Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
ID: 31M admitted for SOB
PMH: Remote IVDU, Endocarditis 2011 of AV/MV complicated by severe AR resulting in Prosaic Bioprosthetic Valve inserted, residual significant MR
MEDS: Carvedilol, Candarsartan, Lasix
Social: No more IVDU
HPI: 2 week history of SOB, cough, subjective fevers/chills, NYHA Class 3-4.
Exam: VS stable, no oxygen requirements, afebrile, mild clinical hypovolemia
Previous Echo:
Plan:
Previous
Blood cultures: Negative (remained afebrile)
CT Abdo: Splenic infarct
CT Head: Frontal subarachnoid hemorrhage with associated mycotic aneurysm
Presumed paravalvular abscess adjacent to the bioprosthetic aortic root including communication with the subvalvular LVOT. Multiple areas of low attenuation within the cavity, the right ventricle and the mitral valve likely represent vegetations versus thrombus.
Moderate size mobile filling defect at the right ventricular apex, not seen on non-contrast images,
suspicious for chordal based vegetation or thrombus.
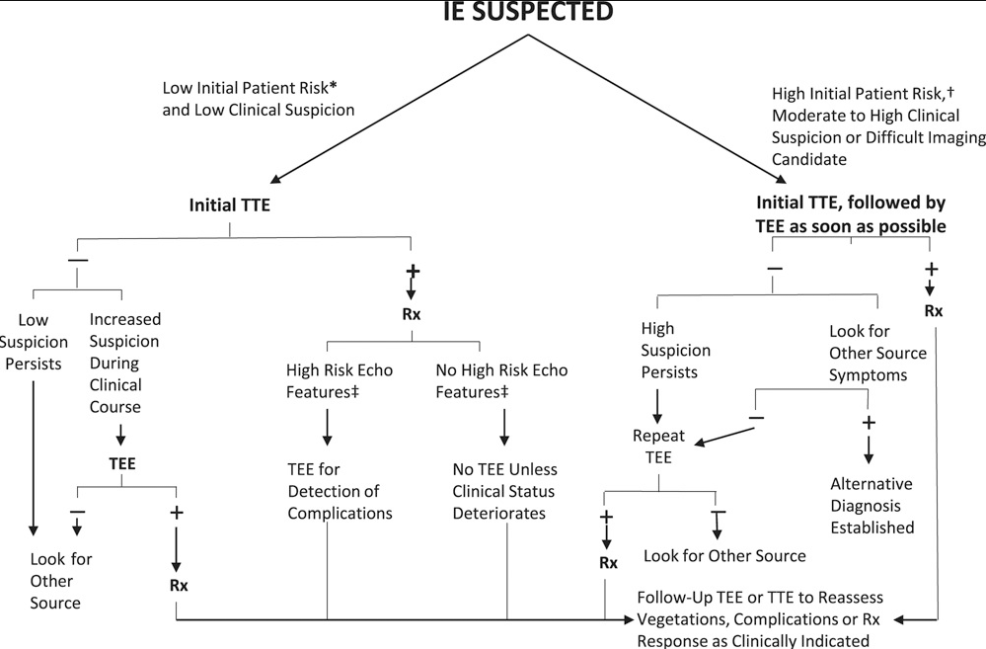
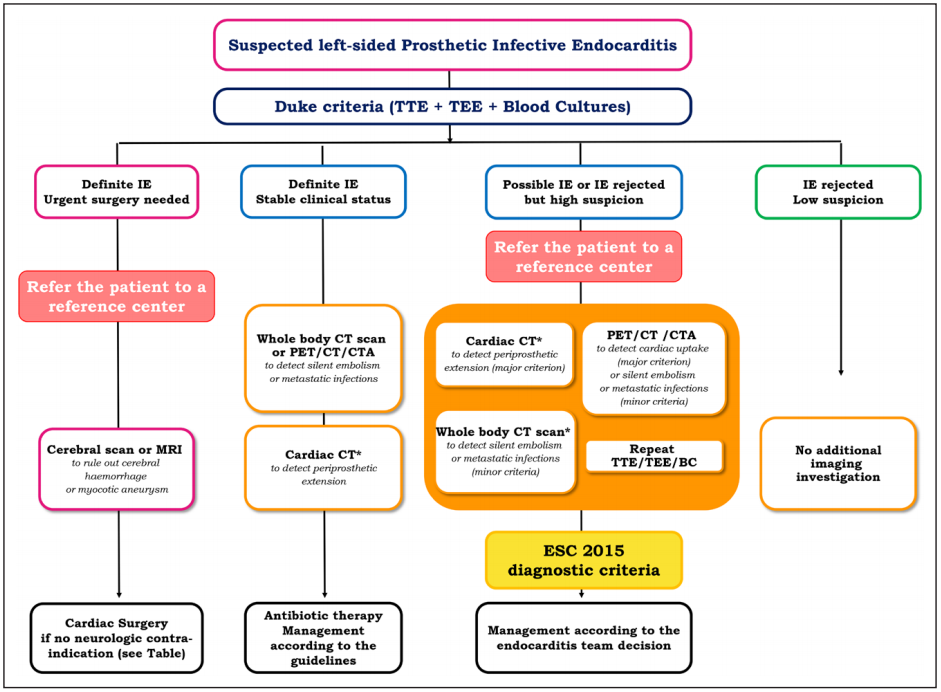
AHA
Erba PA, Pizzi MN, Roque A, et al. Multimodality Imaging in Infective Endocarditis: An Imaging Team Within the Endocarditis Team. Circulation. 2019; 140(21):1753-1765.
Management Challenge
OR:
Follow-up:
By Atul Jaidka
Echo Rounds - Jan 22



