

Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
Uptodate
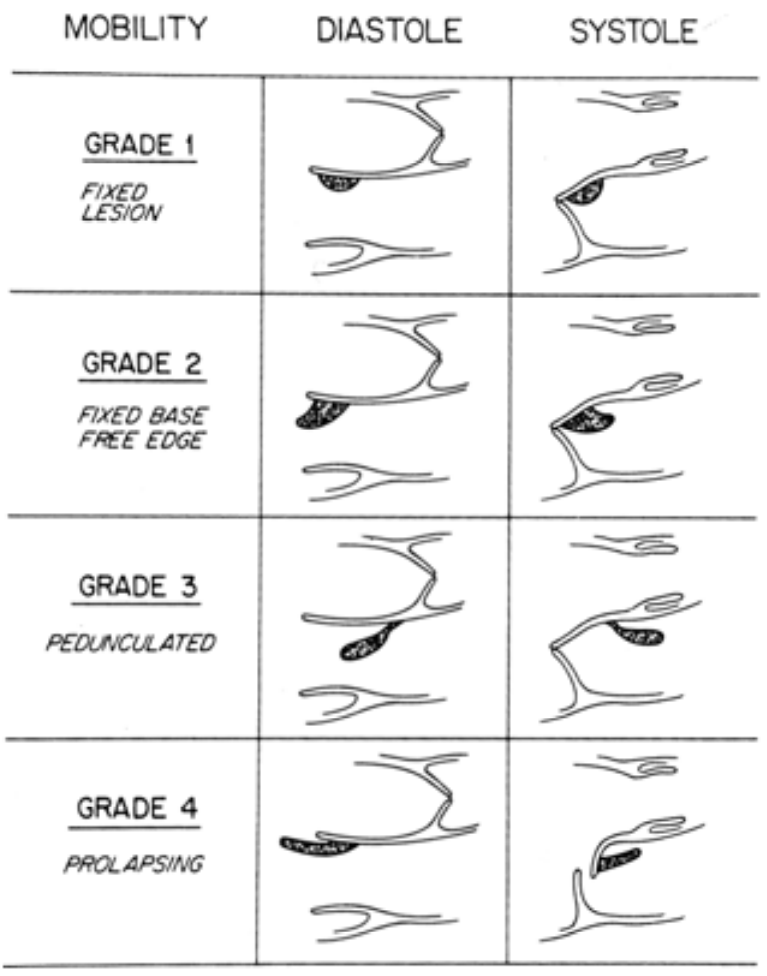
AHA: High risk: large/mobile vege, perivalvular extension, mod/sev regurg, new LV dysfunction
Uptodate
Note: new or worsening murmur not sufficient
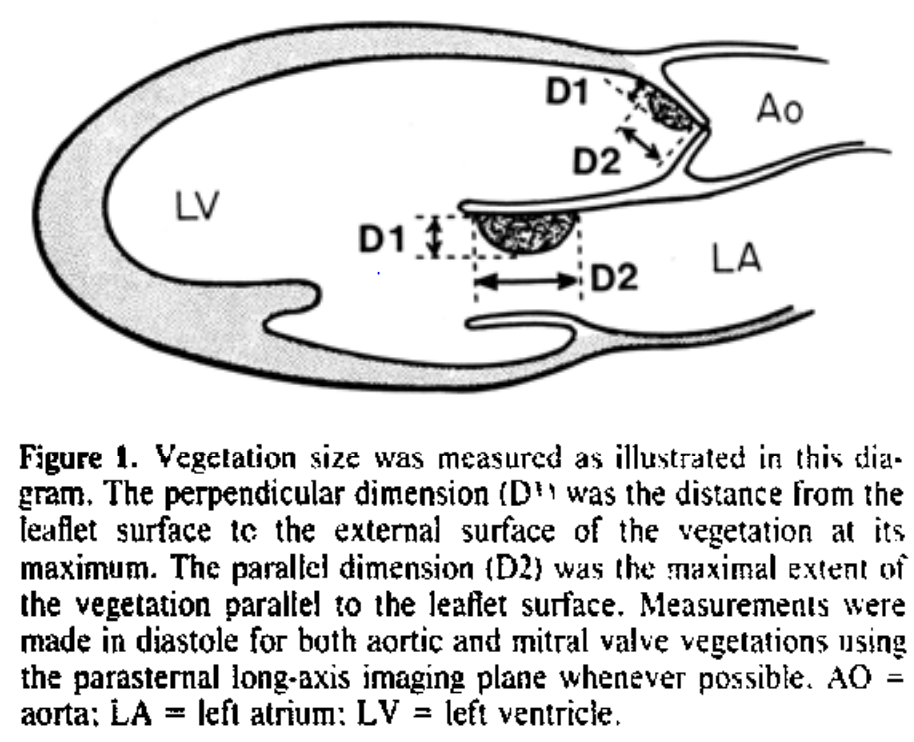
Two largest orthogonal dimensions
Sanfillpo et al. Echocardiographic assessment of patients with infectious endocarditis: prediction of risk for complications.
Sanfillpo et al. Echocardiographic assessment of patients with infectious endocarditis: prediction of risk for complications.
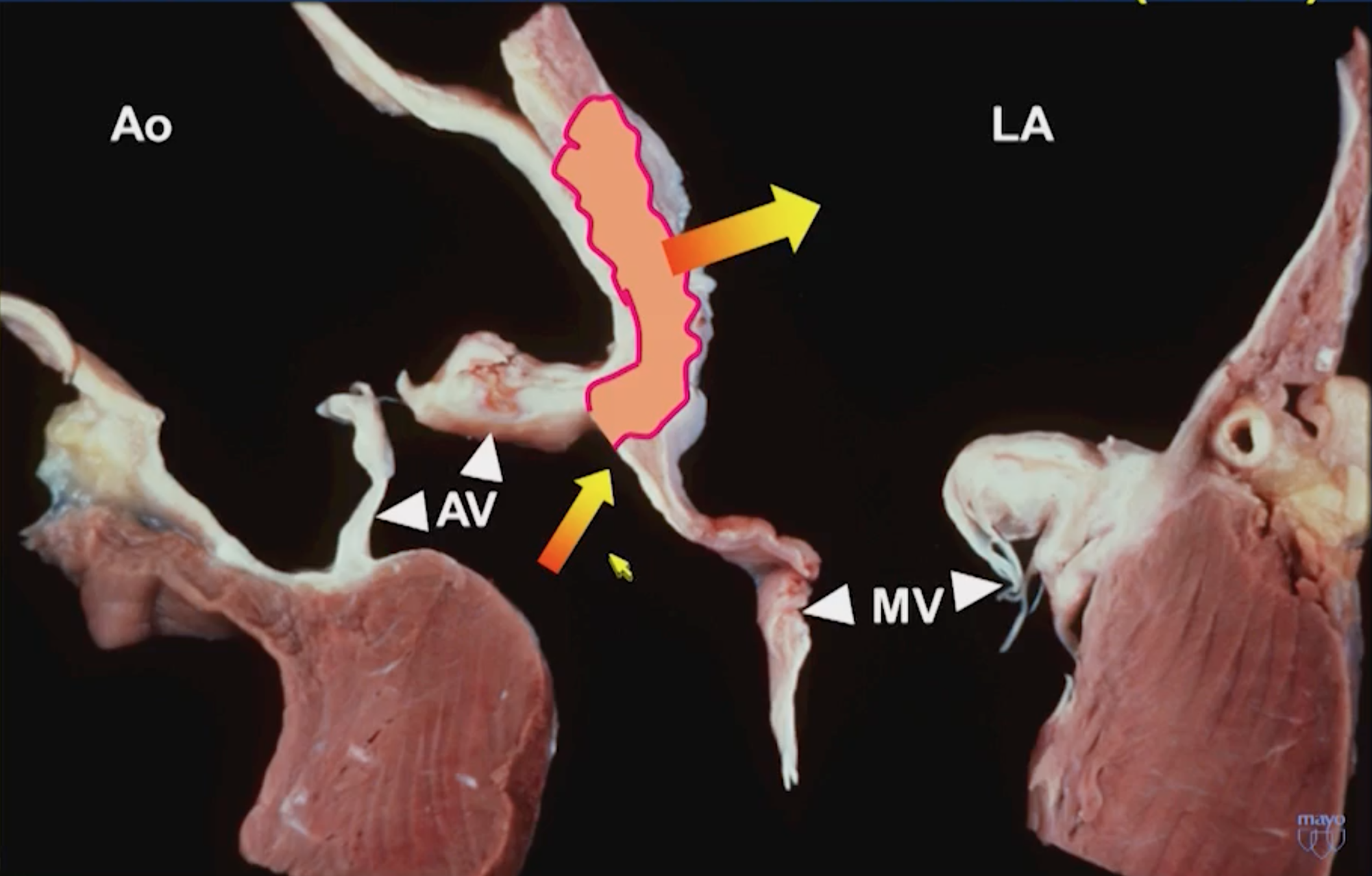
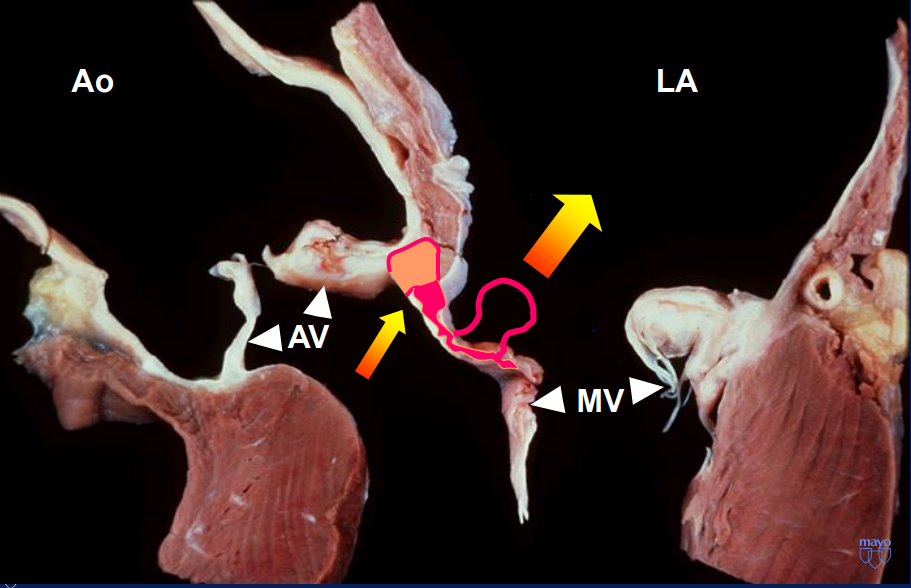
Fibrous region of the heart that connects the anterior mitral leaflet to the posterior aortic root and communicates with the left ventricular outflow tract
1. Urgent re-do sternotomy.
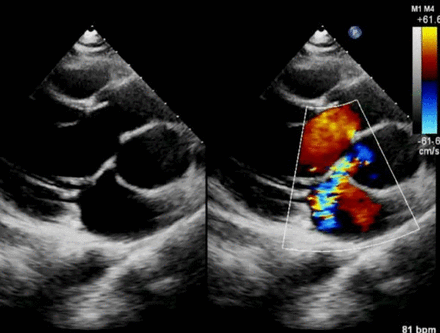
2. Aortic valve explantation and extensive debridement of aortic root and fibrous trigones.
3. Aortic root replacement (26 mm LifeNet aortic homograft).
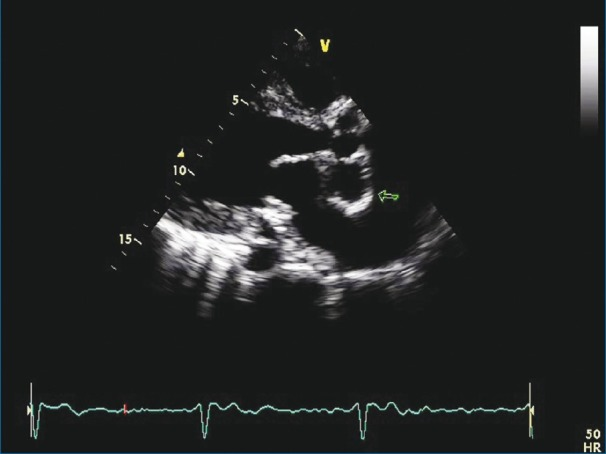
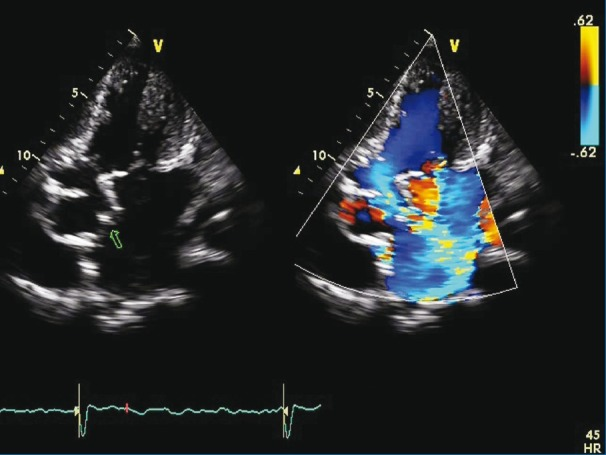
4. Palliative, complex mitral repair (A2 triangular resection, debridement of posterior medial commissure, A1 perforation closure and 34 mm Cosgrove band annuloplasty).
5. Repair of atrioventricular groove, reconstruction of fibrous trigones.
6. Patent foramen ovale closure.
7. Left common femoral arterial line.
By Atul Jaidka
Echo Rounds - Jan 22



