Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
Atul Jaidka
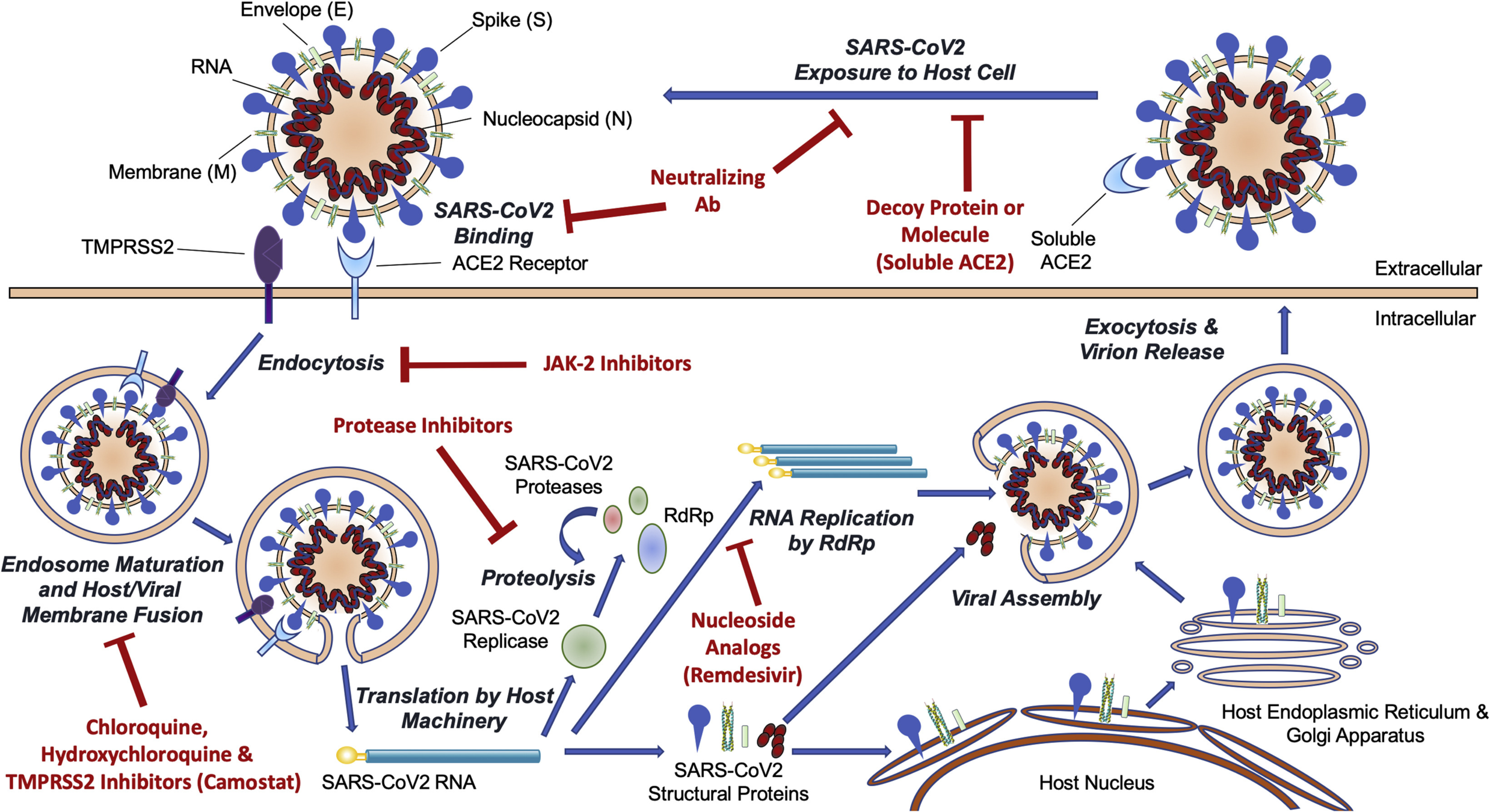
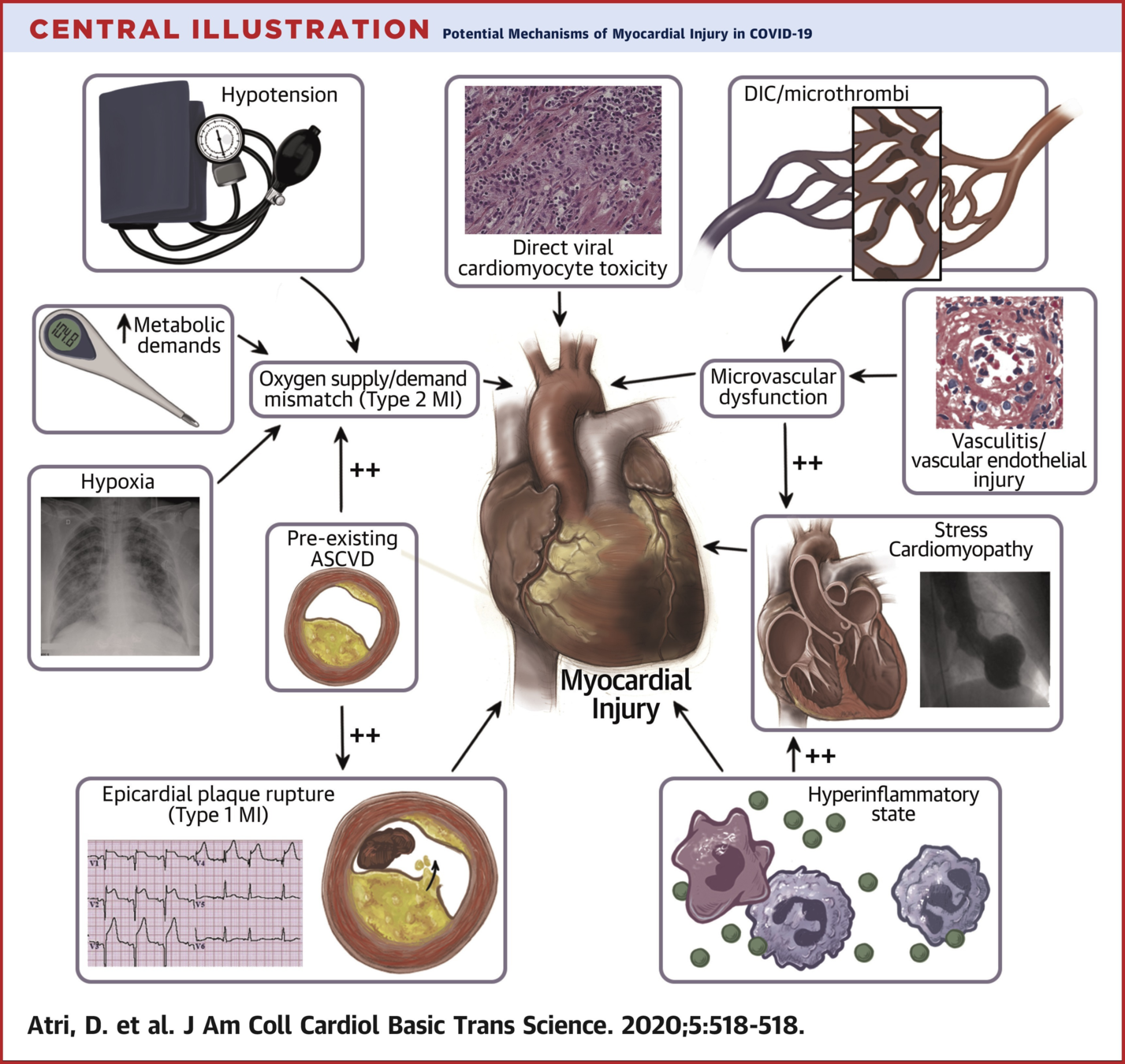
Atri D, Siddiqi HK, Lang JP, Nauffal V, Morrow DA, Bohula EA. COVID-19 for the Cardiologist: Basic Virology, Epidemiology, Cardiac Manifestations, and Potential Therapeutic Strategies. JACC Basic Transl Sci. 2020; 5(5):518-536. [PDF]
UTD
UTD
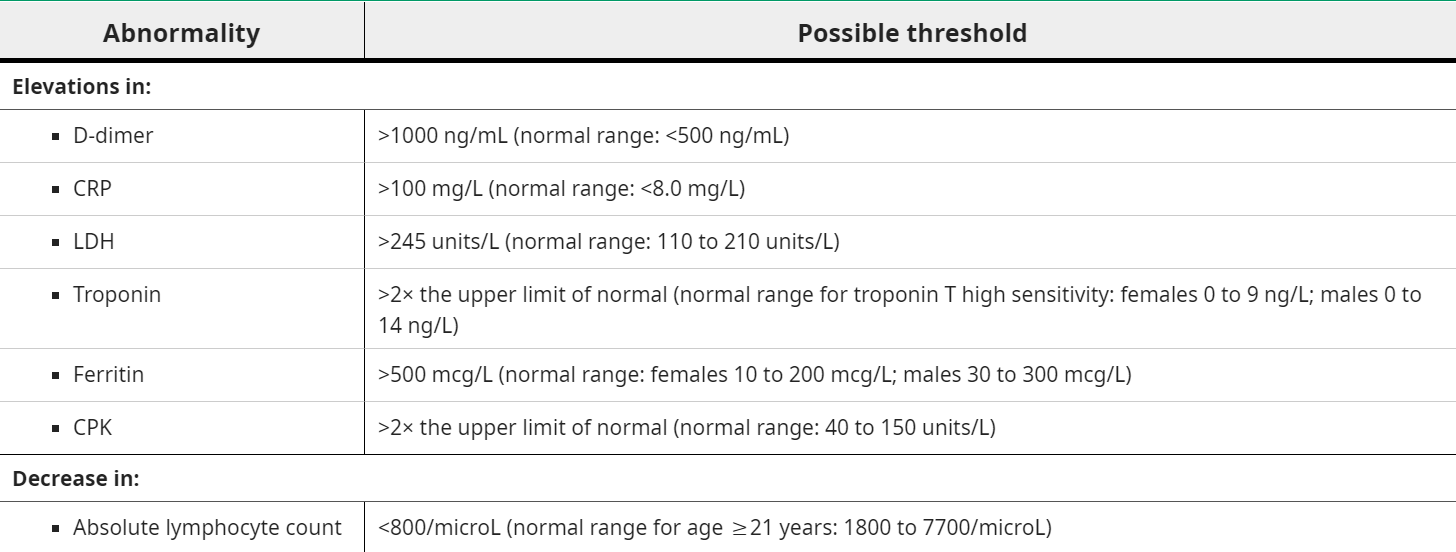
Recommended in all patients:
Recommended in patients with new HF, ECG changes, or cardiac arrhythmias. Important considerations:
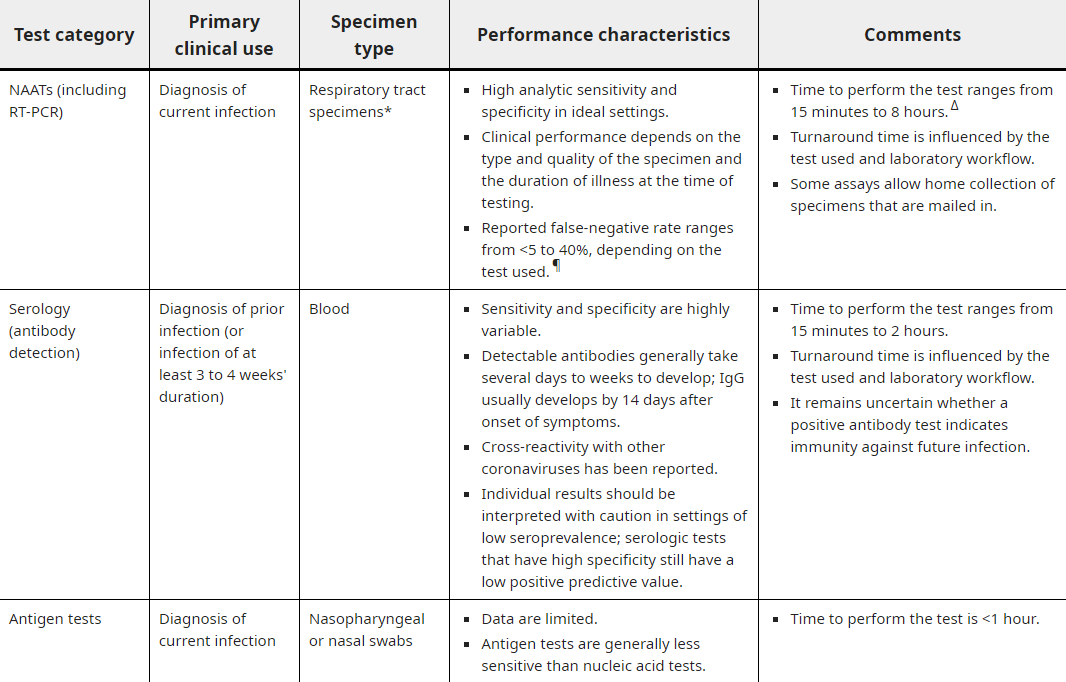
All patients:
Cause unknown but proposed mechanisms:
Unknown if ACE2 signaling pathway has a role in COVID-19 cardiac injury
By Atul Jaidka



