




Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
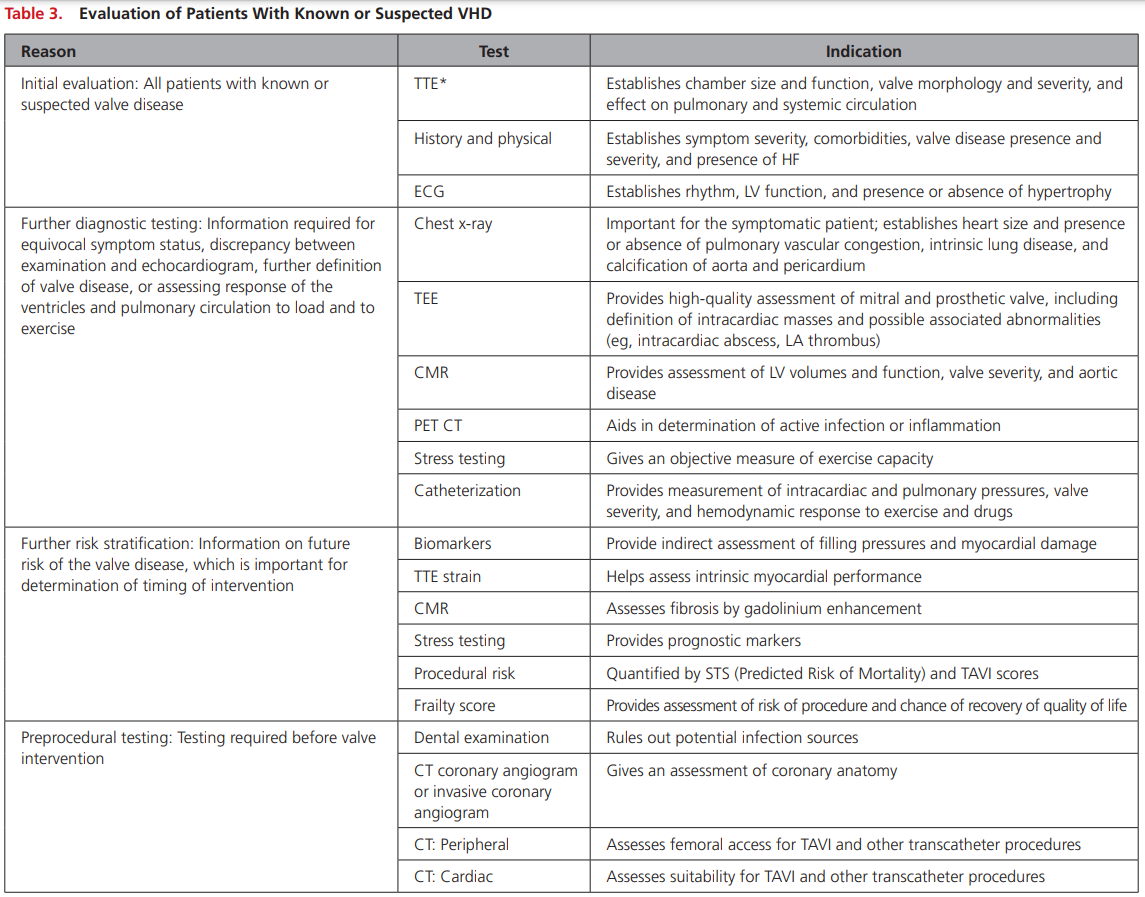
You are seeing a 78 year old female in your outpatient General Internal Medicine clinic for 1 year of progressive shortness of breath. History and physical are otherwise unremarkable but you hear a 2/6 systolic murmur heard throughout the precordium. How do you workup this patient?
Transthoracic Echo:
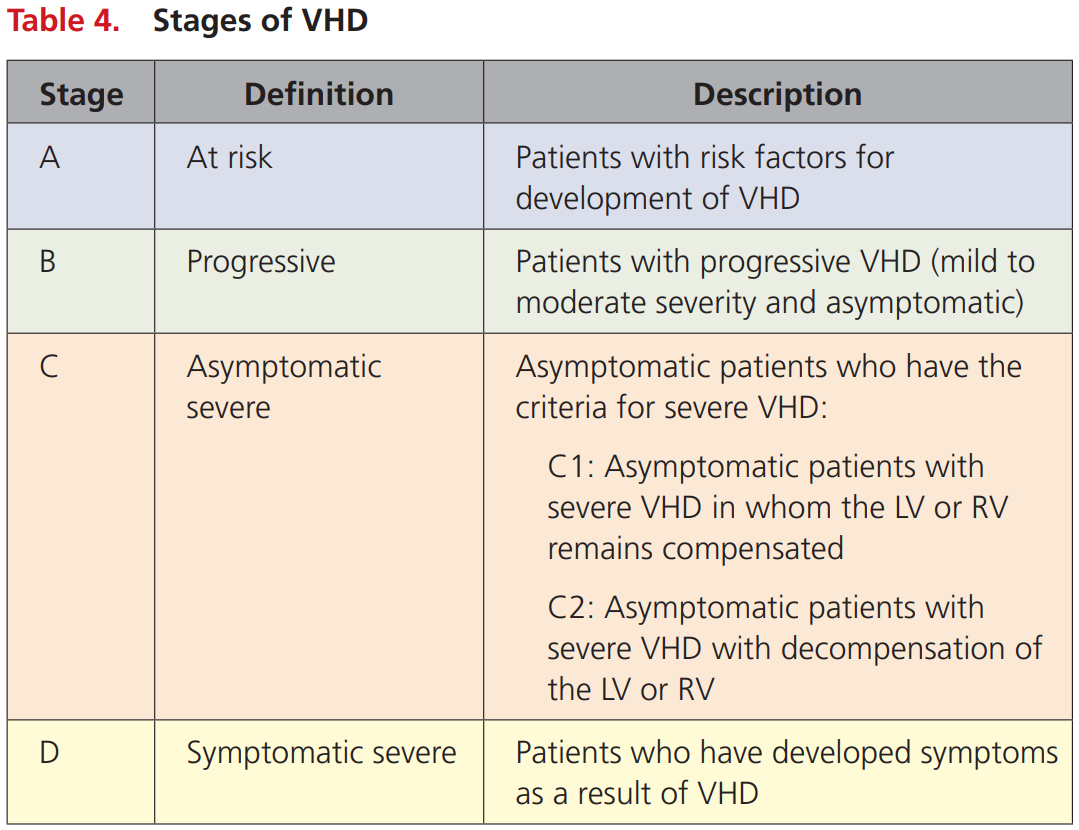
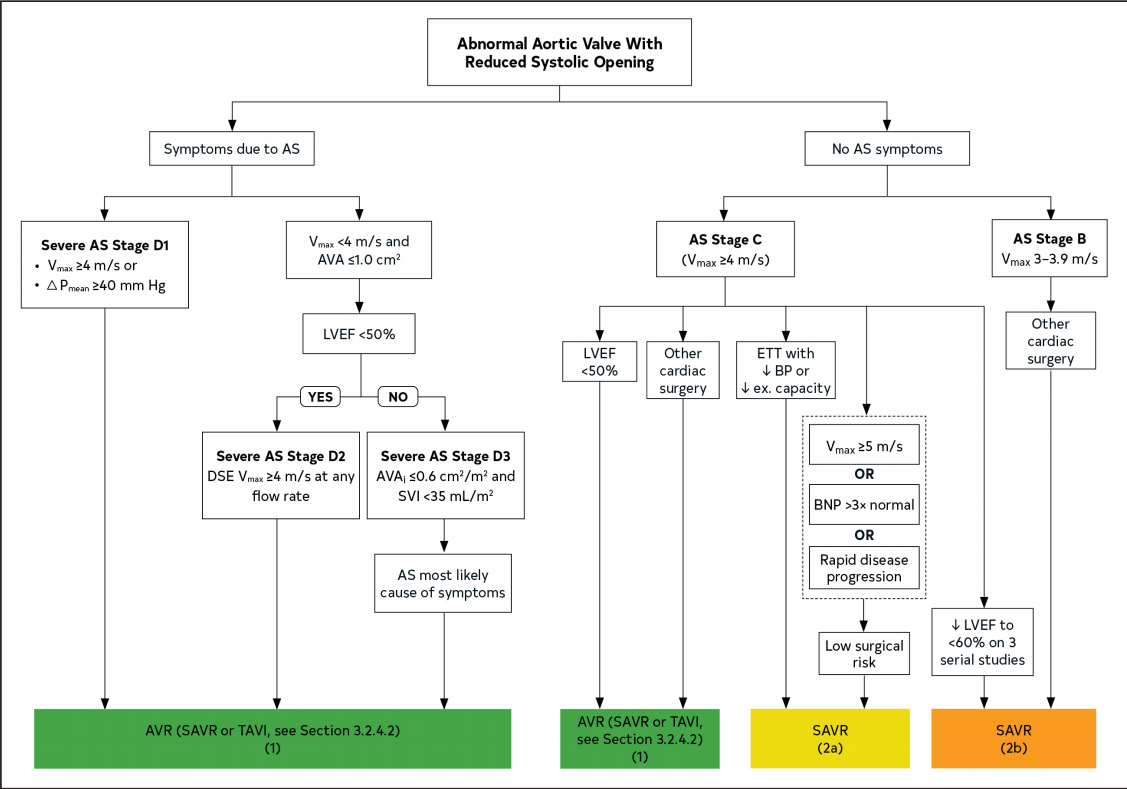
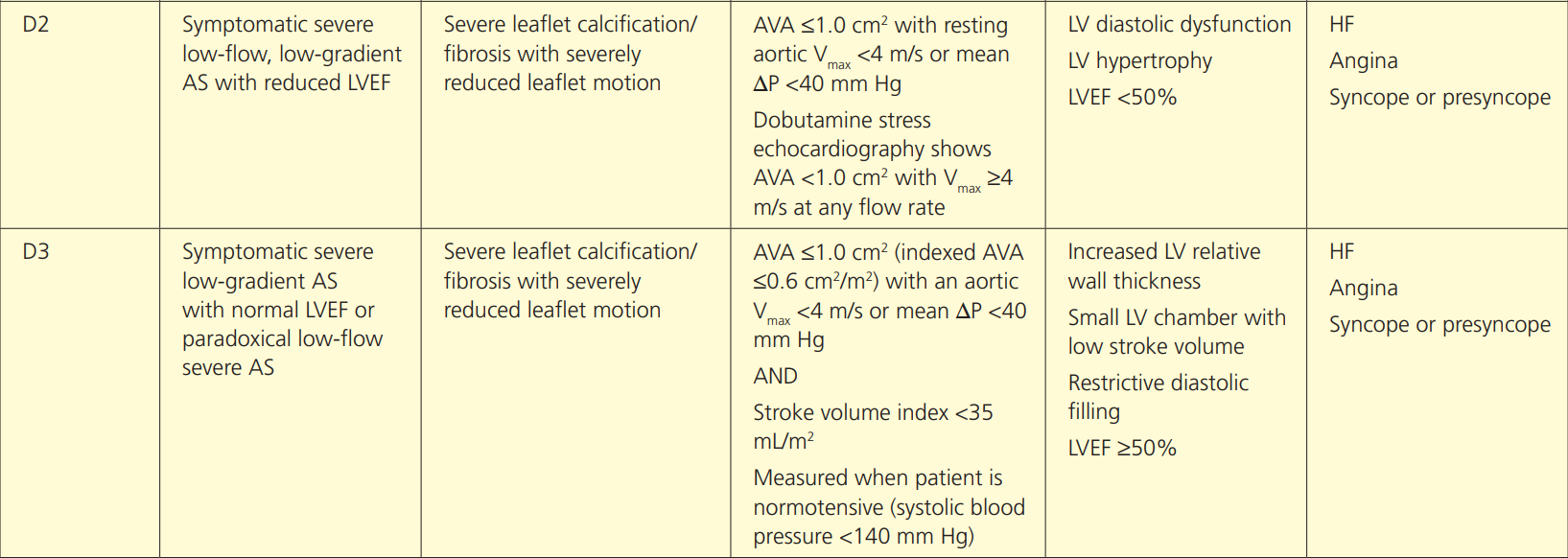
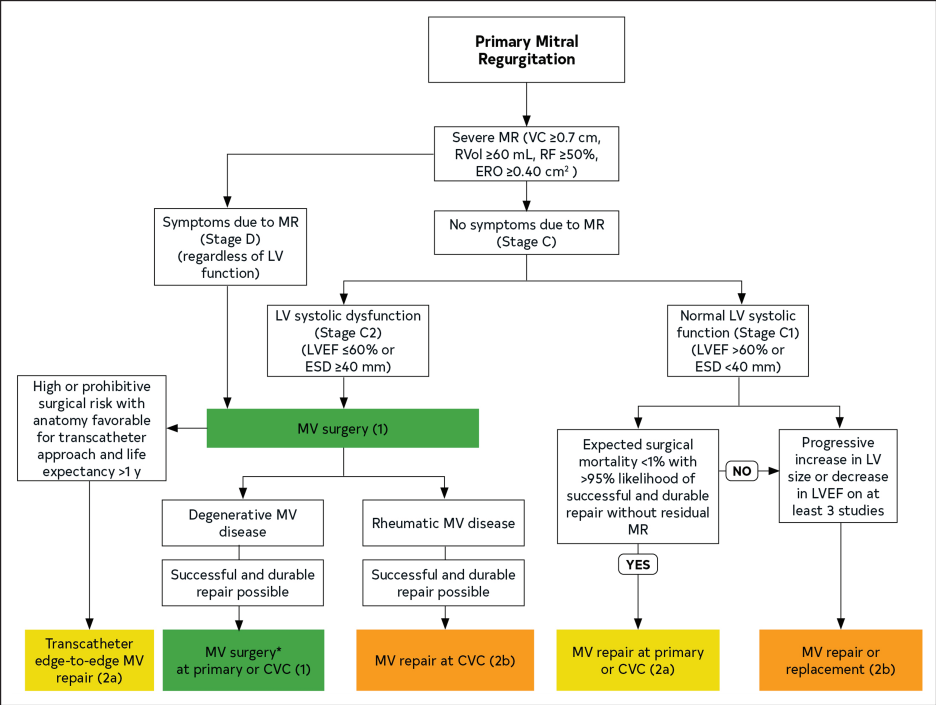
How would you stage this patient?
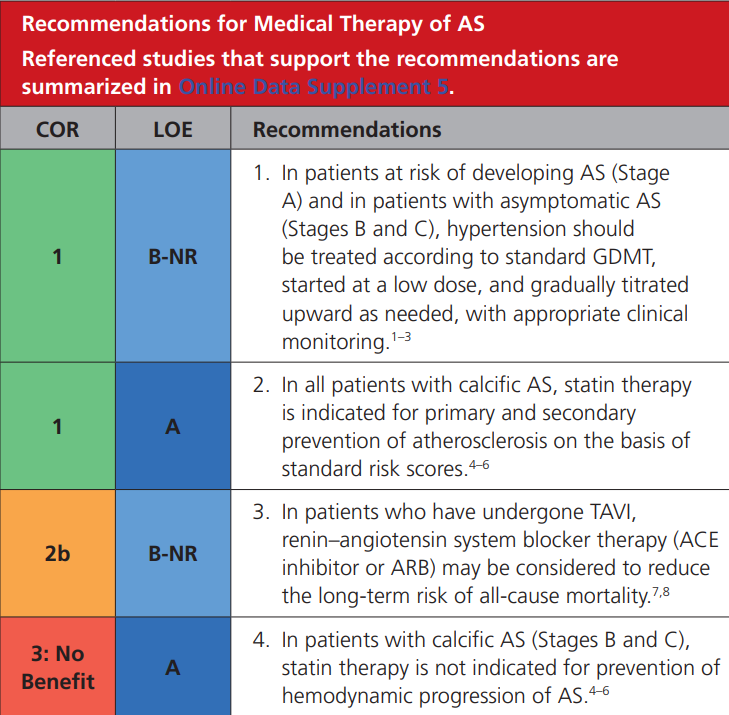
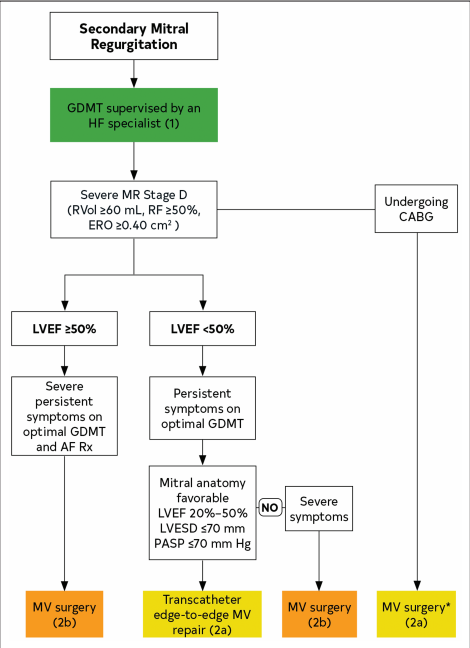
Given the recent echocardiographic findings, how will you manage this patient?
Review article: https://www.ahajournals.org/doi/pdf/10.1161/JAHA.120.016911
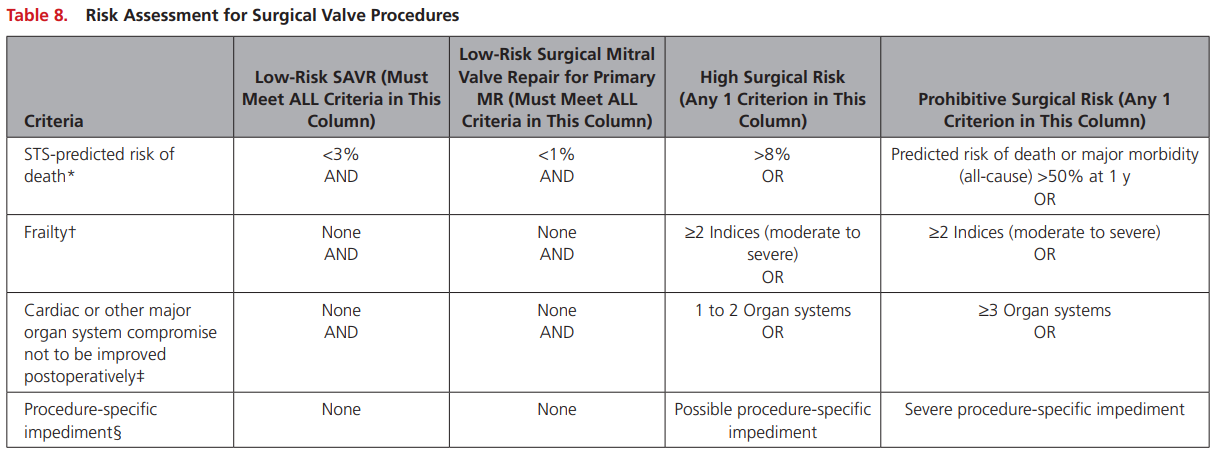
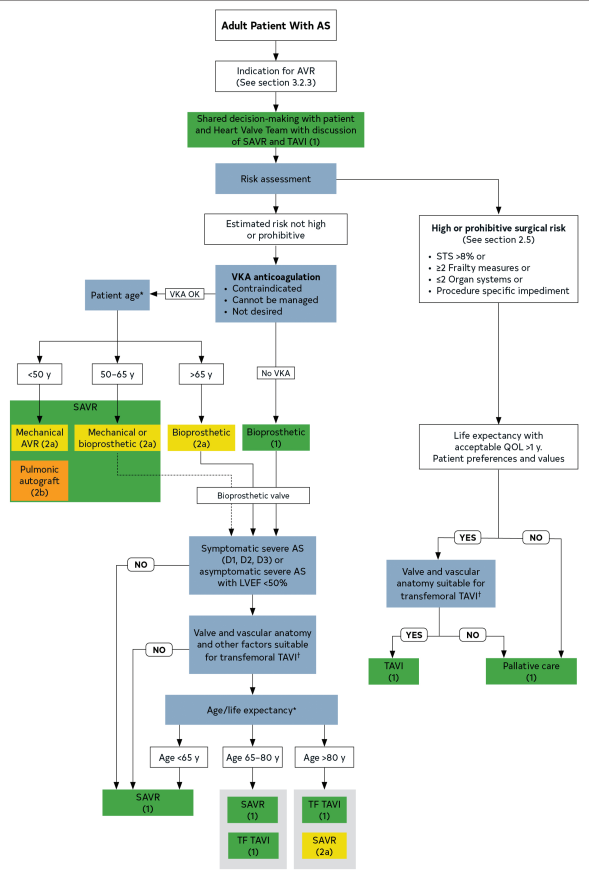
How will you decide if she is a candidate for intervention and what intervention should she get?
*Risk can be assess with STS or EUROSCORE II
†Assess by ADLs or score (ie. FRAILTY-AVR 4 point score)
Note: don't memorize scores but understand what the contain
Text
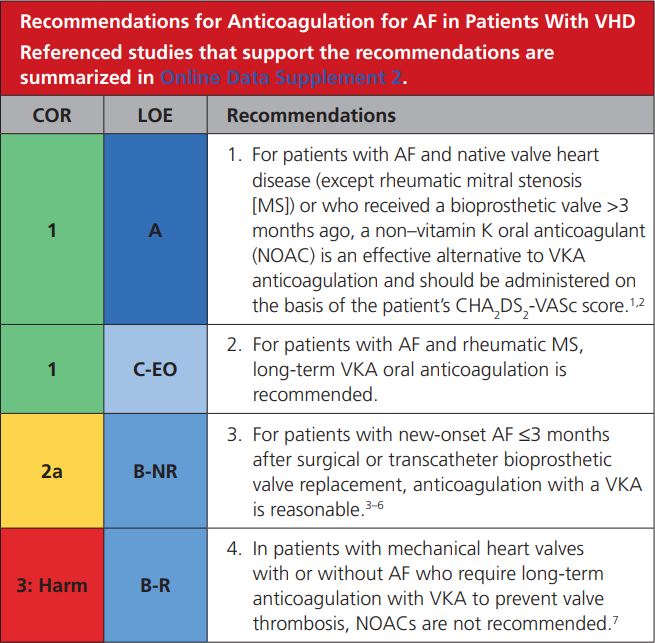
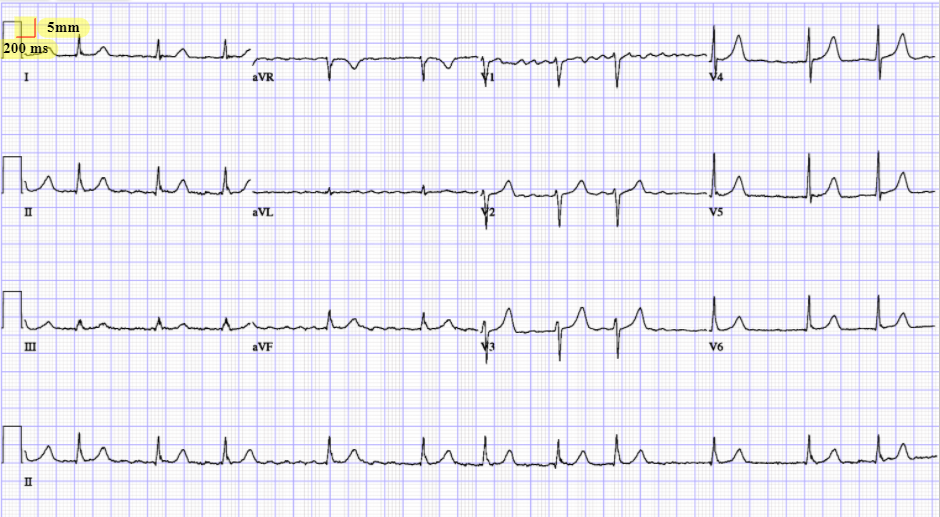
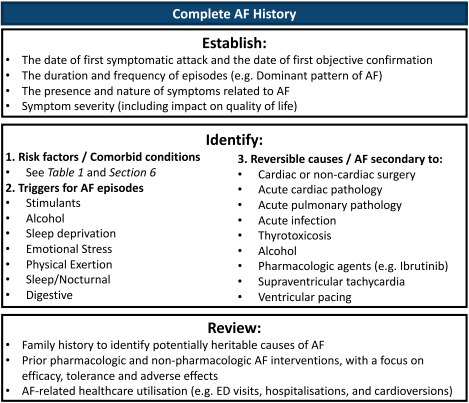
You are seeing her in clinic for new onset of palpitations while waiting for TAVI and Holter monitor shows atrial fibrillation. How will you manage her new diagnosis?
CCS always wins. CCS Afib 2020:
"The current definition of “valvular AF” is limited to AF in the presence of any mechanical heart valve, or in the presence of moderate to severe mitral stenosis (rheumatic or nonrheumatic)."
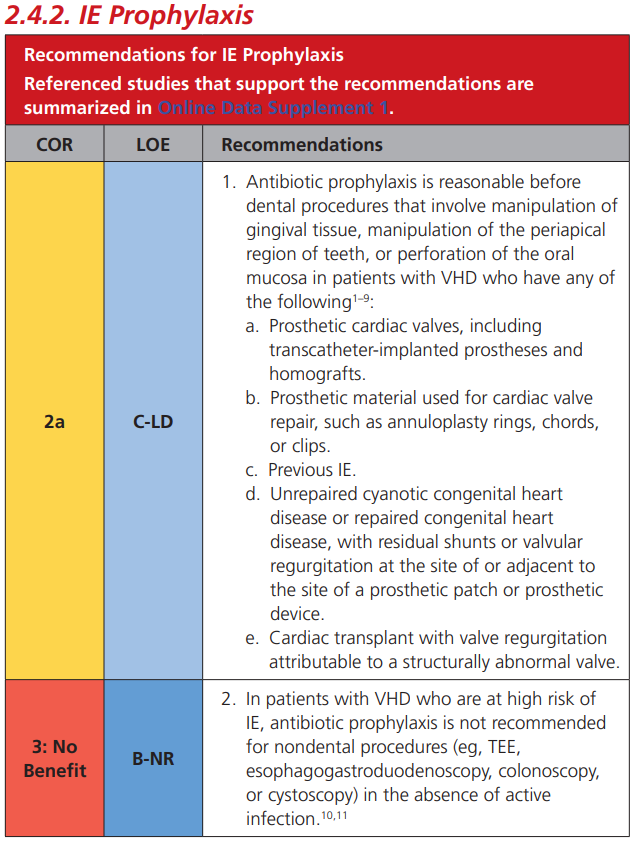
You are seeing her in clinic 1 year after her TAVI and he remembers the TAVI coordinator saying something about antibiotics before certain procedures. How will you counsel her?
You are seeing a 68 year old male in the emergency medicine department who presents with anxiety. His brother developed atrial fibrillation and he is wondering whether he should have screening. How do you counsel him and if screening is appropriate how would you do so?
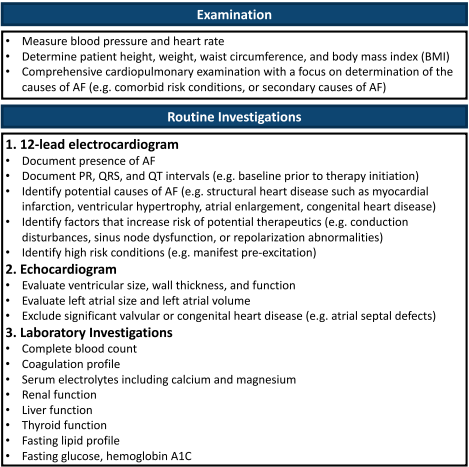
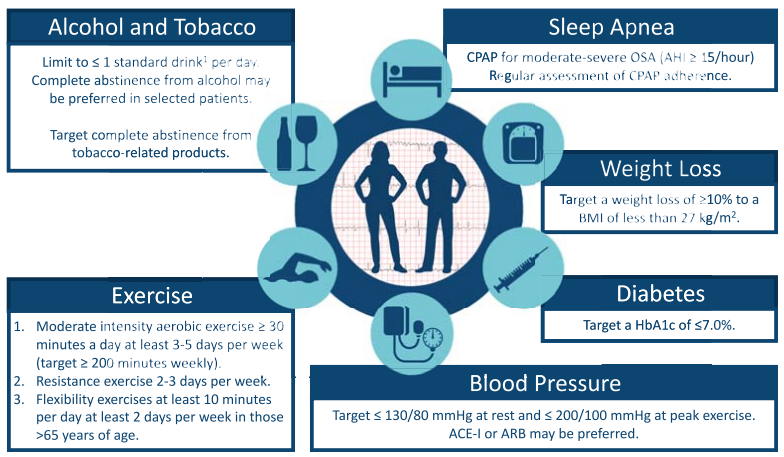
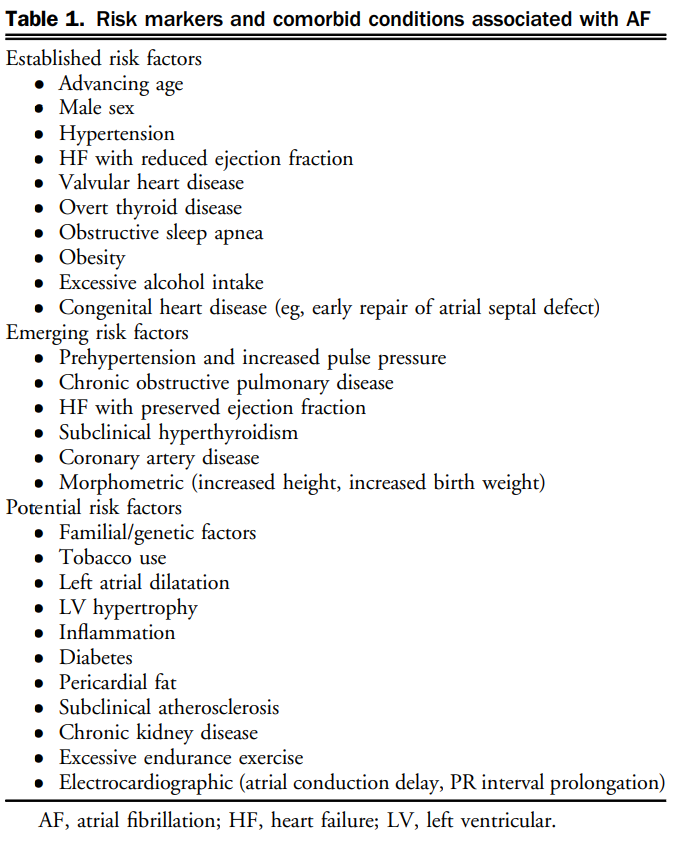
What are risk factors for atrial fibrillation and how would you counsel the patient on modifying them?
We suggest a structured, integrated, multidisciplinary, patient-focused approach to care should be implemented for patients with AF (Weak Recommendation; Moderate-Quality Evidence).
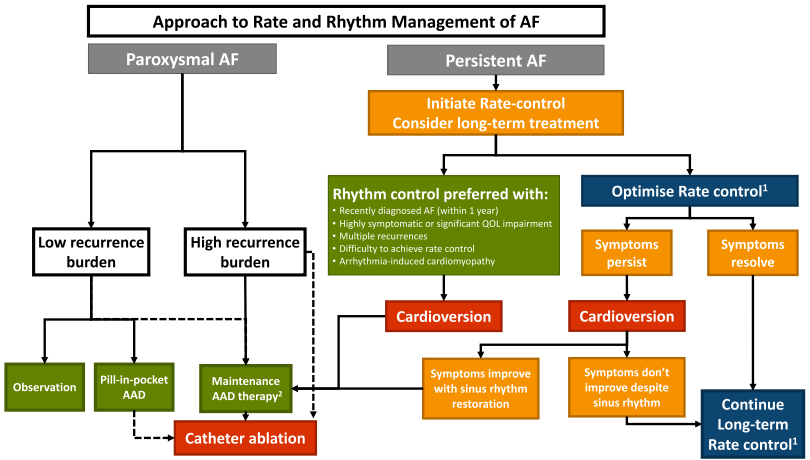
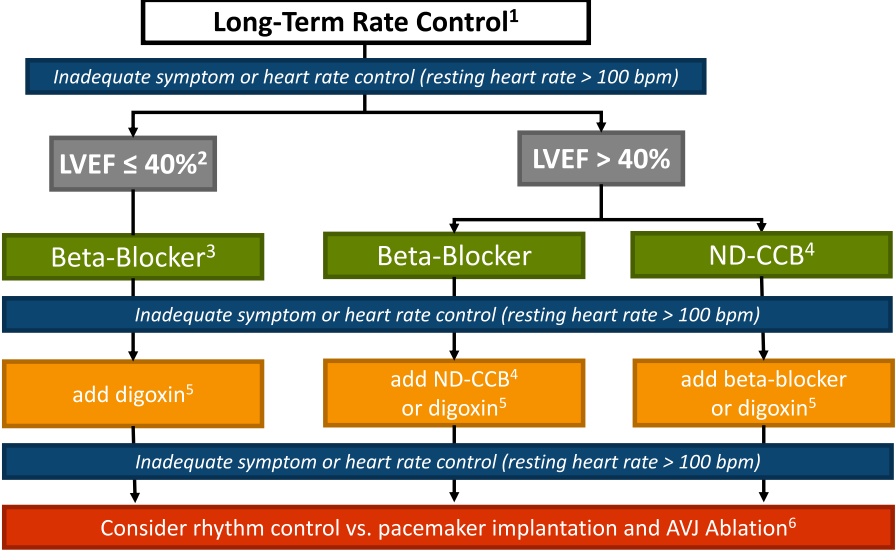
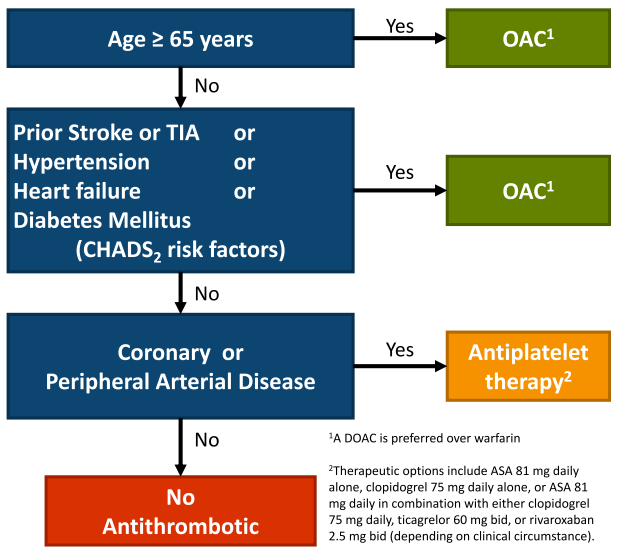
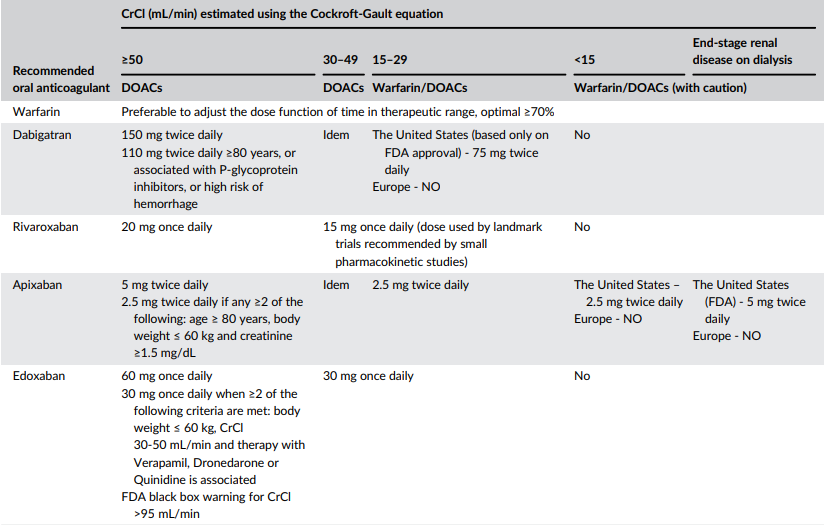
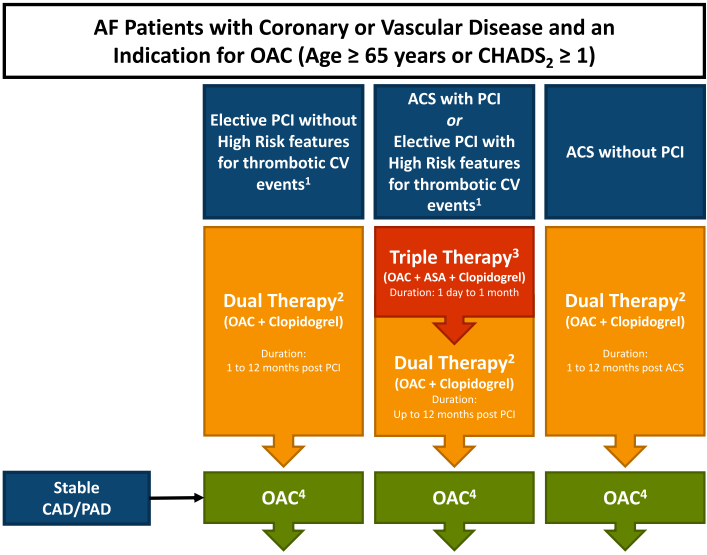
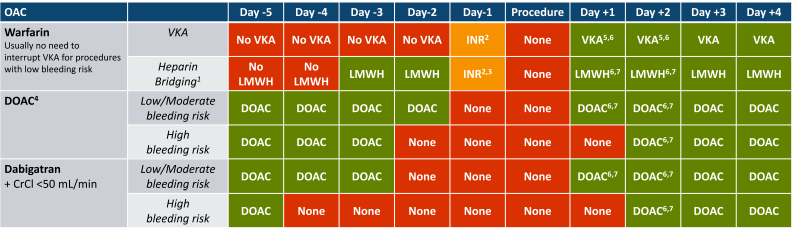
You have initiated a multi-disciplinary non-pharmacologic plan for the patient and now move to the pharmacologic component. How will you manage this patient?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6671778/
Dual: warfarin, apixiban 5mg, dabigatran 110/150, edoxaban 60, rivaroxaban 15
Triple: warfarin INR 2-2.5, rivaroxaban 2.5, apixaban 5 (DOAC preferred)
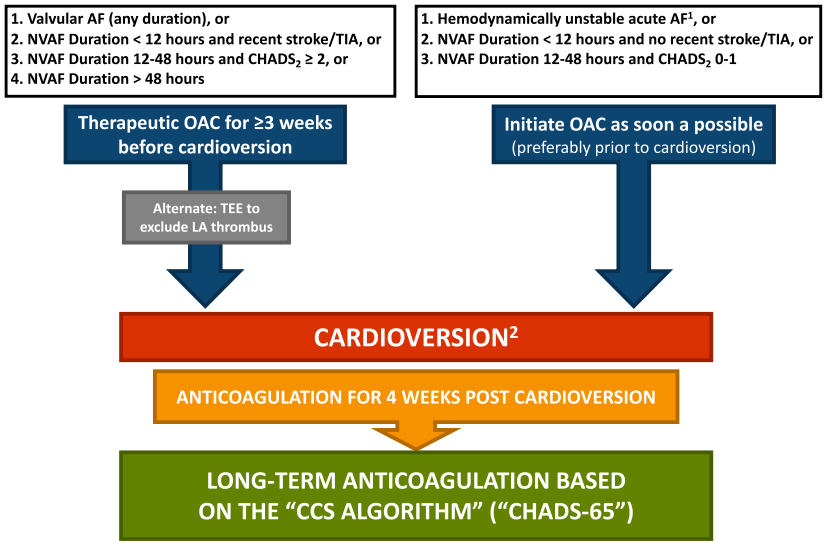
Patient comes back to the emergency department with rapid atrial fibrillation. He is hemodynamically stable. Emergency medicine doctors asks if it is safe to cardiovert. His CHADS65 score is 2 and the symptoms clearly started 16 hours ago. How would you proceed?
By Atul Jaidka
Valve/Afib



