
Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
Journal Club Nov 4, 2021 | Atul Jaidka
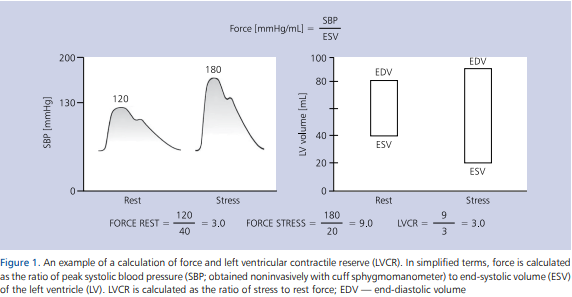
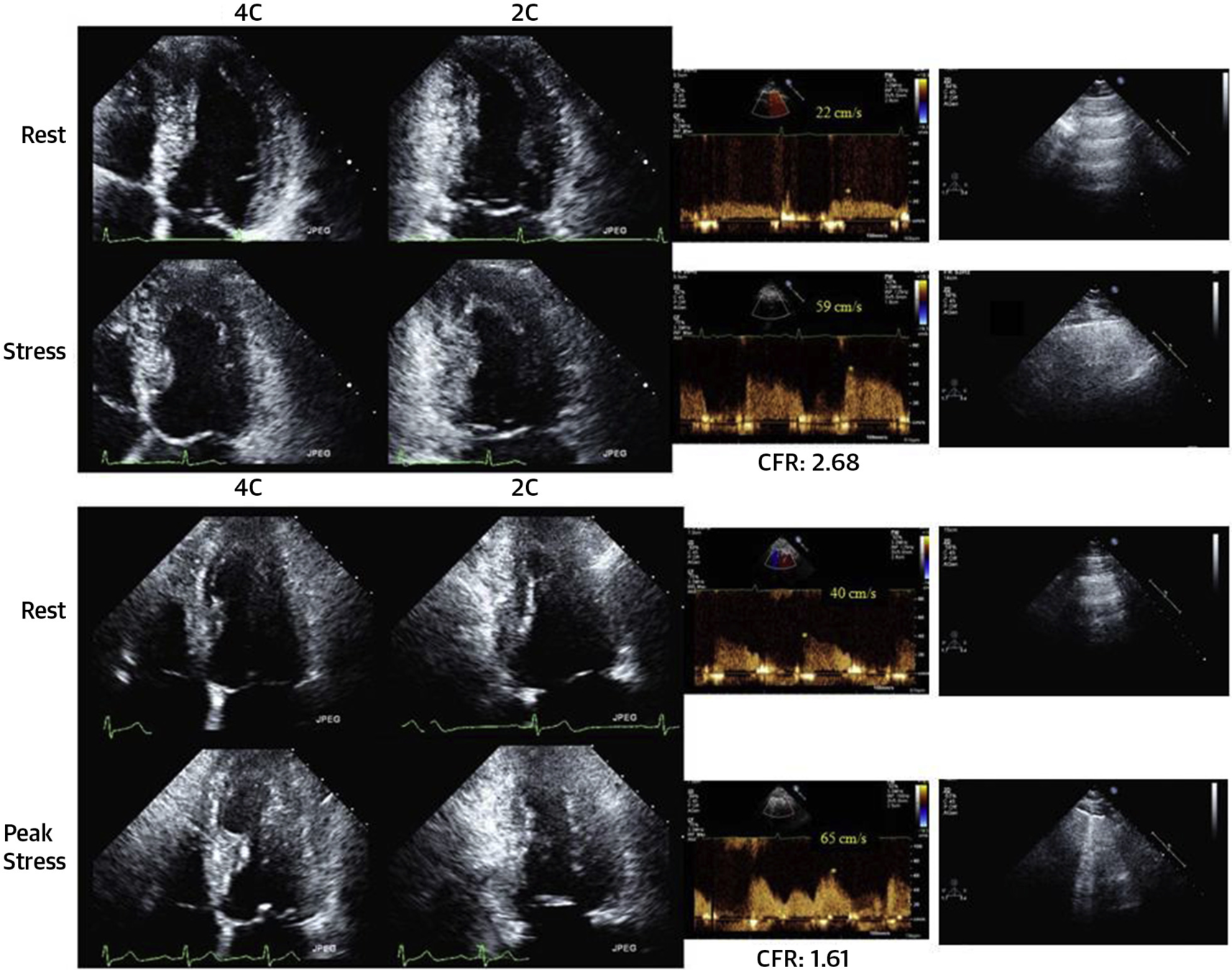
Rest
Post Exercise
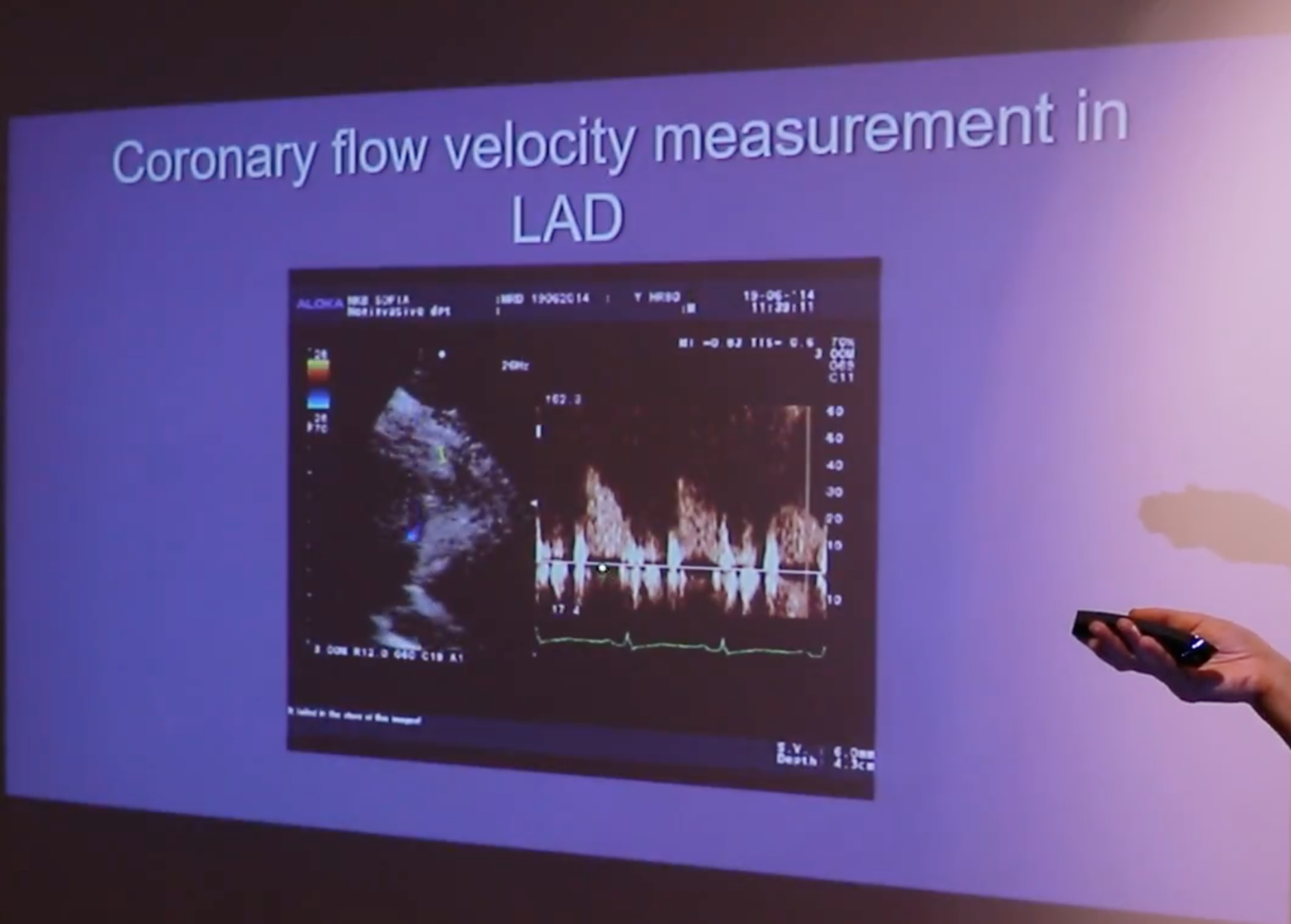
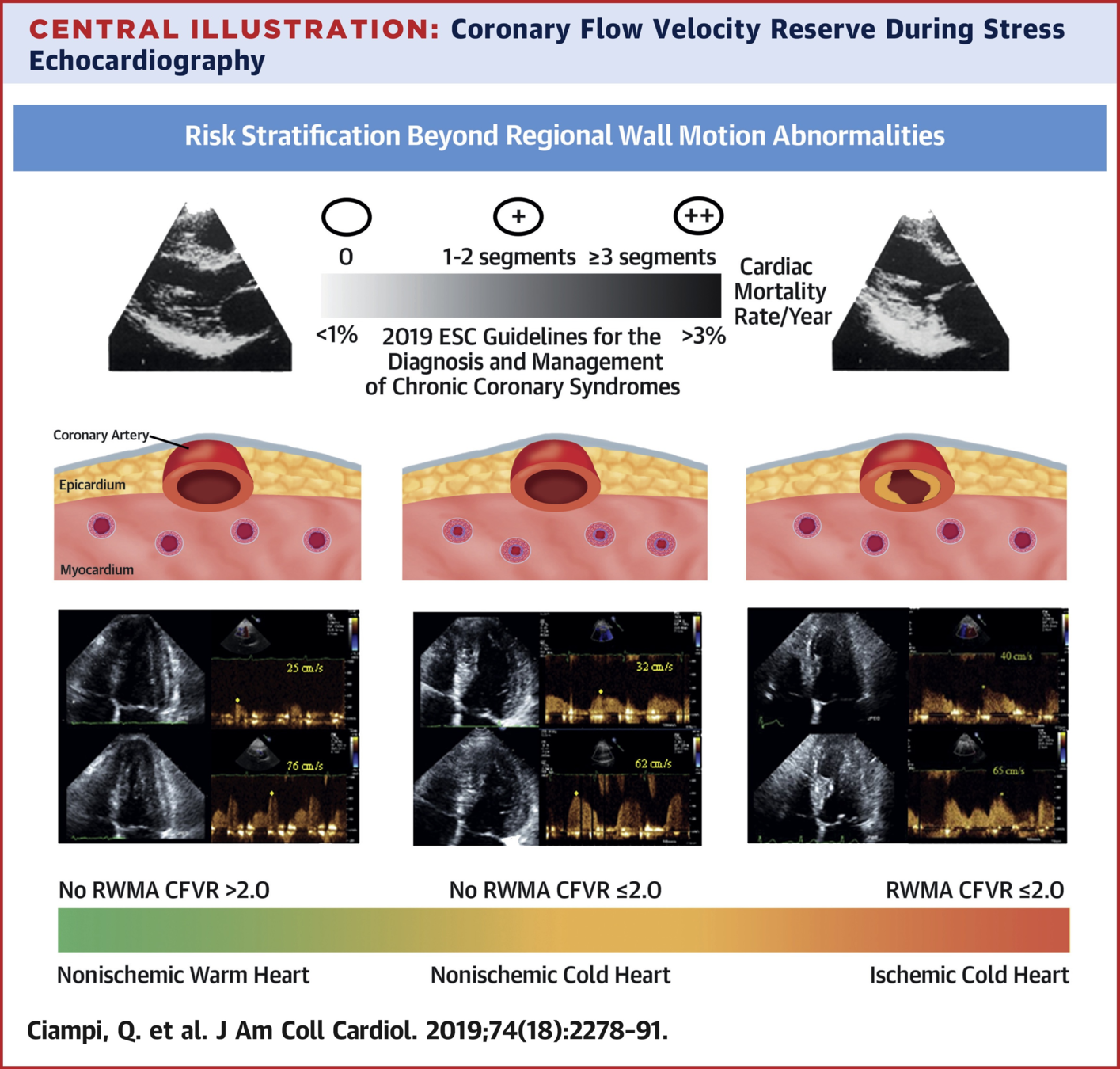
LAD Ischemia
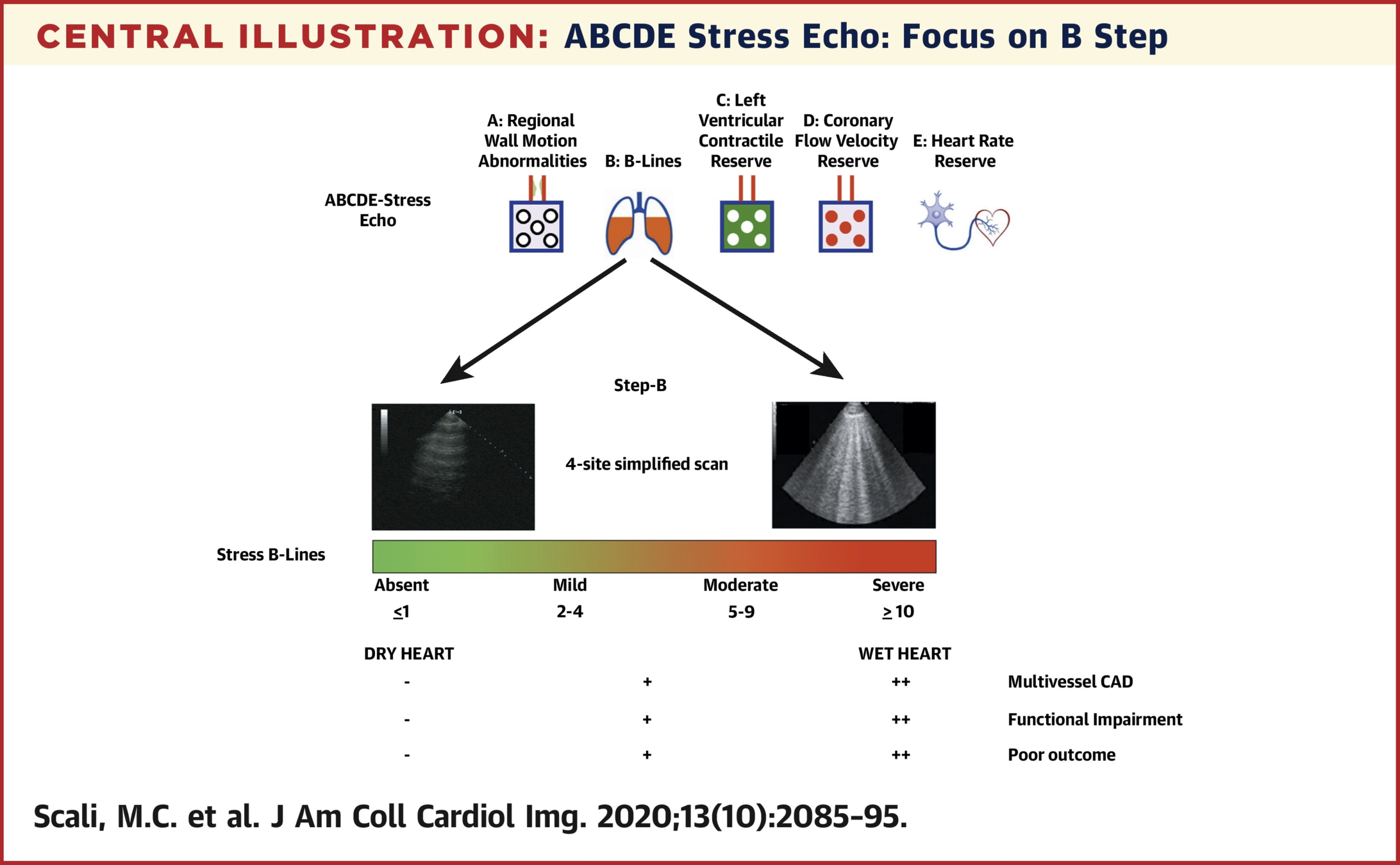
Treatments potentially titratable to ABCDE risk score
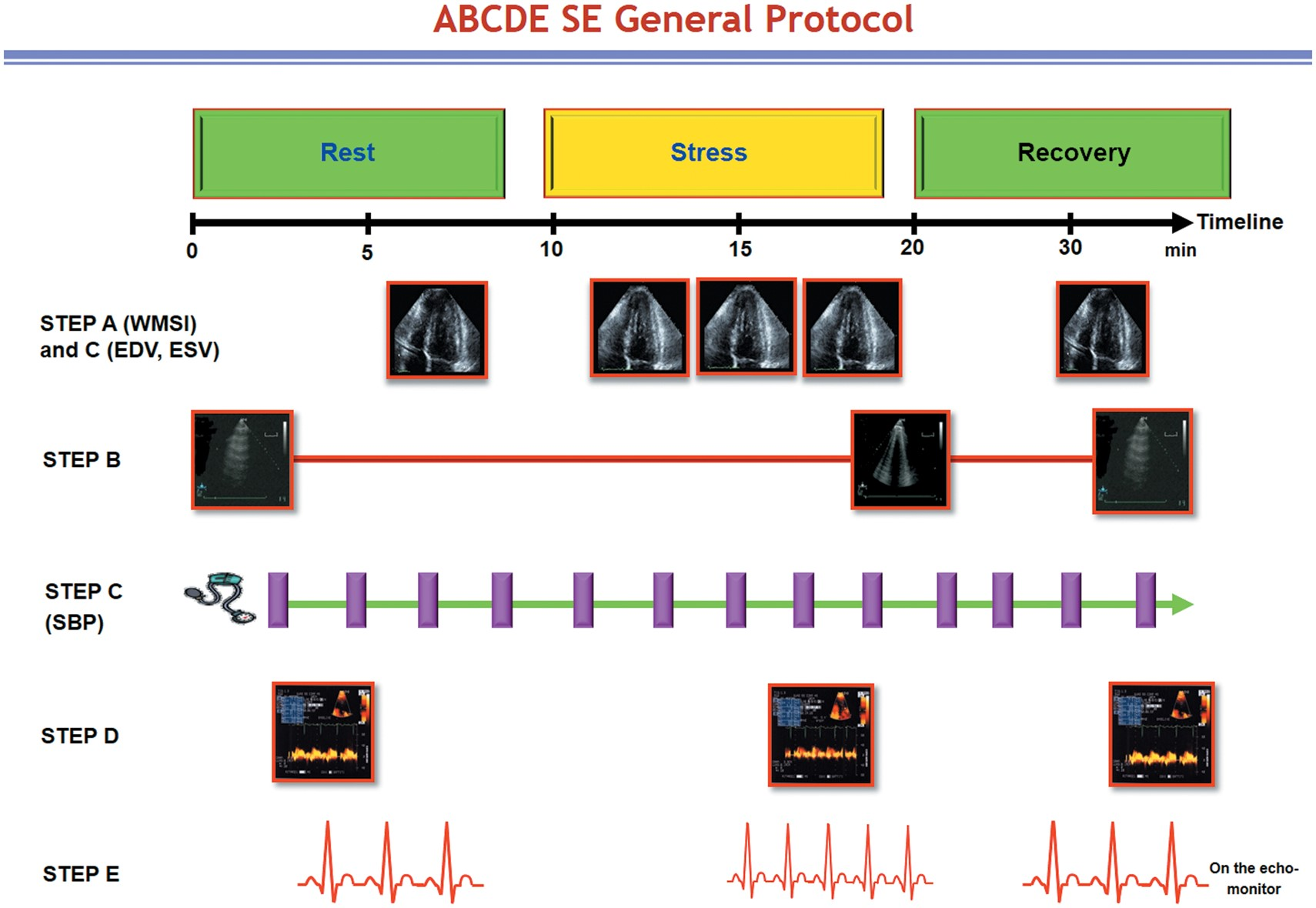
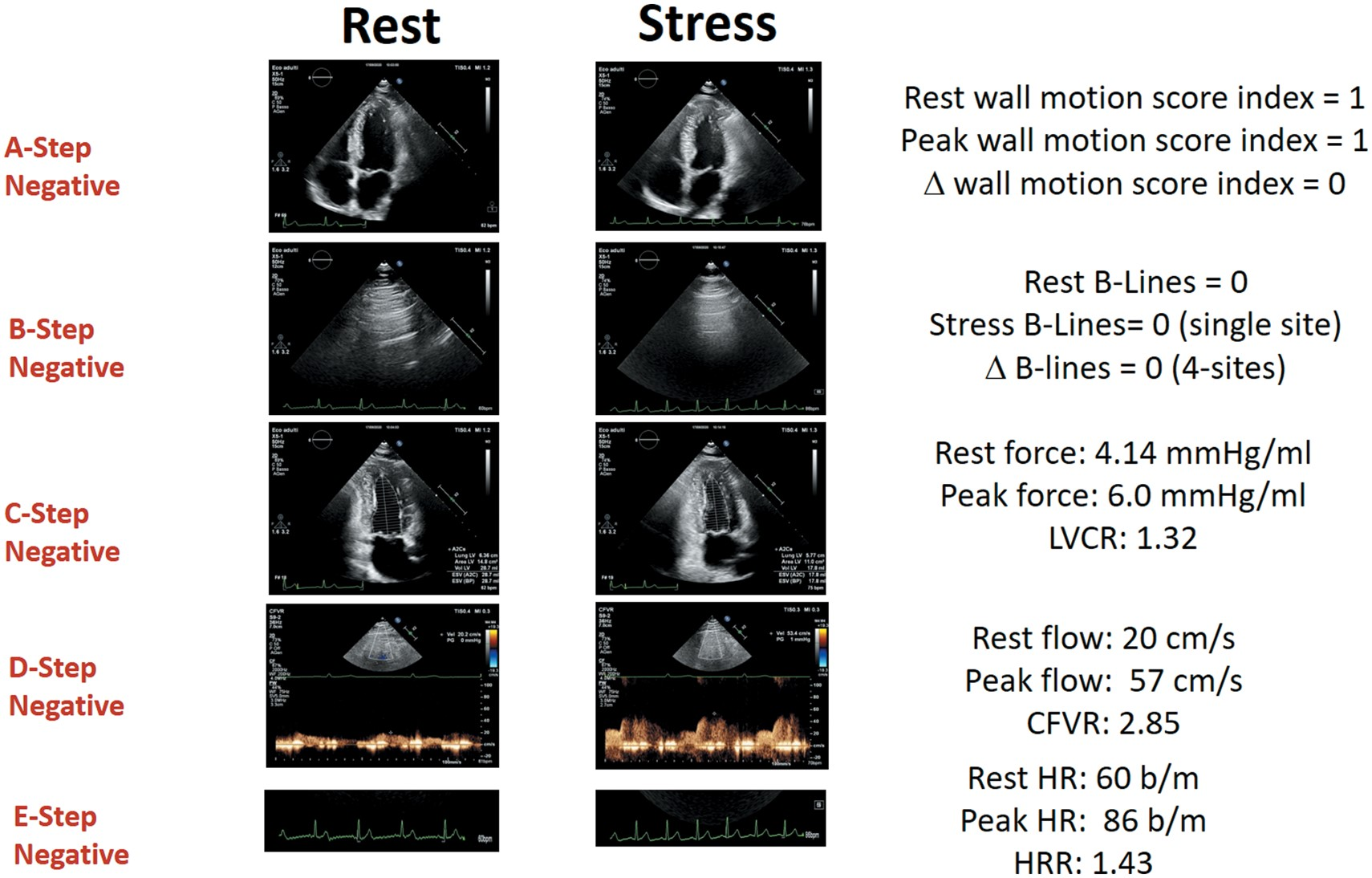
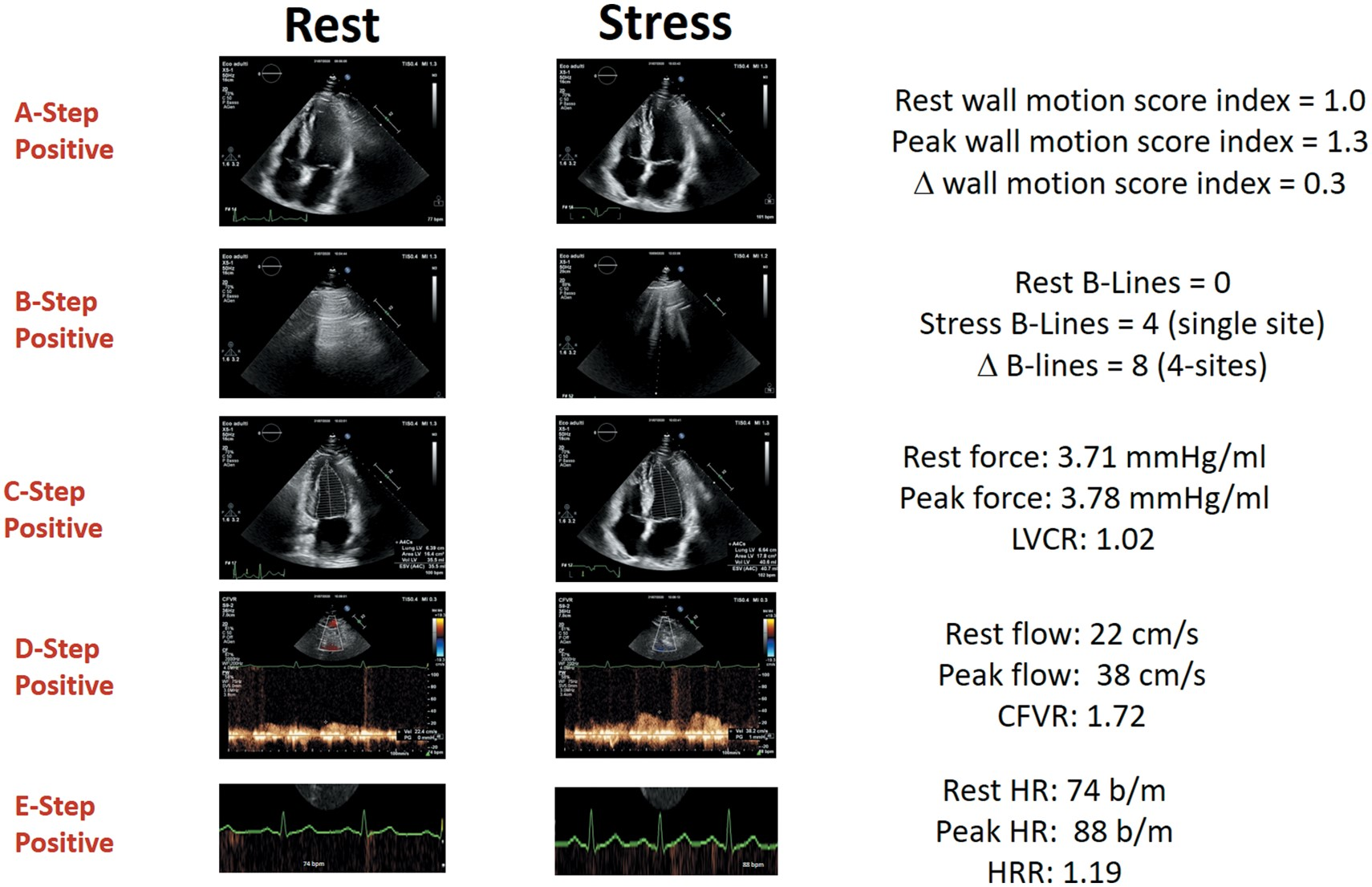
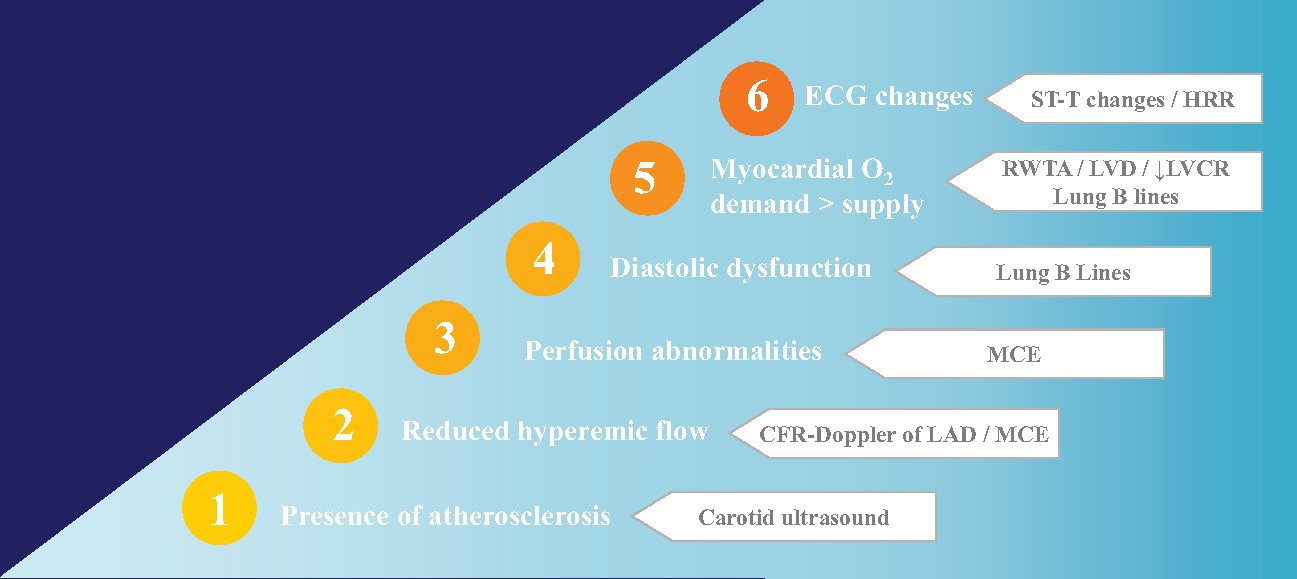
ABCDE + F (regurgitant flow) G (LVOT gradients) L (left atrial volume/function) P ( pulmonary and LV pressures) L (RV function)
By Atul Jaidka



