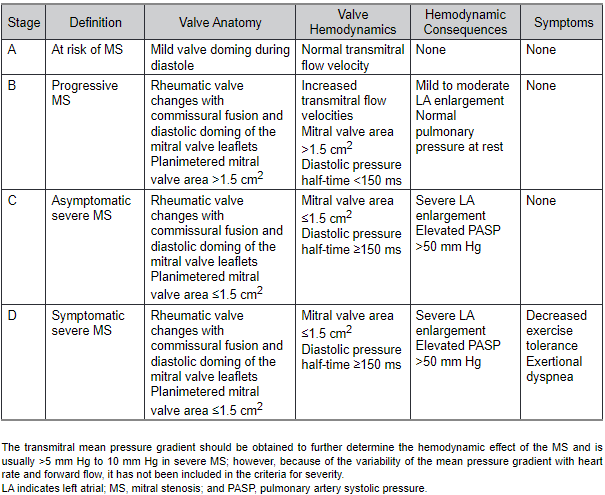
2020 ACC/AHA Guideline for the Management of Valvular Heart Disease
Intervention for Rheumatic MS
Kumar, et al. 2020, Circulation 142(20), pp.e337- e357
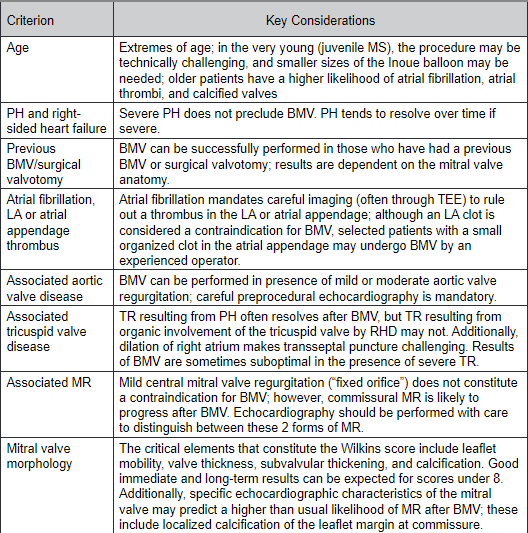
Intervention for Rheumatic MS

2020 ACC/AHA Guideline for the Management of Valvular Heart Disease
Intervention for Rheumatic MS
Intervention for Degenerative MS
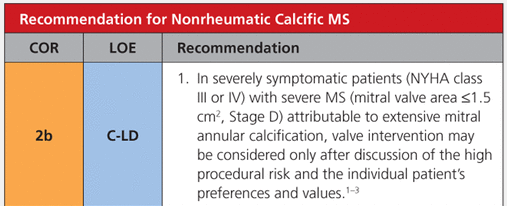
2020 ACC/AHA Guideline for the Management of Valvular Heart Disease
- Because calcification involves the annulus and base without the commissures there is no role for PMBC
- Patients with stenosis from MAC have high surgical risk due to multiple comorbidities
Summary
- Determining mitral gradient
- Determining mitral valve area by planimetry, T1/2
- Describing mitral valve anatomy
- Use of exercise testing
- Interventions for MS
Please evaluate the presentation
Mitral Stenosis
By Seana Nelson



