



Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
https://www.ahajournals.org/doi/pdf/10.1161/JAHA.120.017559
https://www.ahajournals.org/doi/pdf/10.1161/JAHA.120.017559
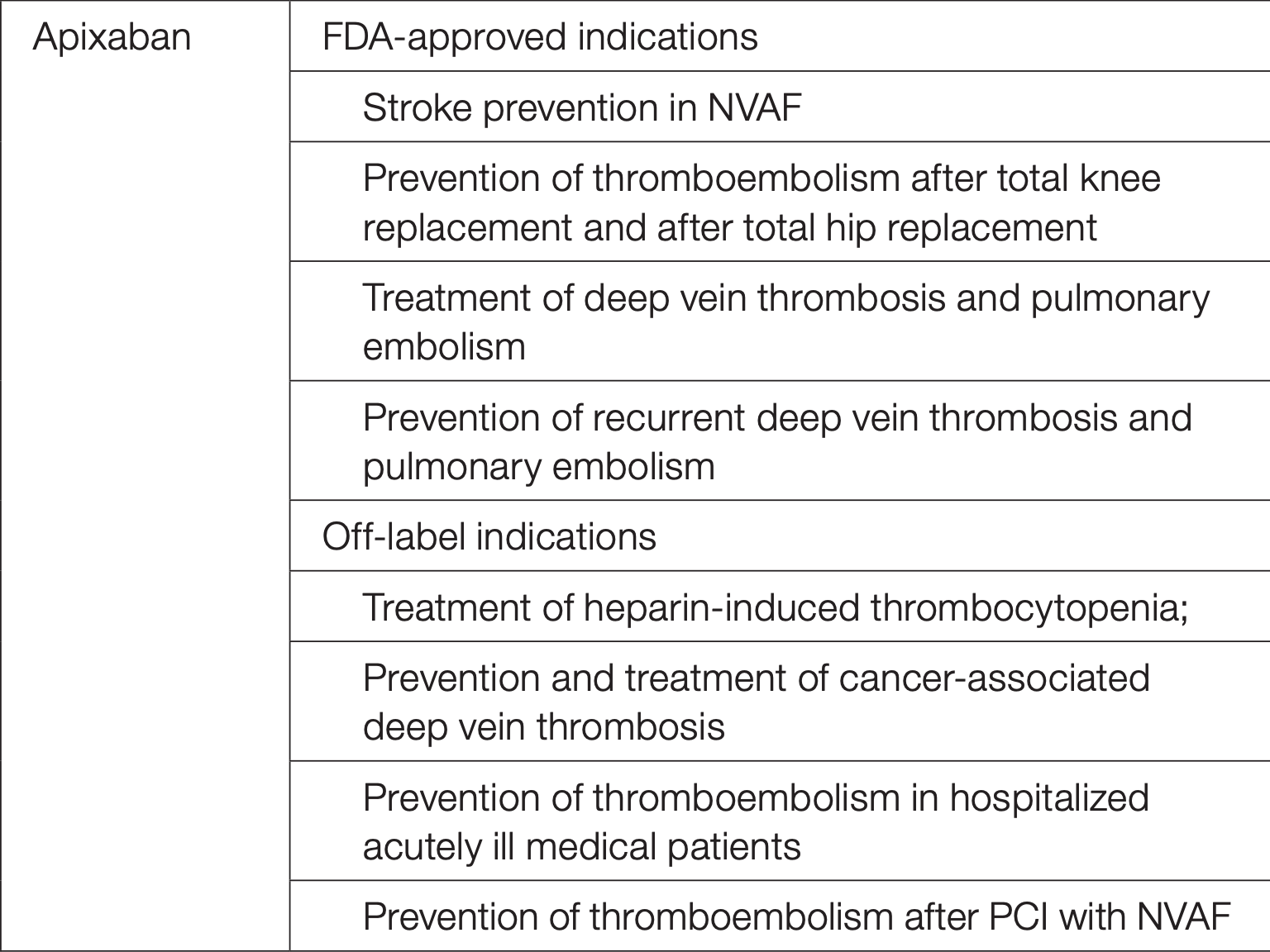
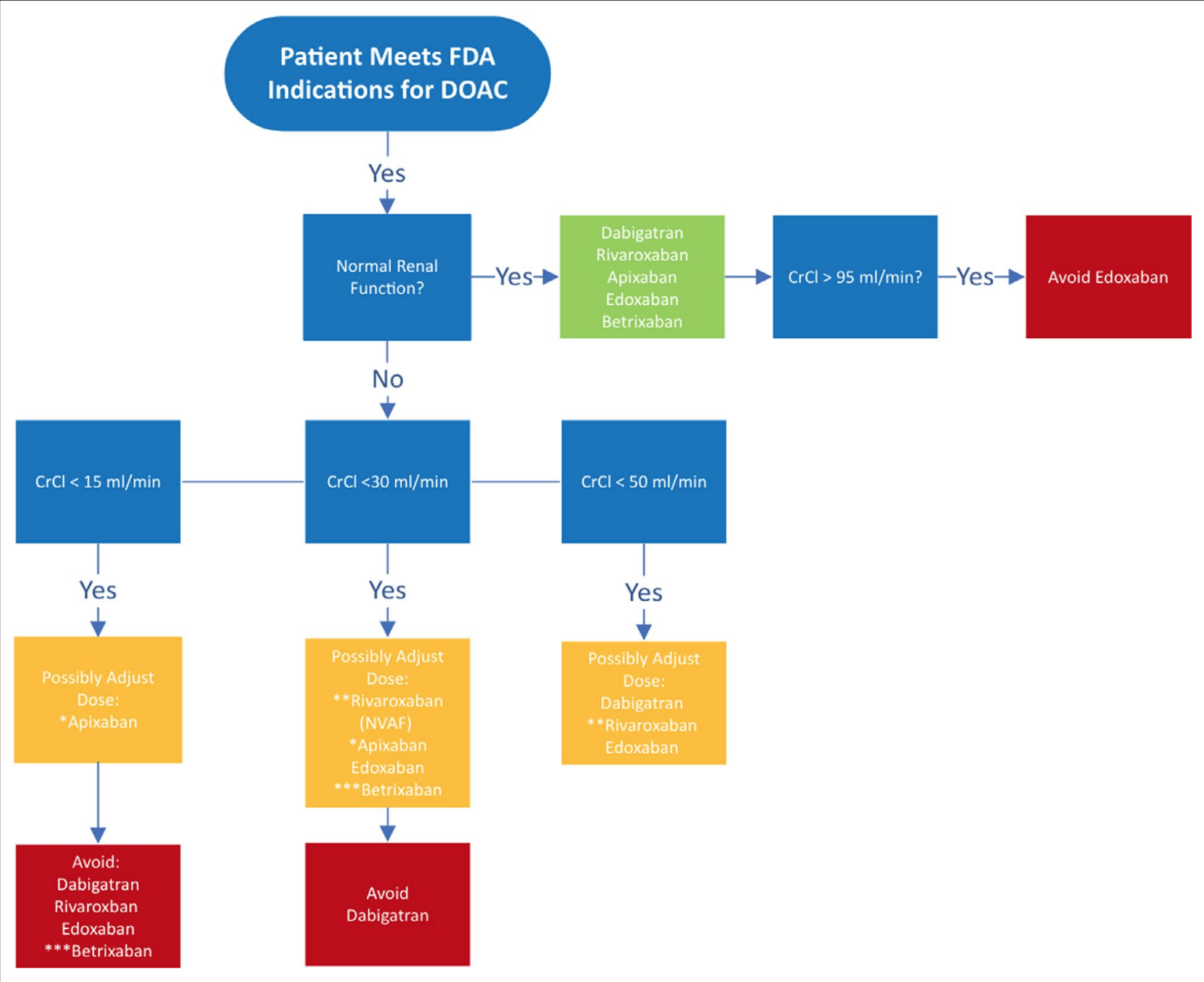
Severe or end-stage renal disease (ESRD) not requiring dialysis: Apixaban or warfarin is considered appropriate (AHA/ACC/HRS [January 2014]; AHA/ACC/HRS [January 2019]). Some experts recommend apixaban 2.5 mg twice daily for CrCl 15 to 29 mL/minute (ACCP [Lip 2018]).
https://www.ahajournals.org/doi/pdf/10.1161/JAHA.120.017559
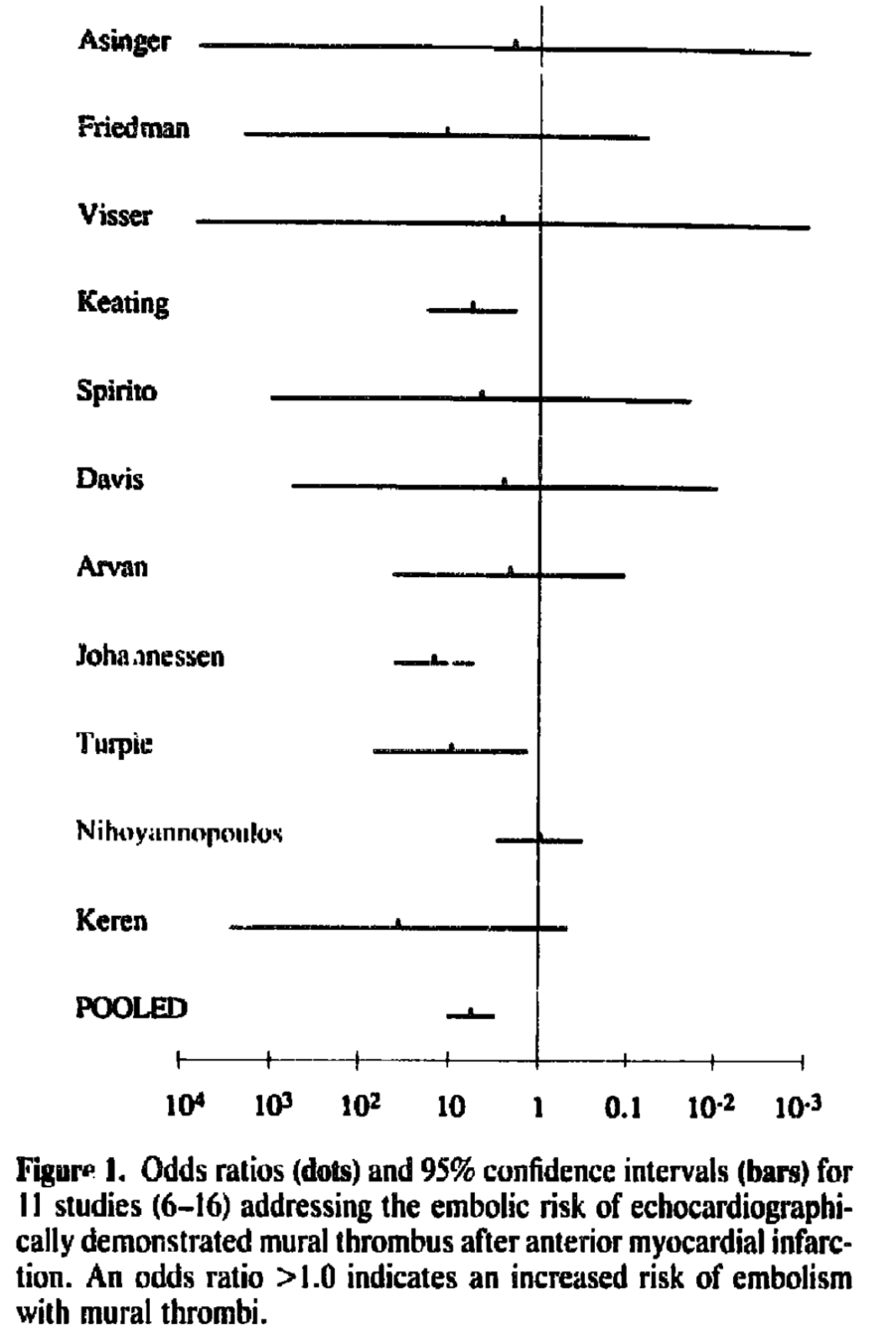
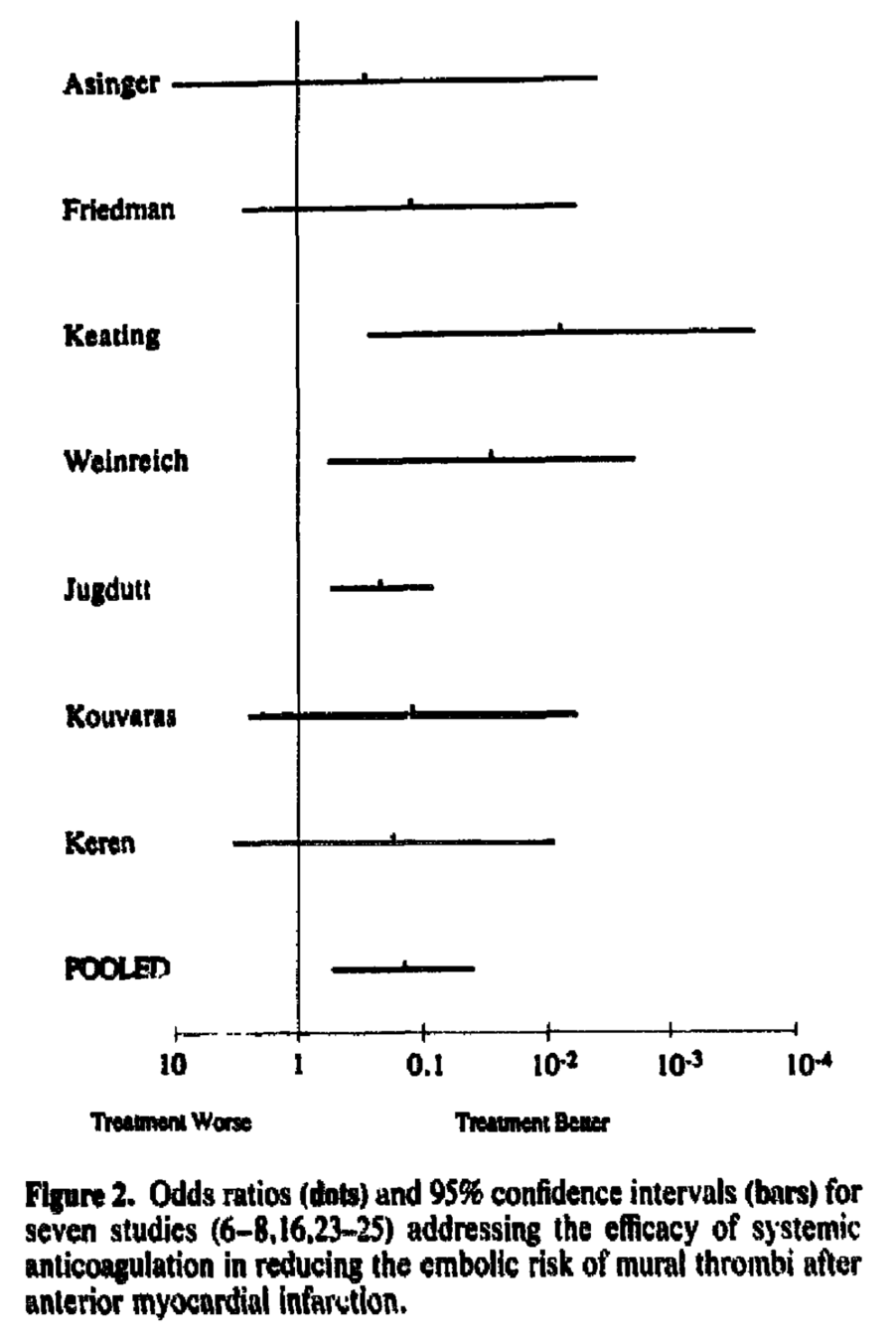
Meta-analysis from 1993 that looked at embolization and benefit of anticoagulation
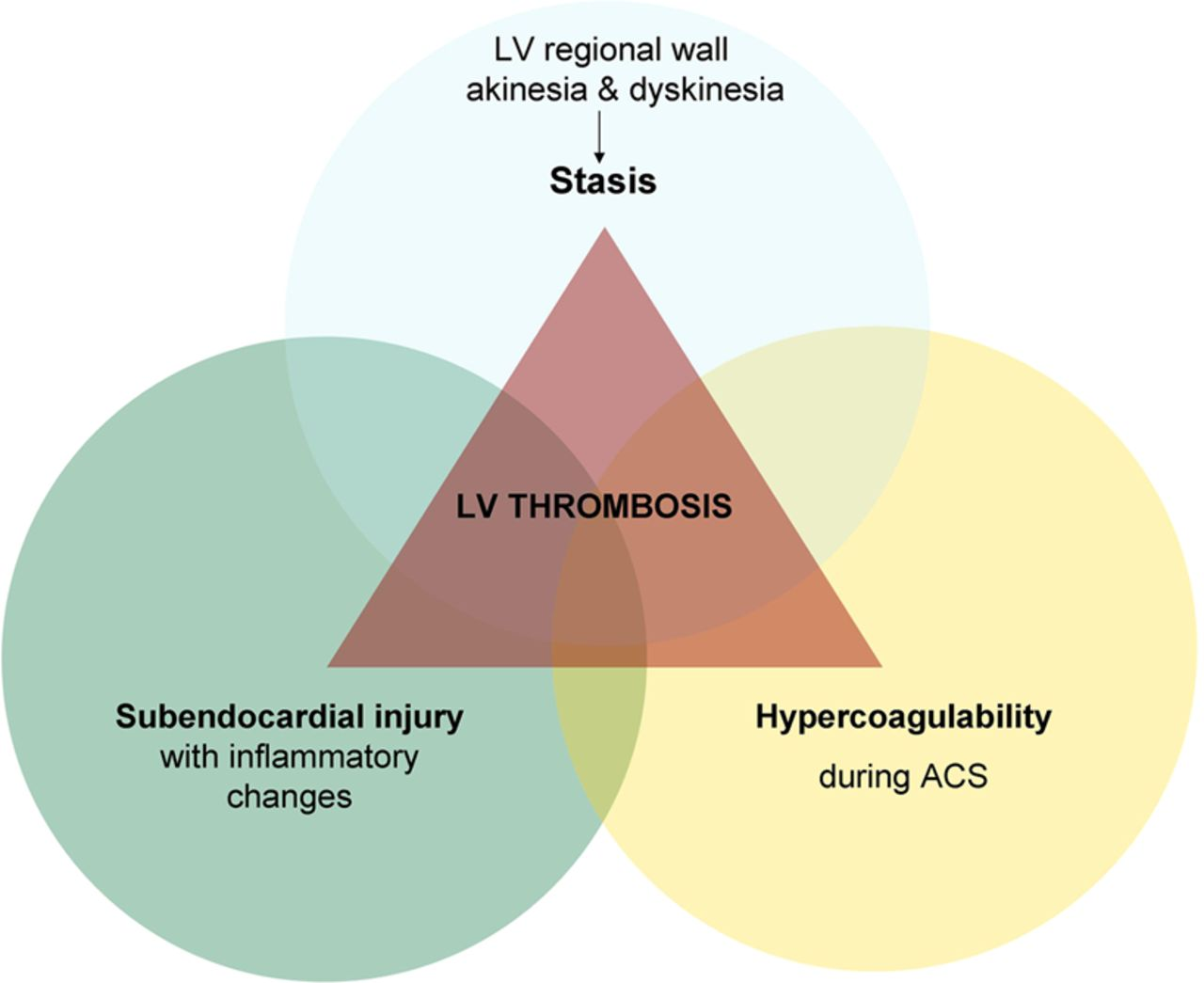
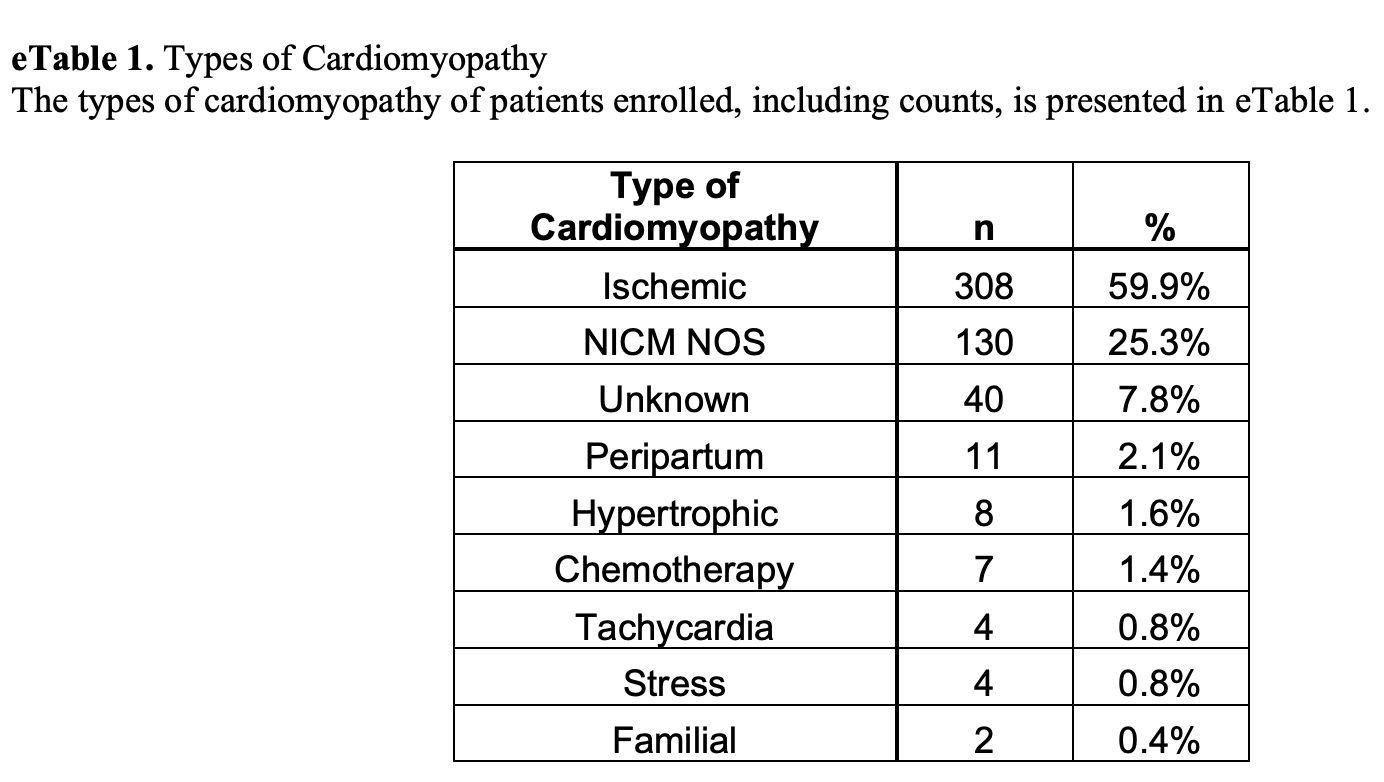
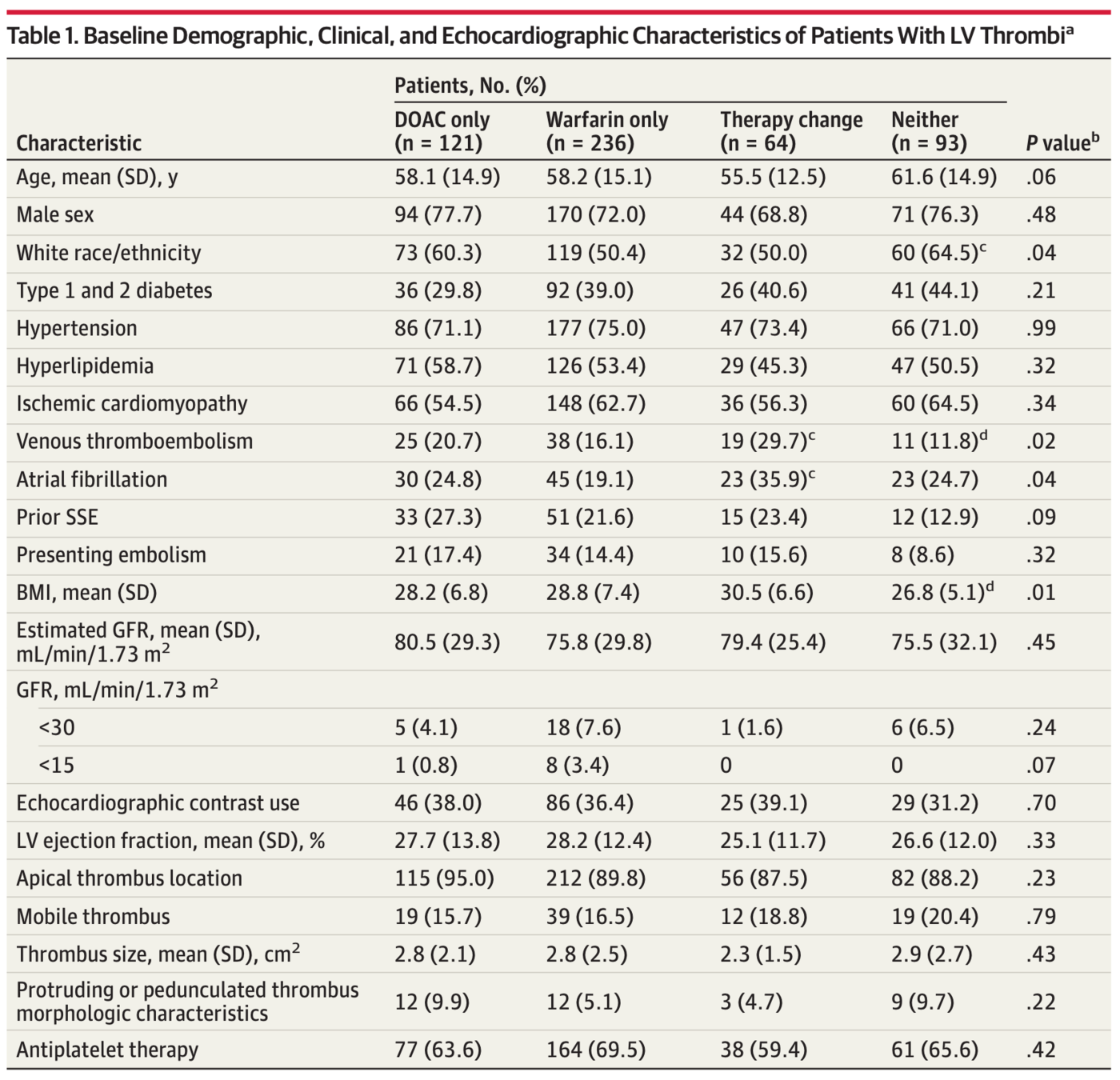
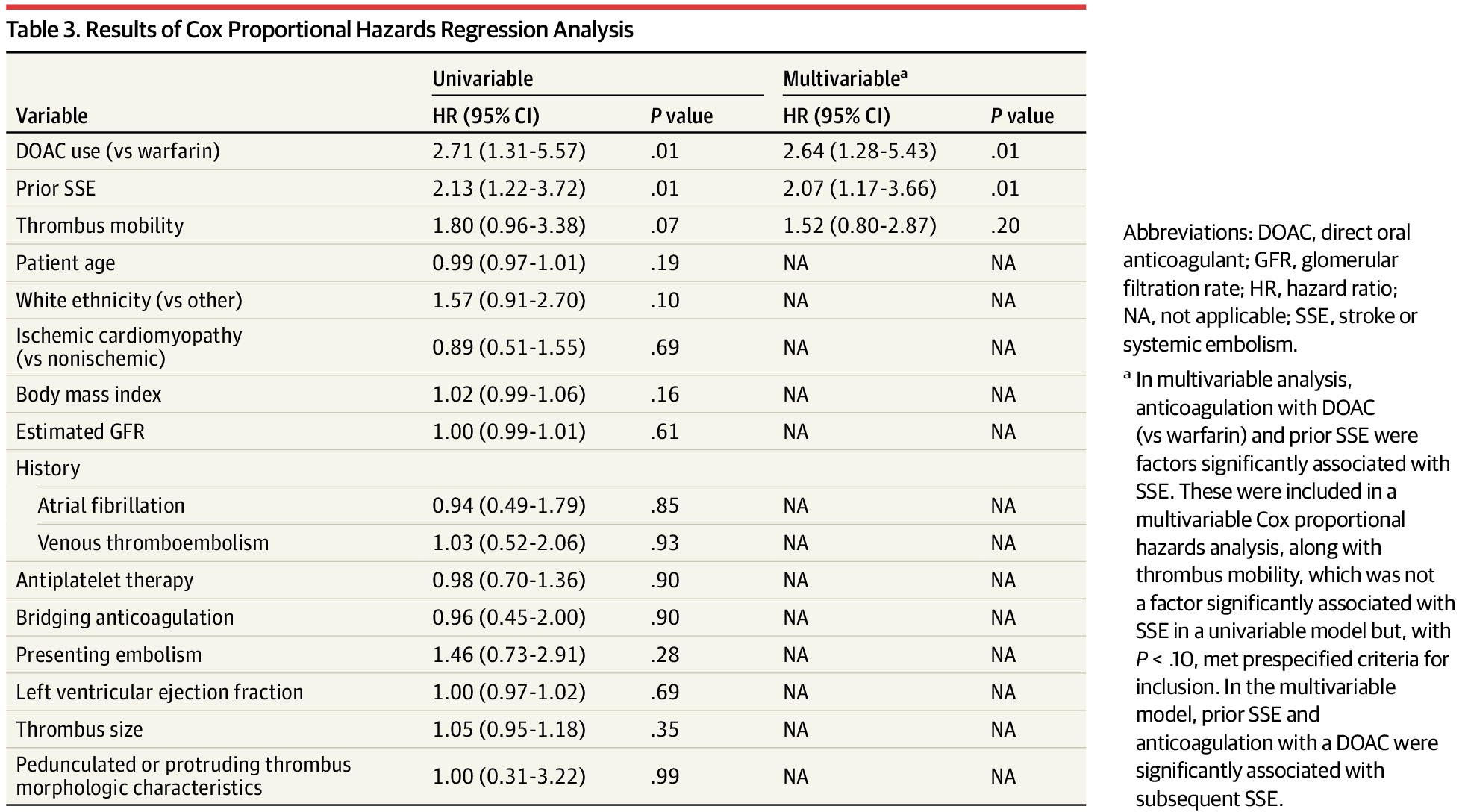
A total of 514 patients (379 men; mean [SD] age, 58.4 [14.8] years) who had echo diagnosed LV thrombi were identified
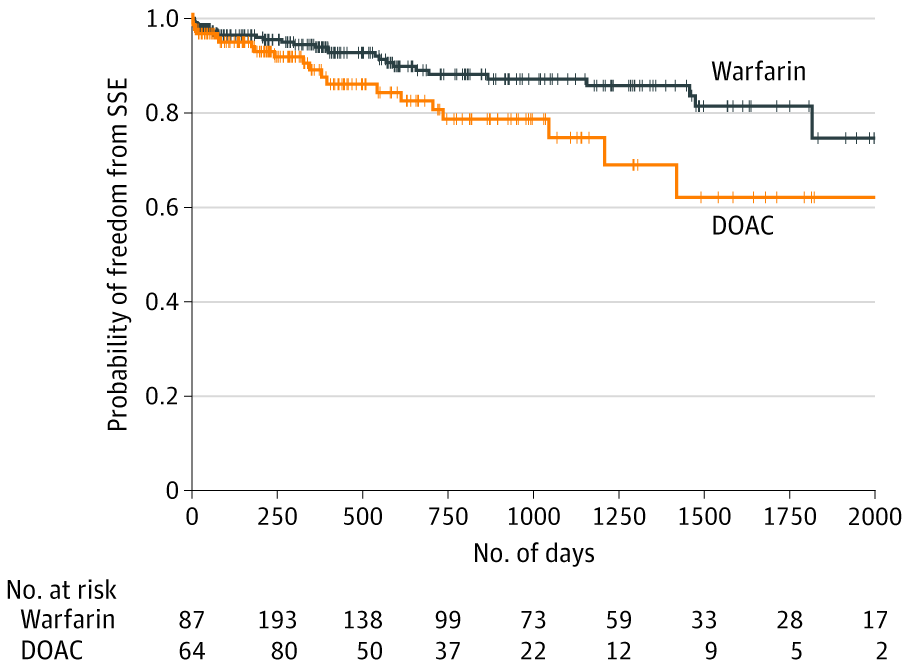
Mantel-Byar P < .001.
https://jamanetwork.com/journals/jamacardiology/fullarticle/2764430
"These therapies are not a panacea"
By Atul Jaidka



