Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
https://www.acc.org/latest-in-cardiology/articles/2016/07/12/13/06/cmr-and-pericardial-masses
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5128889/
UTD
https://academic.oup.com/ehjcimaging/article/12/11/E43/2396998
https://academic.oup.com/ehjcimaging/article/12/11/E43/2396998
https://academic.oup.com/ehjcimaging/article/12/11/E43/2396998
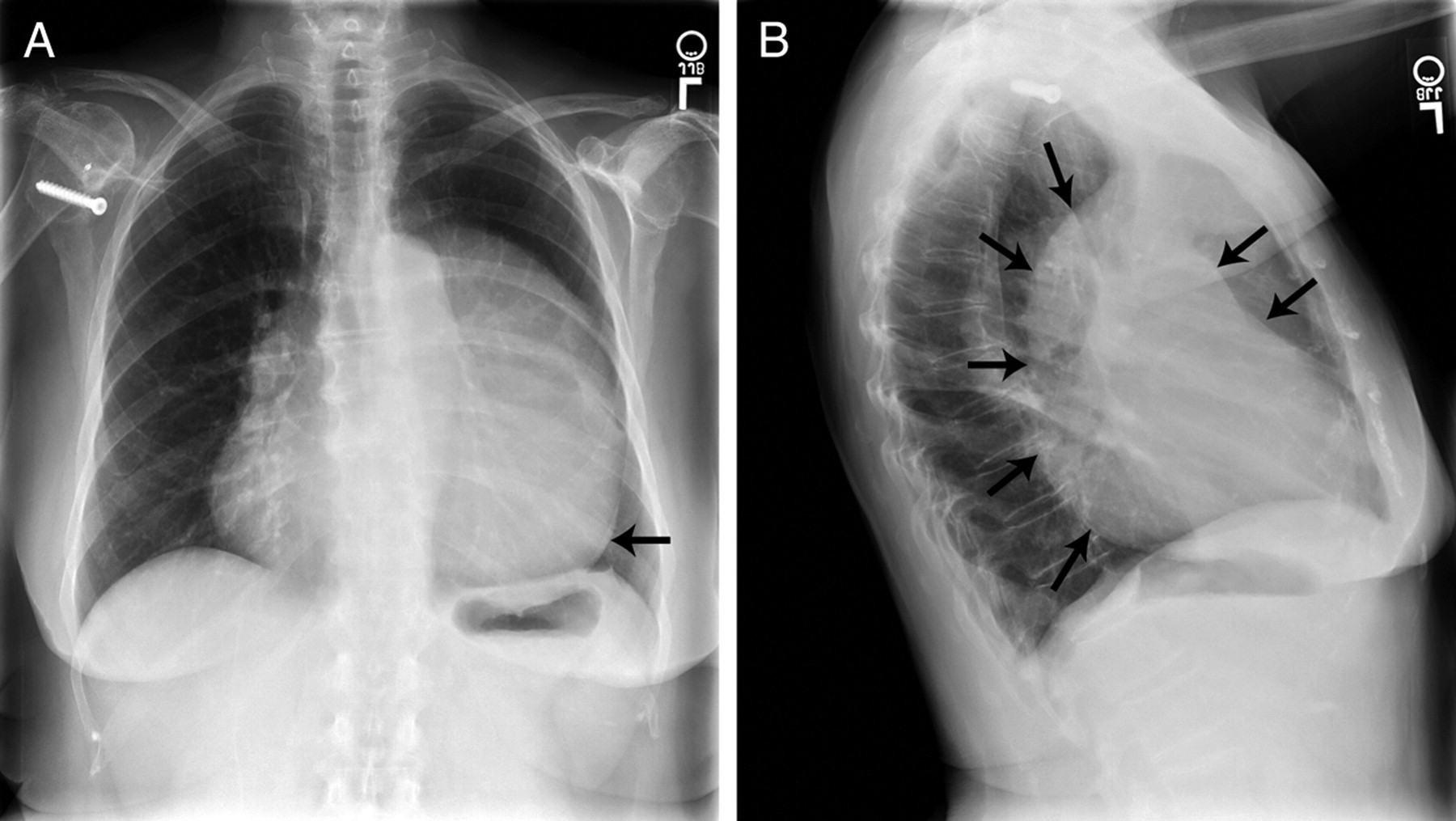
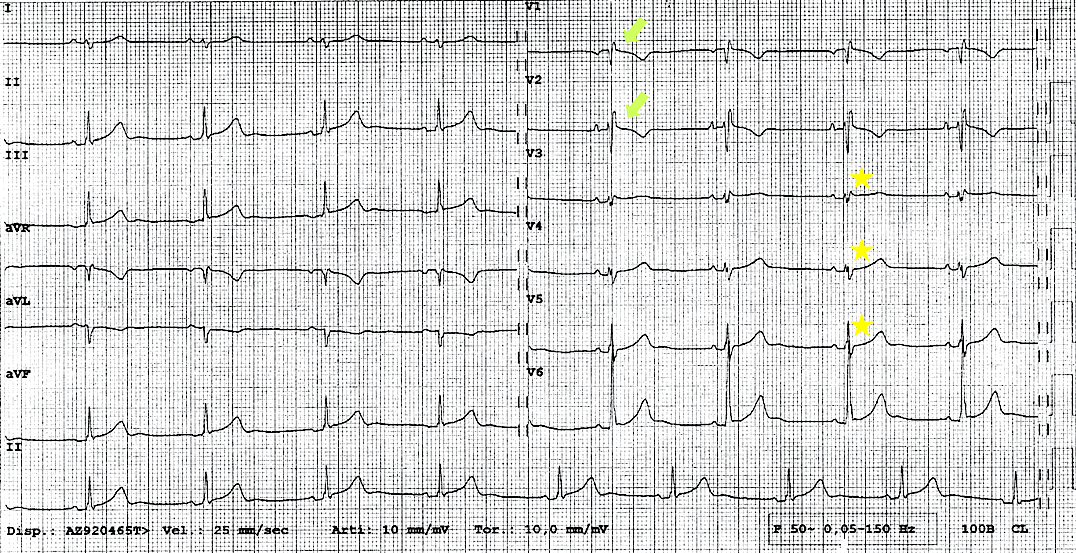
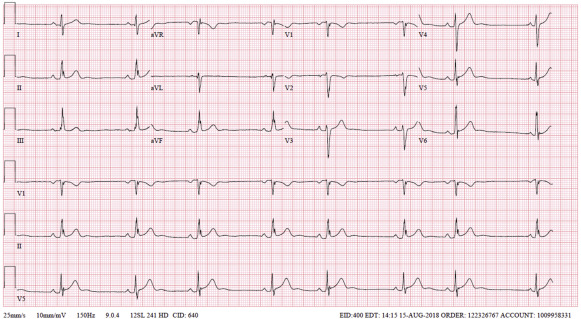
ECG: incomplete RBBB, poor R wave progression, right axis deviation
29M presented with atypical chest pain
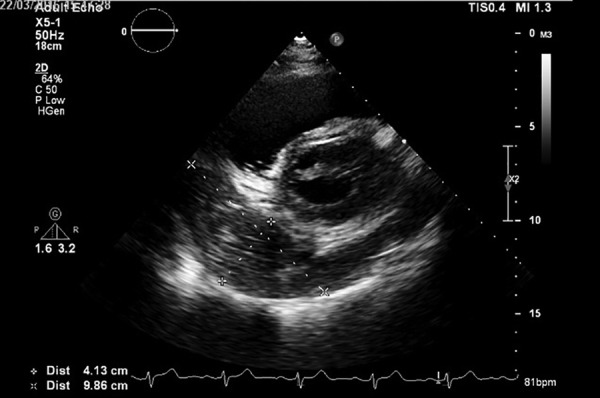
A4C Medial
A4C Lateral
Note posteriorly directed apex and exaggerated mobility. "Teardrop" ventricles. Usual apical location shows RV predominance requiring supine positioning
https://www.cvcasejournal.com/article/S2468-6441(19)30165-3/fulltext
Right ventricle appears enlarged, teardrop-shaped heart, and hypermobile heart
https://www.cvcasejournal.com/article/S2468-6441(19)30165-3/fulltext
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3998169/
https://www.jacc.org/doi/pdf/10.1016/j.jacc.2011.05.052
UTD
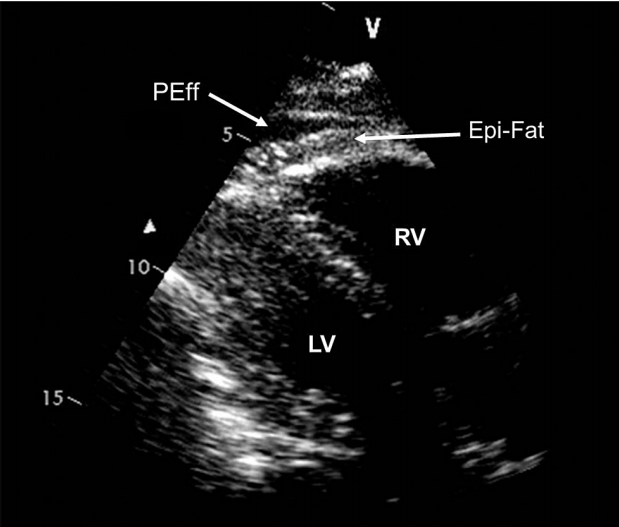
https://www.journal-of-cardiology.com/article/S0914-5087(14)00203-2/pdf#:~:text=On%20the%20other%20hand%2C%20the,(pericardi%2Dal%20fat).
ASE
ASE
ASE
UTD
UTD
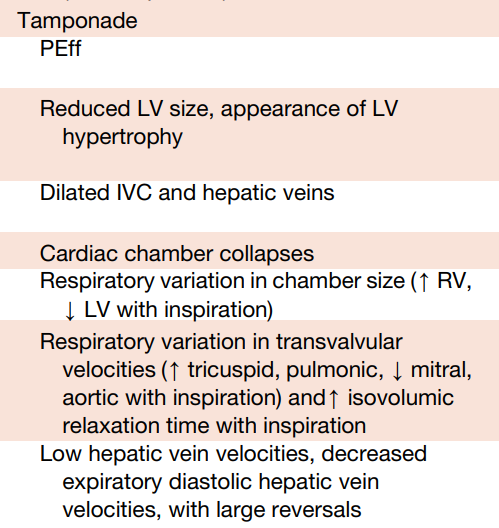
1 + either 2 or 3 = 87% sensitive and 91% specific
By Atul Jaidka
Echo Rounds



