
Atul Jaidka PRO
Cardiologist | Unity Health - St. Joseph's Hospital
Serum
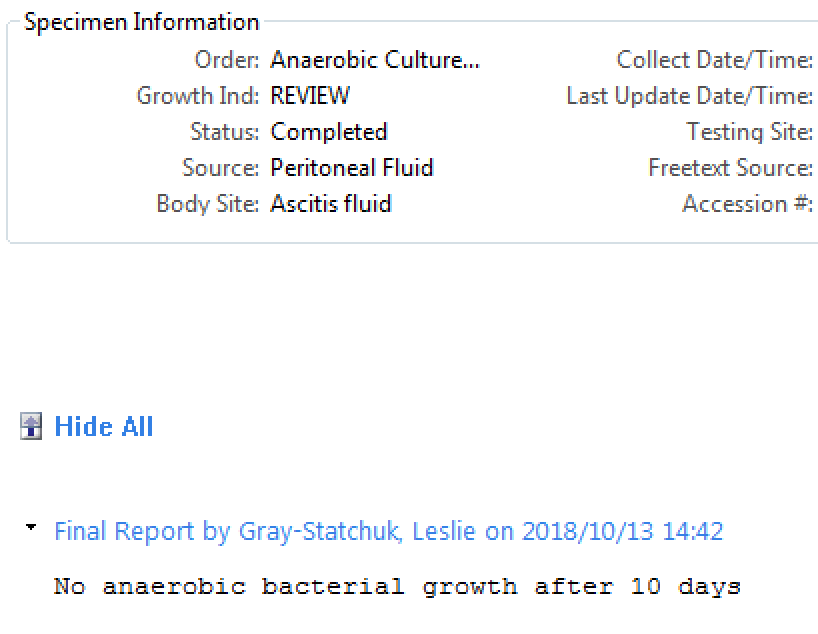
Pleural Fluid (straw coloured)
Other tests:
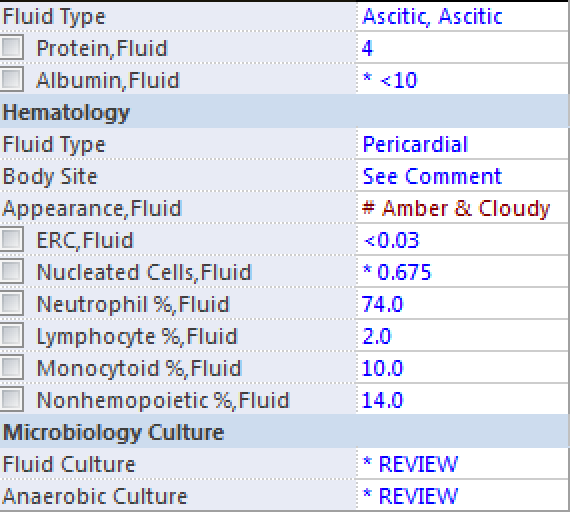
drainage frank pus/cloudy
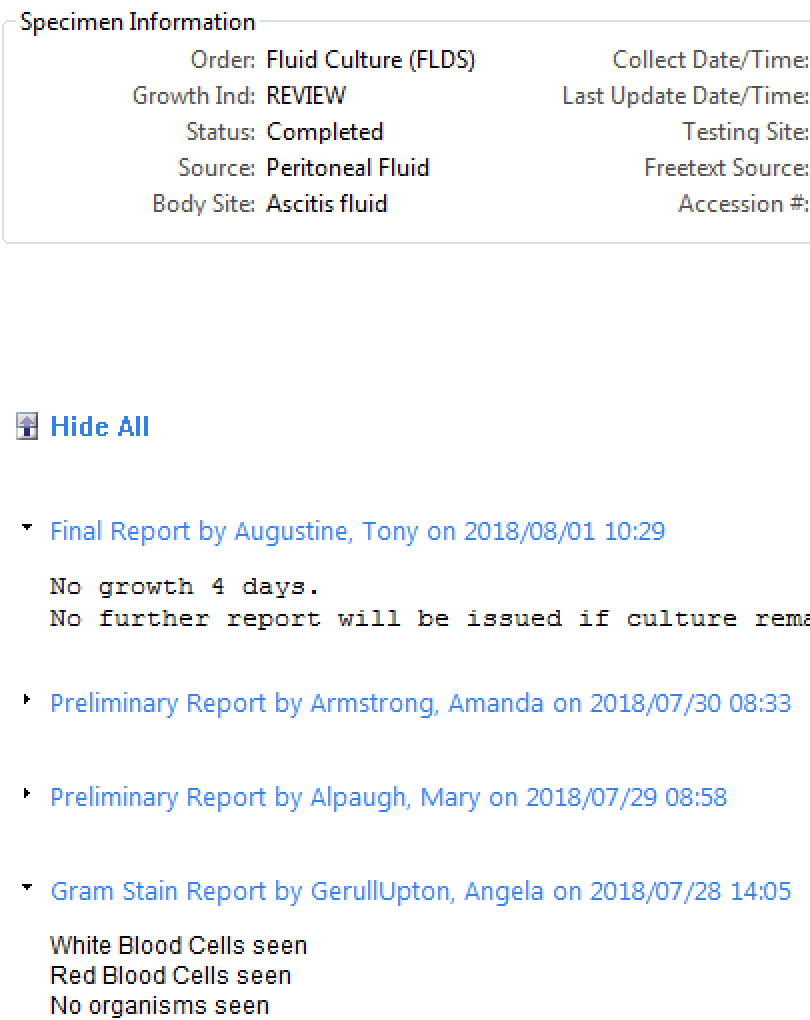
positive gram stain or culture
pH <7.2 (if unavailable use glucose <3.4 mmol/L)
loculations on imaging
Diagnosis and most common cause?
Text
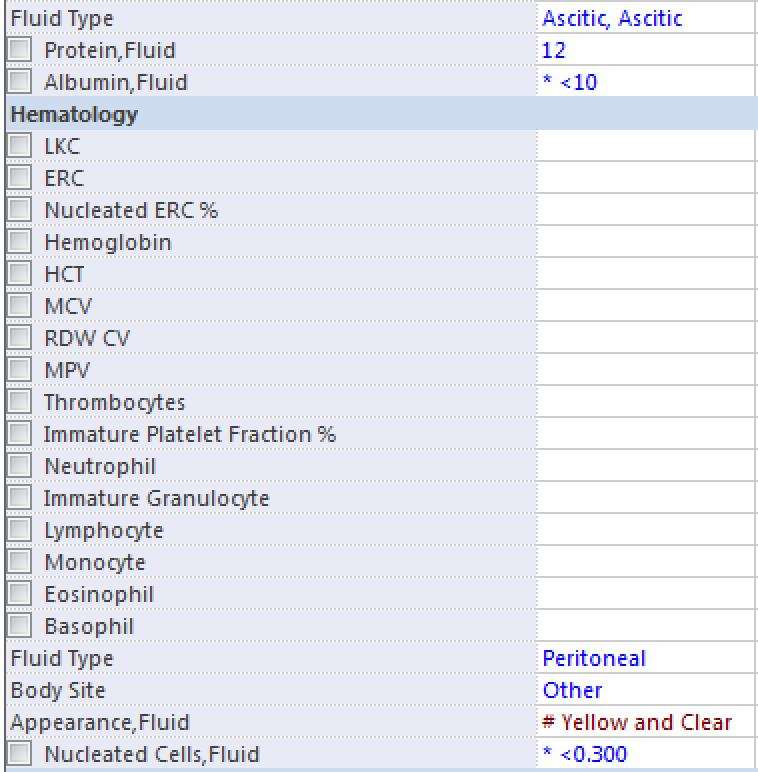
Bonus points: His albumin is 23, portal hypertension present?
Norfox or Cipro or Septra
https://www.aasld.org/sites/default/files/guideline_documents/adultascitesenhanced.pdf
https://aidsinfo.nih.gov/guidelines/html/4/adult-and-adolescent-opportunistic-infection/354/primary-prophylaxis
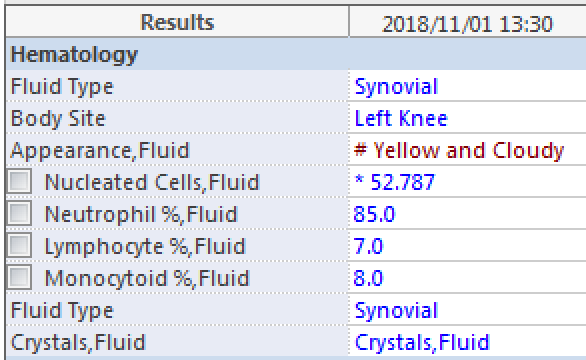
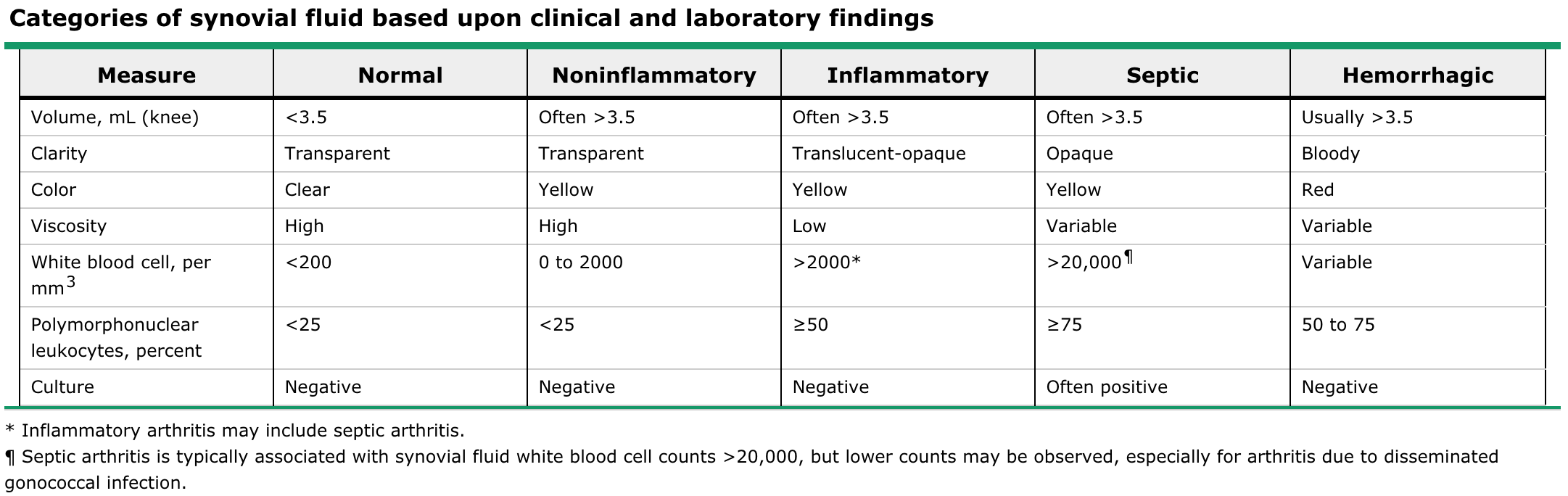
Synovial fluid is usually purulent, with typical leukocyte count of 50,000 to 150,000 cells/mm3 (most of which are neutrophils)
| Tube # | 2 |
|---|---|
| Appearance | clear & colourless |
| Glucose | 1.7 (2.2-3.9) |
| Protein | 500 (200-400) |
| Tube # | 1 |
| Appearance | slight pink & clear |
| Nucleated Cells | 400 (0-5) |
| Erythrocyte | 6 |
| Tube | 4 |
| Appearance | clear & colourless |
| Nucleated Cells | 400 (0-5) |
| Erythrocytes | 1 |
| Neutrophil % | 35 |
| Lymptocyte % | 65 |
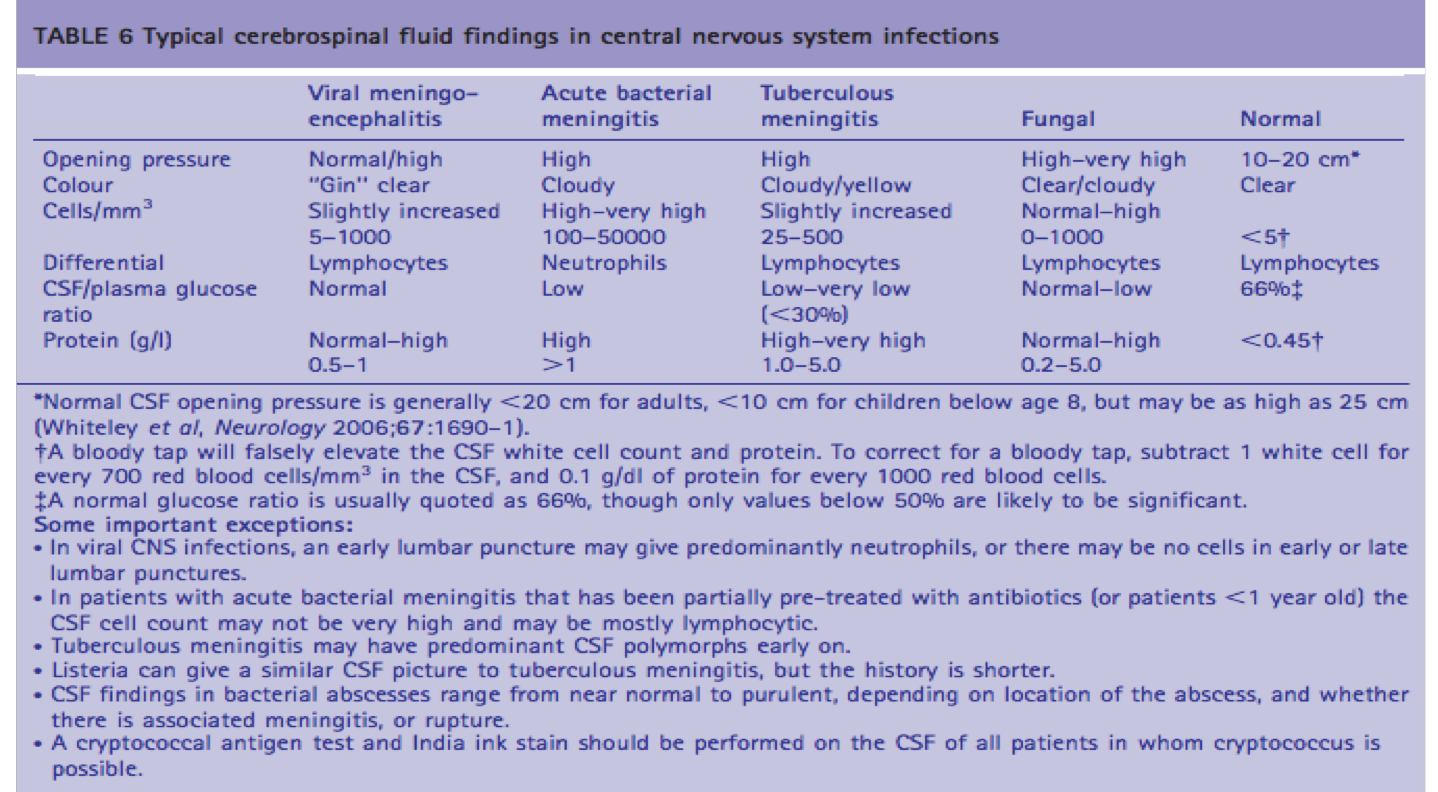
Patients with tuberculous meningitis are categorized by stage on presentation, based upon mental status and focal neurologic signs as follows:
•Stage I patients are lucid with no focal neurologic signs or evidence of hydrocephalus.
•Stage II patients exhibit lethargy, confusion; they may have mild focal signs, such as cranial nerve palsy or hemiparesis.
•Stage III represents advanced illness with delirium, stupor, coma, seizures, multiple cranial nerve palsies, and/or dense hemiplegia.
INH (isoniazid) + RMP (Rifampin) + PZA (Pyrazinamide) + EMB (Ethambutol)
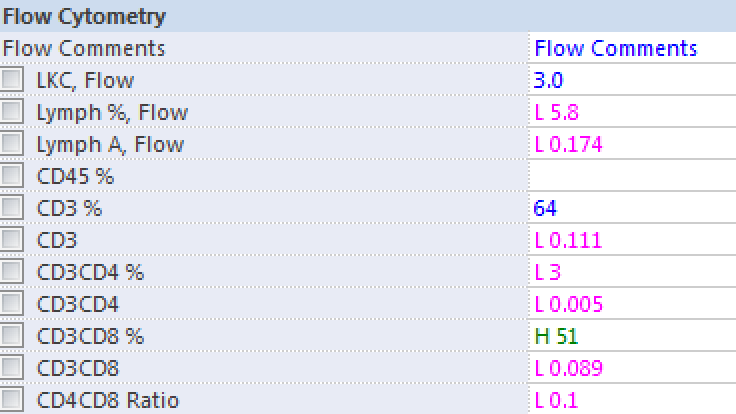
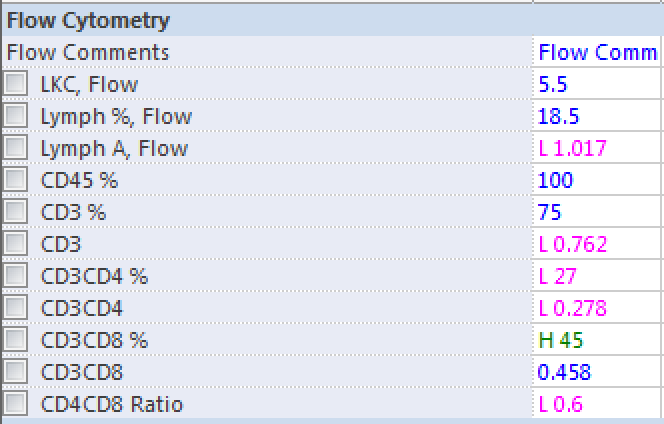
Lymphocyte
Predominant
By Atul Jaidka
Diagnostic Rounds 2049



