





Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
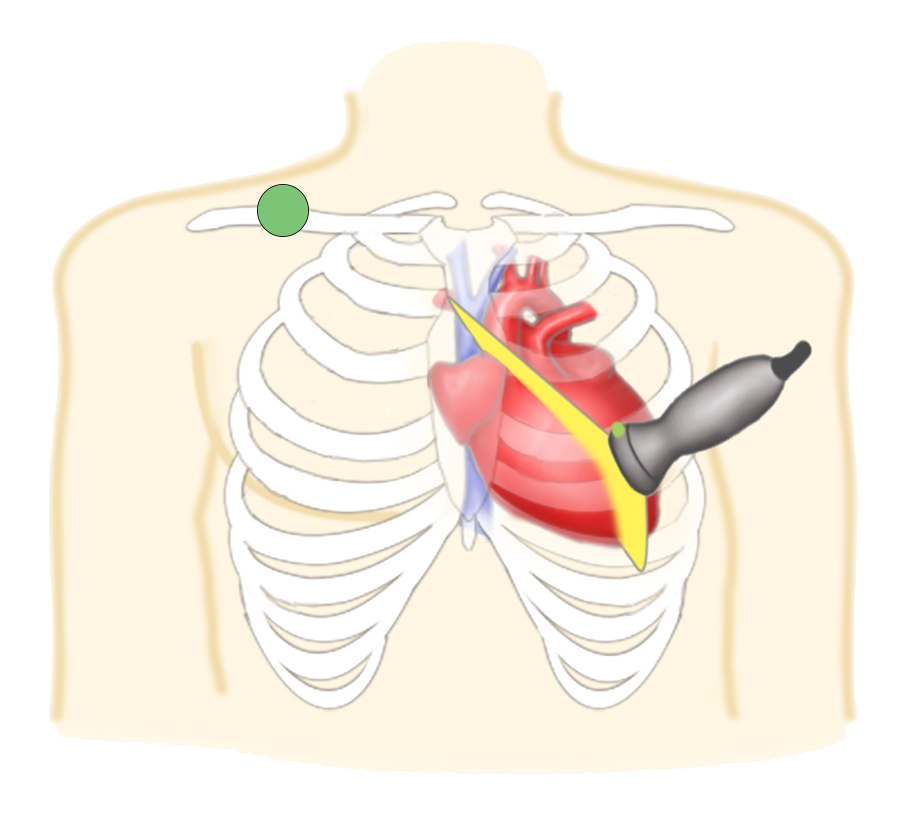
Troubleshooting
If no view, make large concentric circles
Once you see heart, slowly focus in
+++GEL
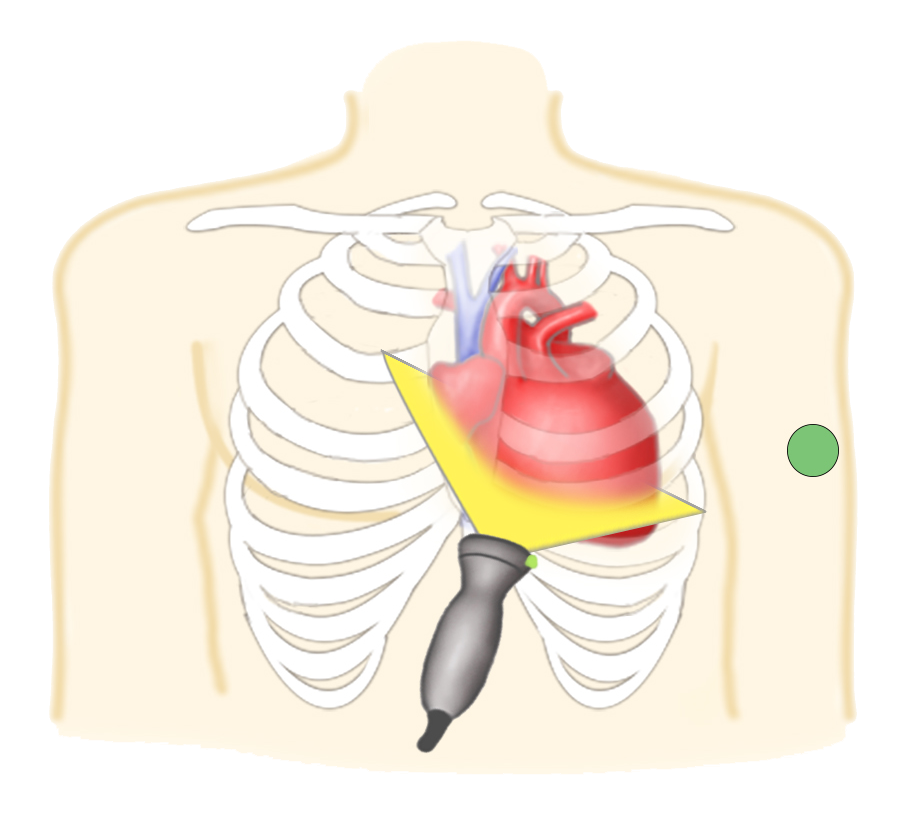
Left lateral decubitus position
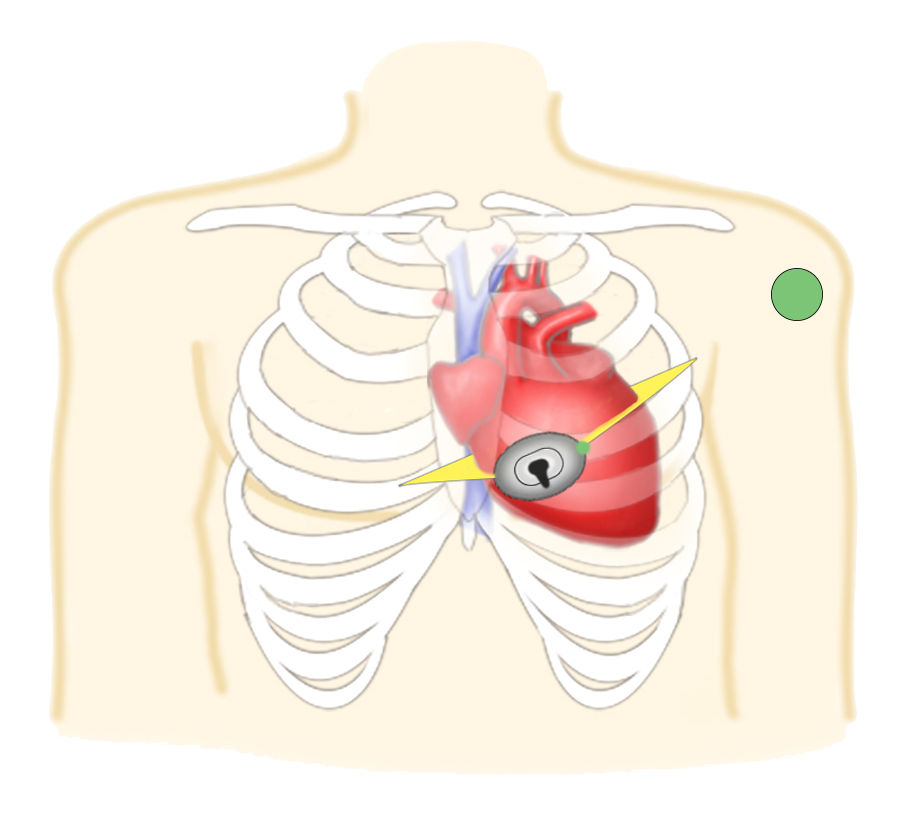
Troubleshooting
If no view, make large concentric circles
Once you see heart, slowly focus in
Alternatively, start at parasternal short axis and slide down to the apex keep heart in view
+++GEL
Left lateral decubitus position***
False positives
Pleural effusion, free fluid, fat pad
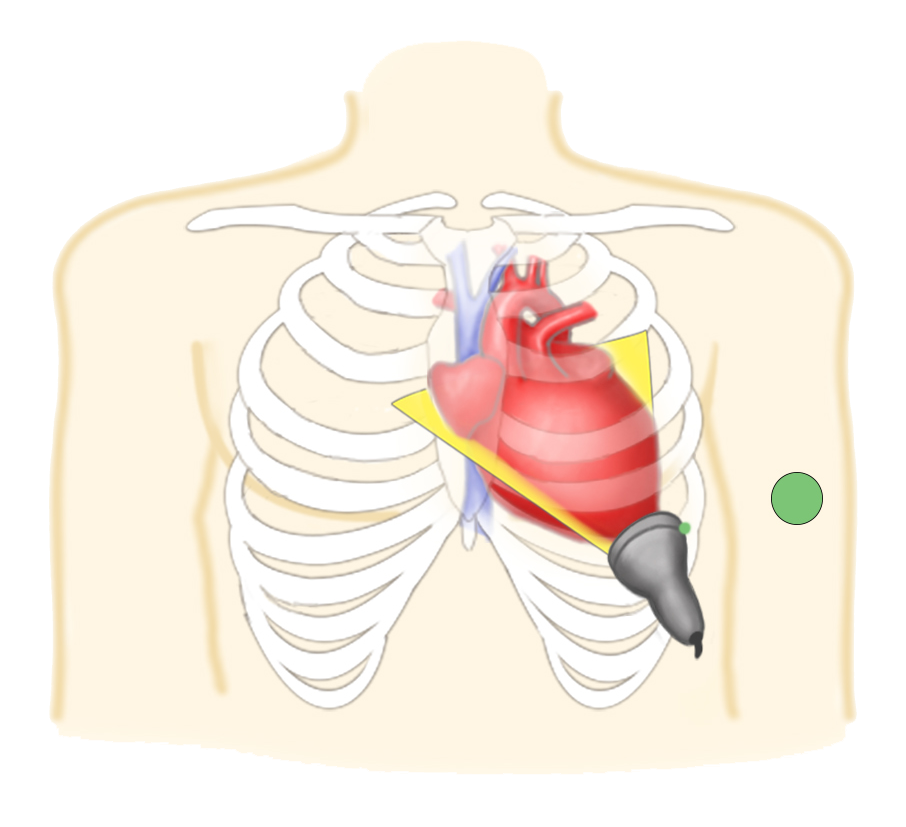
Troubleshooting
Start LOW
GEL
↑ Depth
Bend knees, hands to sides, deep breath & hold
Downward pressure with some upward pressure*
Move to patient’s right to use liver as an acoustic window
By Atul Jaidka



