Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
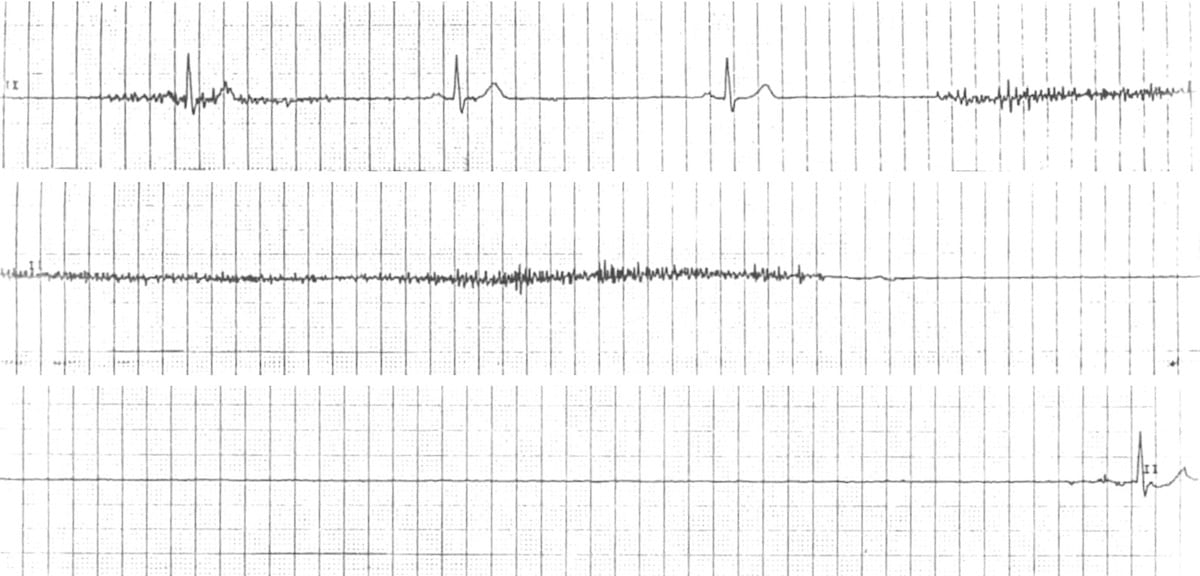
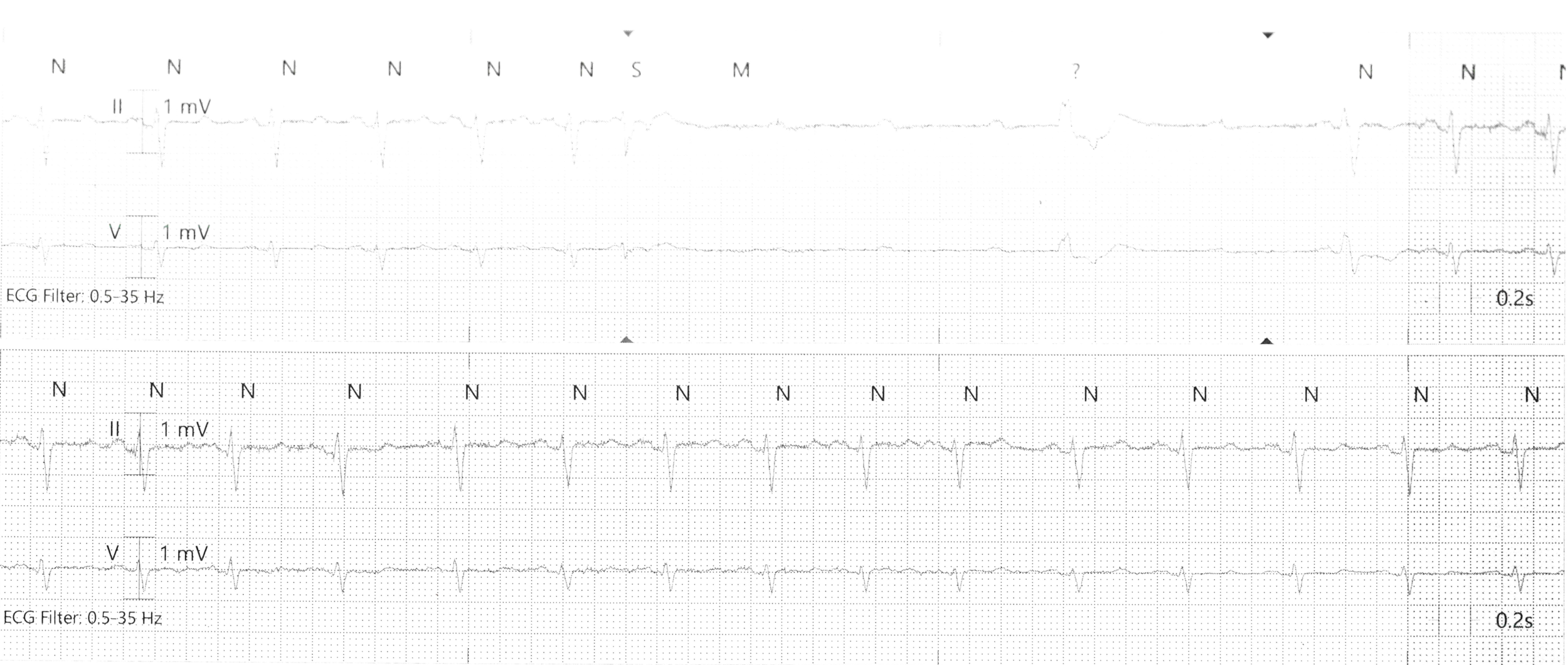
Note: no time stipulation for pauses
Temporary Transvenous?
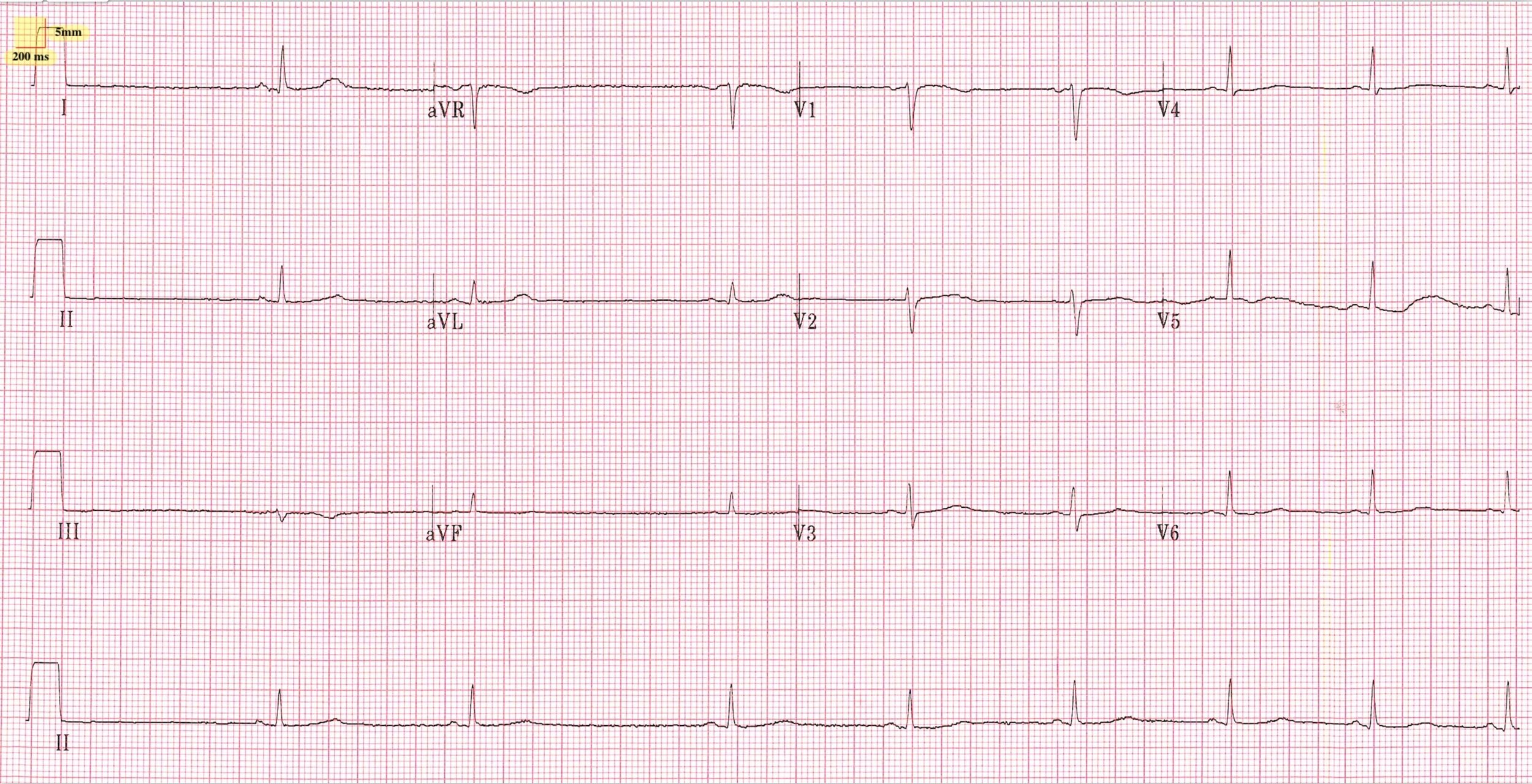
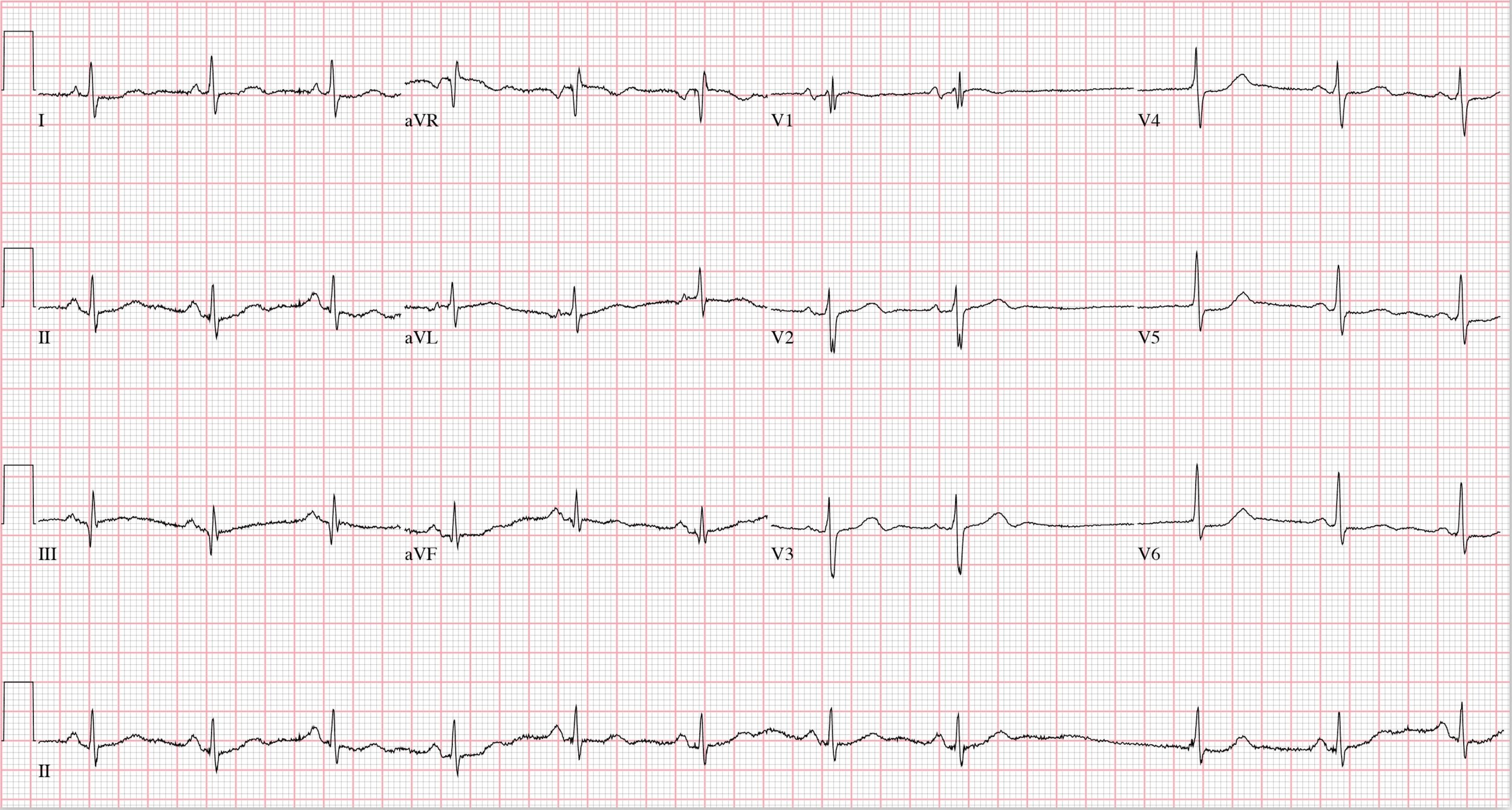
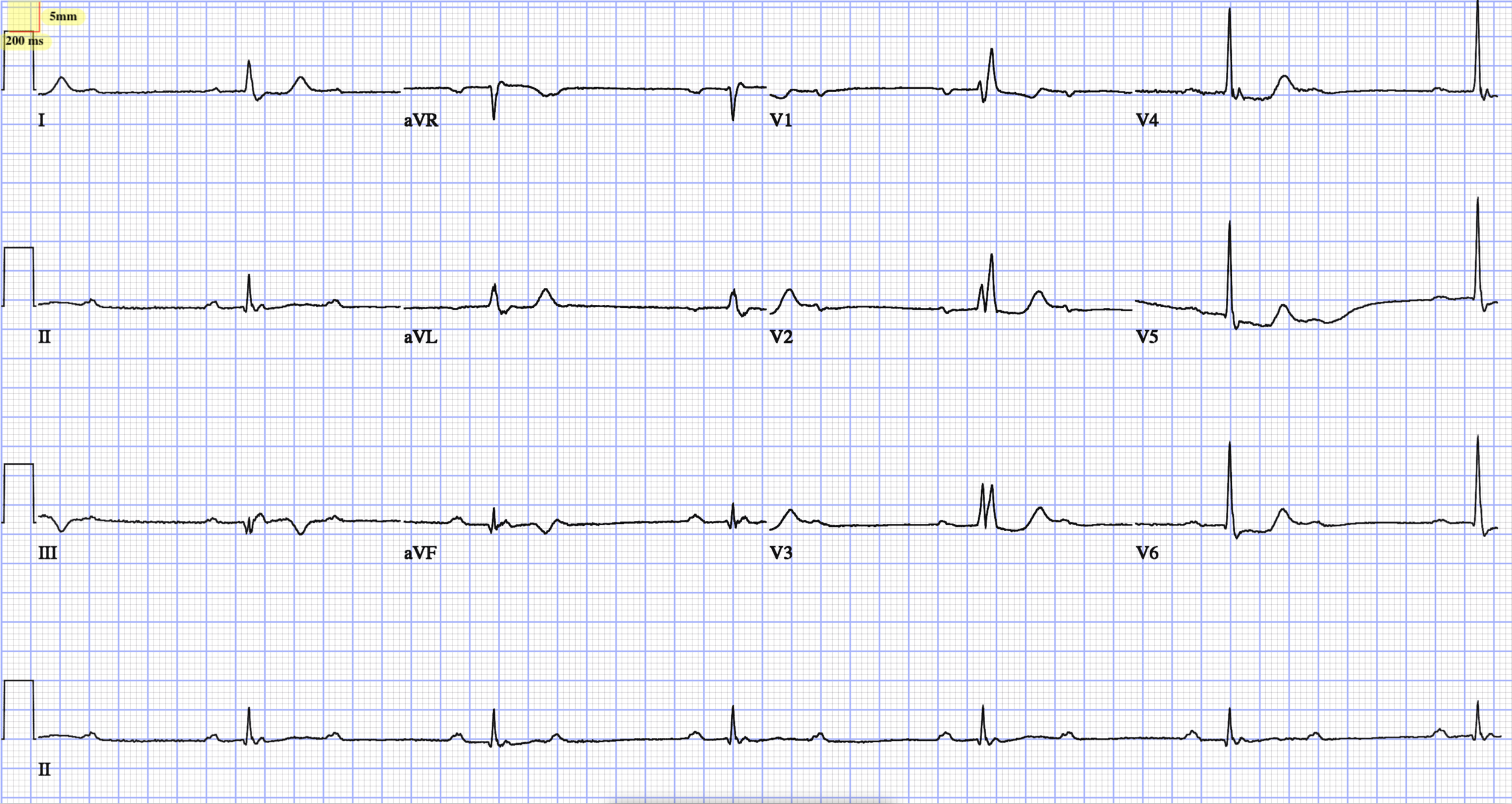
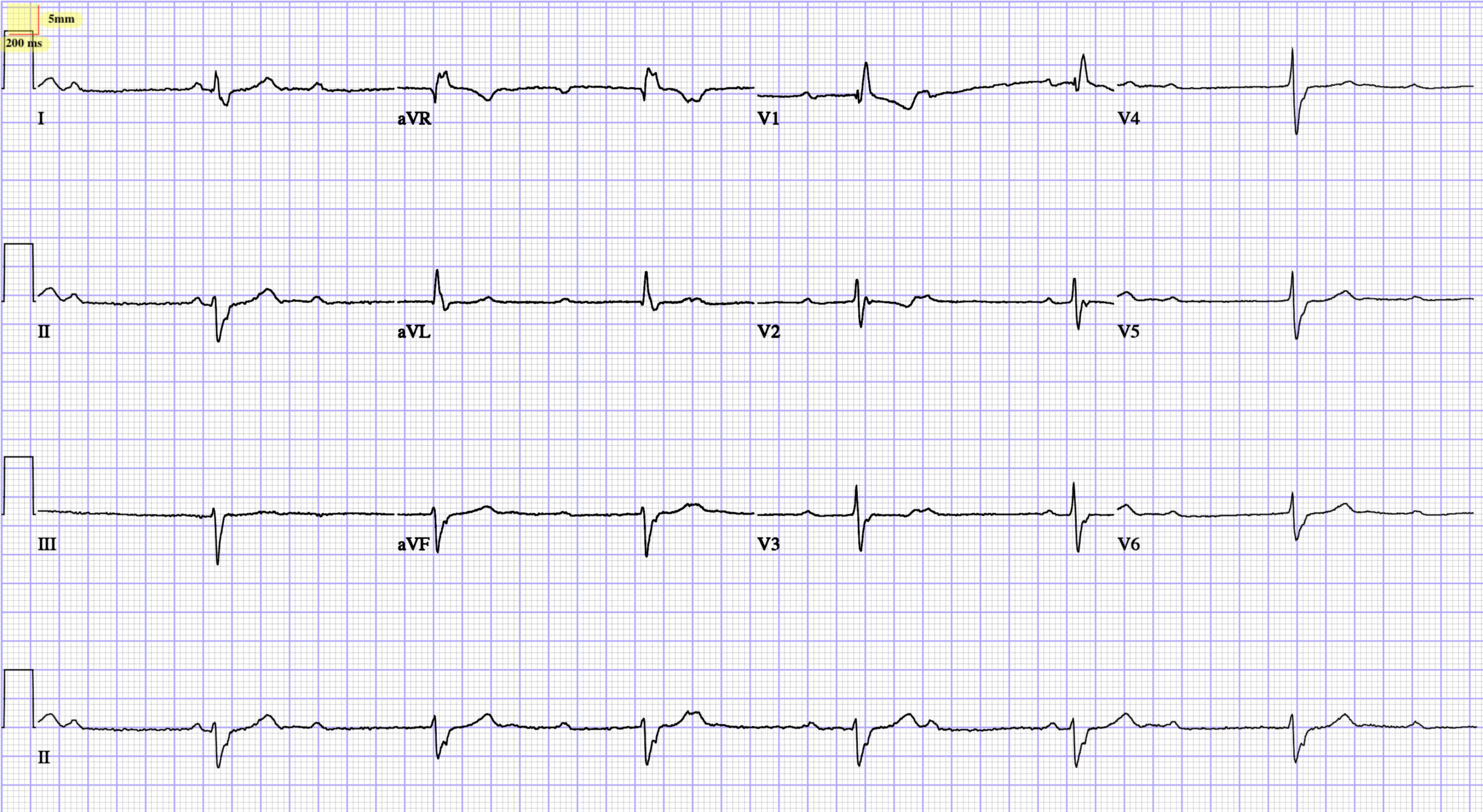
Sinus bradycardia with sinus arrhythmia with 1st degree A-V block with occasional with 2nd degree A-V block (Mobitz I) , 2:1 av-block , Premature ventricular complexes with ventricular escape complexes
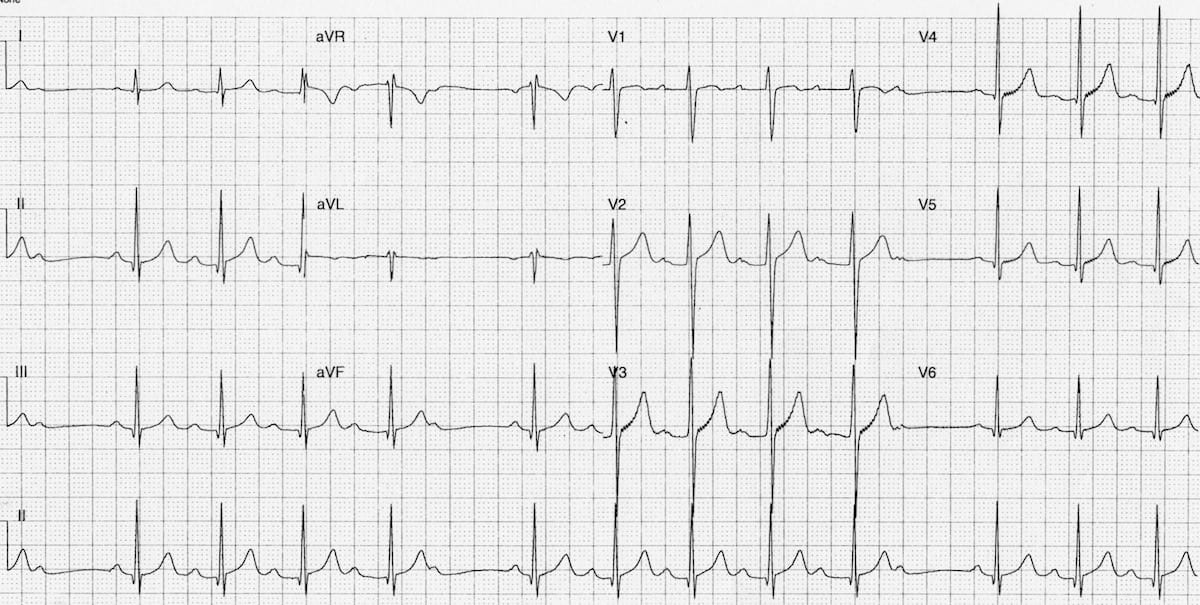
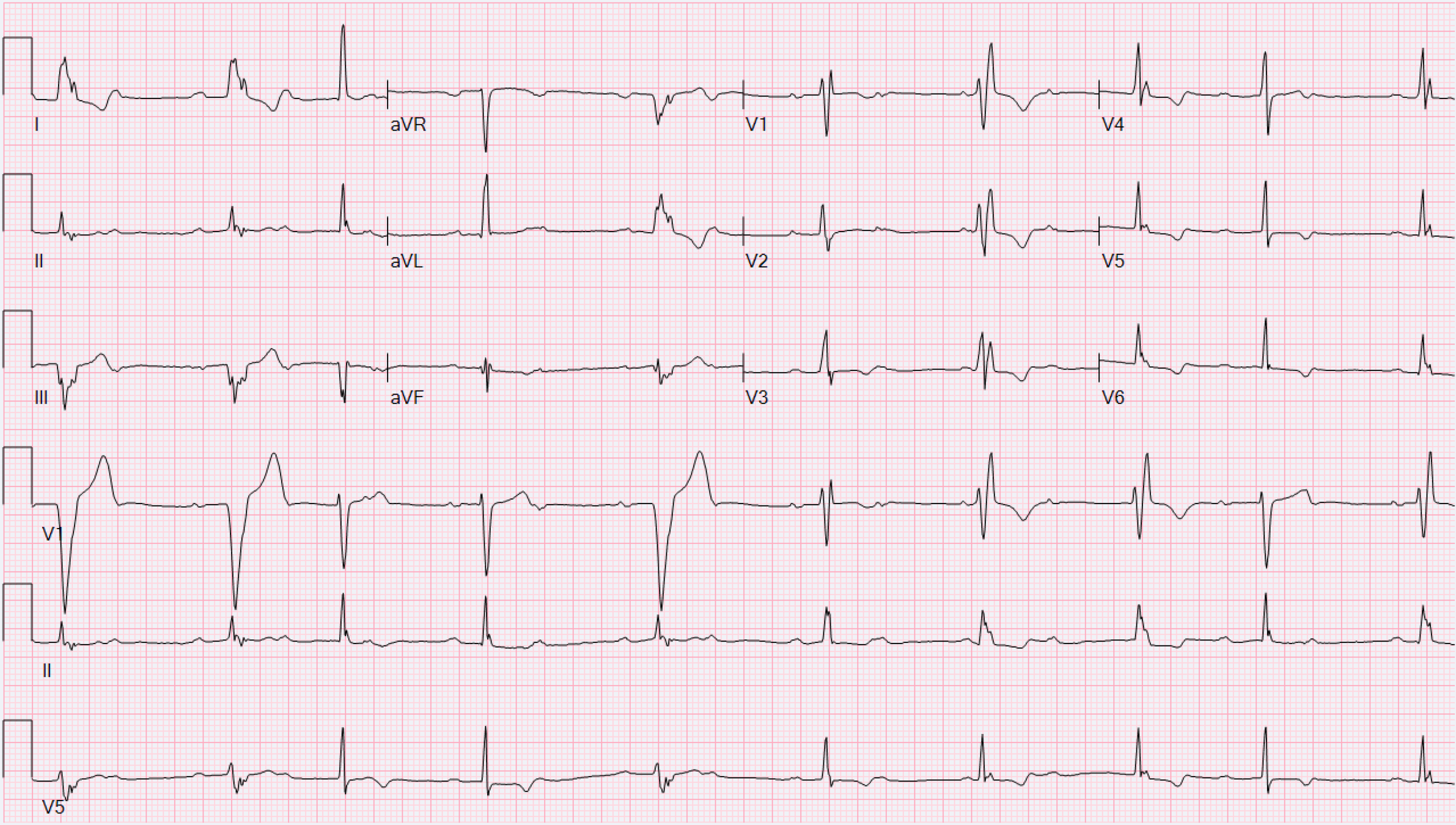
Intermittent Left bundle branch block and Right bundle branch block complexes
By Atul Jaidka



